Download presentation
Presentation is loading. Please wait.

1
Litigation in Obstetrics and Gynaecology: “Situational Awareness” and “Root Cause Analysis” Professor Dilly OC Anumba, LLM (Medical Laws) Academic Unit of Reproductive & Developmental Medicine Department of Human Metabolism University of Sheffield Sheffield
 Academic Unit of Reproductive & Developmental Medicine Department of Human Metabolism University of Sheffield Sheffield")
2
Outline The economic and medicolegal burden of litigation in Obstetrics and Gynaecology Trends in litigation “Situational awareness” - prevention “Root Cause Analysis”- reflection/prevention Any evidence that risk management works? Future trends

3
Pattern of Obstetric and Gynaecologic Litigation

4
Litigation trends and incidence Maternity claims - highest value and second highest number of clinical negligence claims reported to the NHS Litigation Authority (NHSLA) Between 1st April 2000 and 31st March 2010 – 5,087 maternity claims – Total value of claims £3.1 billion. – For 5.5 million births in England, < 0.1% subject of a claim

6
Total number and value of maternity claims by financial year as at 31 st March 2010 For settled maternity claims, average time from incident to claim resolution - 4.32 years. For claims with damages above £1 million, average time from incident to resolution - 8.57 years, usually more complex cases.

7
Claim categories Three most frequent categories of claim: – management of labour (14.05%) – caesarean section (13.24%) – cerebral palsy (10.65%). Cerebral palsy and management of labour, including CTG interpretation, accounted for 70% of total value of all maternity claims

8
Practitioner experiences Alderman B Litigation in obstetrics and gynaecology has increased in Merseyside. BMJ 1997; 314 doi: http://dx.doi.org/10.1136/bmj.314.7080.607 (Published 22 February 1997) Cite this as: BMJ 1997;314:607.1 From 1 Jan to 31 Dec 1995 I spent 110.5 hours of time dealing with litigation issues (correspondence, reports to solicitors, interviews, etc) - about 3 working weeks. The majority of time in the evenings and weekends, not paid for by the NHS. If all 5 consultants spent roughly equivalent time dealing with their own litigation cases this would amount to about 550 consultant hours a year in department alone-equivalent to 16 working weeks of consultant time a year.
 Cite this as: BMJ 1997;314:607.1 From 1 Jan to 31 Dec 1995 I spent hours of time dealing with litigation issues (correspondence, reports to solicitors, interviews, etc) - about 3 working weeks. The majority of time in the evenings and weekends, not paid for by the NHS. If all 5 consultants spent roughly equivalent time dealing with their own litigation cases this would amount to about 550 consultant hours a year in department alone-equivalent to 16 working weeks of consultant time a year..")
9
Practitioner experiences Litigation in Department January 1995 -106 cases January 1996 - 146 cases, an increase of 38%. Support staff spend time and huge effort in managing complaints and litigation. Cost to taxpayers massive. Full time risk management and legal teams

10
DEALING WITH THE LITIGATION BLACK HOLE THROUGH SITUATIONAL AWARENESS AND ROOT CAUSE ANALYSIS

11
Situational awareness Definition: “the perception of elements in the environment within a volume of time and space, the comprehension of their meaning, and the projection of their status in the near future.” – Assess and become aware of relevant factors in the current environment – Consider any implications of these factors – Foresee future consequences “Knowing what is going on around you”.

12
Aviation example Aviation industry Highly reliable Enviable record of safety – standardisation of process – unfailing use of checklist-driven protocols to govern behaviour in high-risk situations – Crew resource management National Transportation Safety Board Press release SB-05-09. Washington (DC): March 29, 2005. Degani Cockpit checklists: Concepts, design and use. Hum Factors1993;35:28-43.
: March 29, Degani Cockpit checklists: Concepts, design and use. Hum Factors1993;35:")
13
Elements of a clinical Patient is part of the environment Environment is the setting Task is the clinical encounter the treatment Time is the context in which the treatment is to be meted out.

