Download presentation
Presentation is loading. Please wait.

1
Beacon IC 3 Communities Project From Theory to Practice Association of Utah Diabetes Educators November 4 th, 2011 Korey Capozza, M.P.H. and Sarah Woolsey, M.D.

2
Learning Objectives Describe the Utah Beacon Communities project Review highlights of the Utah Diabetes Practice Recommendations 2011 Introduce Utah Healthscape Introduce mobile health tools being used in the Beacon Communities project Demonstrate the benefits of the Utah Clinical Health Information Exchange for care providers and patients

3
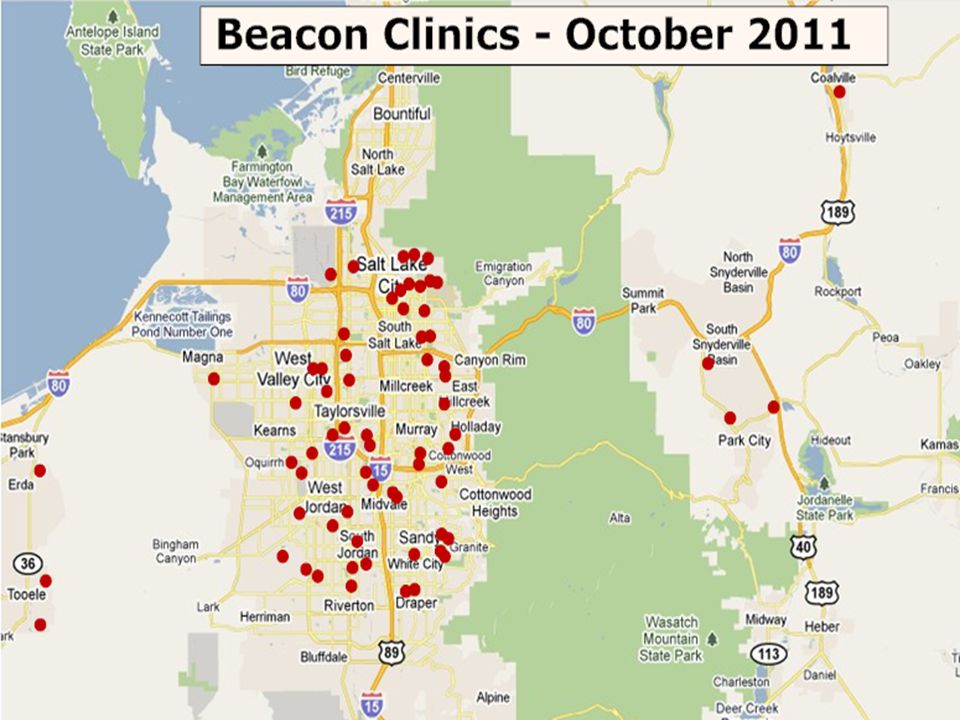
Utah Beacon IC 3 Improving Care through Connectivity and Collaboration 1/17 in the U.S. Project Dates: May 2010 –Mar 2013 GOALS: Utilizing technology, improve health care delivery outcomes while reducing costs Targets: Patients with Diabetes Type II in the Salt Lake MSA, Communicable Disease Reporting, End of Life issues

5
Partners UDOH; Public Health, Epidemiology, Diabetes Program, Vital Records University of Utah Community Clinics Utah Health Information Network Intermountain Healthcare Utah Medical Association Commission on Aging in Utah Community Healthcare Providers

7
More visits needed Colwill J M et al. Health Aff 27:w232 (2008) ©2008 by Project HOPE - The People-to-People Health Foundation, Inc.
 ©2008 by Project HOPE - The People-to-People Health Foundation, Inc..")
8
What is it like in the trenches? More visits/Less Time for visits More diagnoses per patient More medications prescribed More preventive services required More transitions New Technology does not always “fit” Patient outcomes not satisfactory

9
Not just about the technology- Ideal Trained People, Efficient Processes and Easy Tools Data Systems, Structured Data Health Information Exchange Quality Analysis, Interventions Understand Outcomes, Reassess $

10
Not just about the technology- Current State Informal process, Poor Training, Digitized Paper Paper Based Systems, Non- structured Data Fragmented Health Information Exchange Labor Intensive Quality Analysis, Interventions Limited Understanding of Outcomes, Labor Intense Reassessment