14
The clinical situation elements

15
Loss of situational awareness Loss of sight of the bigger picture – Personae involved became highly focussed on repeated attempts of a procedure

16
The Process of Situational Awareness and Assessment

17
Situational awareness activities Get information Understand information Think ahead Comprehend or assign meaning to information Compare Critique Diagnose Comprehend or assign meaning to information Compare Critique Diagnose

18
Maintaining Situational awareness The key is concentration Discover and Recover – Discover potential situational awareness loss, and recover it by getting more information, understanding it, and thinking ahead Communication

19
Situation, Background, Assessment, Recommendation (SBAR) Description SBAR provides a structured method for communicating critical information about patients. Benefits Contributes to effective escalation of intervention in patient care. Increases patient safety.

20
Situation, Background, Assessment, Recommendation (SBAR) Enhances handovers Can be used for urgent and non-urgent communication
 Enhances handovers Can be used for urgent and non-urgent communication")
21
Situation, Background, Assessment, Recommendation (SBAR) How is it used? SBAR used to clarify information that needs to be communicated between health care professionals by using easy- to-remember mechanism that is used to frame the conversation

22
Situation, Background, Assessment, Recommendation (SBAR) Health care professionals structure their conversation around: S - the situation of concern/discussion B - the background of the client/patient under review A - an assessment of the client’s/patient’s condition R - the recommendations for immediate and future care.
 Health care professionals structure their conversation around: S - the situation of concern/discussion B - the background of the client/patient under review A - an assessment of the client’s/patient’s condition R - the recommendations for immediate and future care.")
23
Situation, Background, Assessment, Recommendation (SBAR) Tips for use Consult widely with staff to gain co-operation to use the tool. Use SBAR stickers to act as prompts. Structure the ward documentation around the SBAR model. Structure the handovers around the SBAR model. Ensure SBAR is incorporated in teaching sessions and educational programmes/training. Ensure SBAR is incorporated into the communication/operations policy/strategy.

24
SBAR Tools for clinical care

25
What is Root Cause Analysis? (RCA) Process for identifying contributing/ causal factors that underlie variations in performance associated with adverse events or close calls Process that features interdisciplinary involvement of those closest to and/or most knowledgeable about the situation
 Process for identifying contributing/ causal factors that underlie variations in performance associated with adverse events or close calls Process that features interdisciplinary involvement of those closest to and/or most knowledgeable about the situation.")
26
RCA Goals Find out: – What happened? – Why did it happen? – What do you do to prevent it from happening again? – How do we know we made a difference? For details see either: http://vaww.ncps.med.va.gov/RCAtrain.html http://www.patientsafety.gov/tools.html

27
RCA Model Focuses on prevention, not blame or punishment (cornerstone: no one comes to work to make a mistake or hurt someone) Focuses on system level vulnerabilities rather than individual performance - Communication - Environment/Equipment - Training - Rules/Policies/Procedures - Fatigue/Scheduling - Barriers
 Focuses on system level vulnerabilities rather than individual performance - Communication - Environment/Equipment - Training - Rules/Policies/Procedures - Fatigue/Scheduling - Barriers")
28
Overview of Steps Set up inter-disciplinary team (4-6 people) – Those familiar and un-familiar with the process Flow diagram of “what happened?” – Triggering questions to expand this view – Site visits and simulation to augment – Interviews with those involved or those with similar job Resources Root cause/contributing factors developed – Five rules of causation to guide/push the team deep enough – Cause and Effect Diagram, etc
 – Those familiar and un-familiar with the process Flow diagram of what happened – Triggering questions to expand this view – Site visits and simulation to augment – Interviews with those involved or those with similar job Resources Root cause/contributing factors developed – Five rules of causation to guide/push the team deep enough – Cause and Effect Diagram, etc")
29
RCA Contributory factors framework Patient Factors Clinical condition Physical Factors Social Factors Mental/Psych ological Factors Interpersonal relationships Staff Factors Physical issues Psychological Issues Social Domestic Personality Issues Cognitive factors Task Factors Guidelines, Policies and Procedures Decision making aids Procedural or Task Design

30
RCA Contributory factors framework Equipment DisplaysIntegrityPositioningUsability Work Environment Administrative factors Design of physical environment EnvironmentStaffing Work load and hours of work Time Communication Verbal communication Written communication Non verbal communication Communication Management

31
RCA Contributory factors framework Organisational Organisational structure Priorities Externally imported risks Safety culture Education and Training CompetenceSupervision Availability / accessibility Appropriateness Team Factors Role Congruence Leadership Support and cultural factors

33
EVIDENCE FOR EFFECTIVENESS OF RISK MANAGEMENT STRATEGIES

34
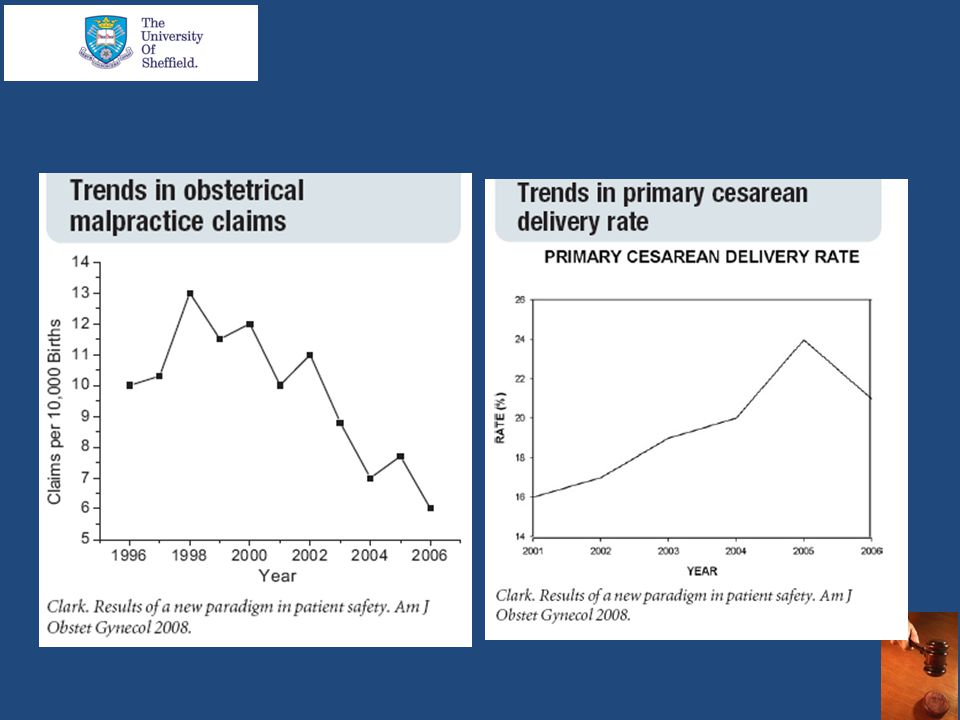
Interventions associated with Improved perinatal outcomes Reduced primary caesarean delivery rate lower maternal and fetal injury Reduced litigation – halving of the number of claims – 5-fold reduction in the cost of claims Clark AJOG 2008;199:105.e1-105.e7.

36
Key interventions in Clark et al 2008 Rigorous guidelines that demonstrate Situation Awareness and SBAR External peer review akin to Root Cause Analysis

38
Conclusion Better patient safety will hinge on improvements in the quality of care, enhanced by best practice in Situational Awareness and Root Cause Analysis, in a cycles of service improvement that inevitably lead to reductions in the burden of litigation

Similar presentations




 Reporting systems are vital in providing a core of sound, representative information on which to base analysis.>")
>")



 Out of Hours Primary Care Outcomes of Service Review Open Meetings Meetings May 2013 Janette Brogan Lead.>")





 of Accidents and Safety Incidents Incident Investigation and Analysis.>")






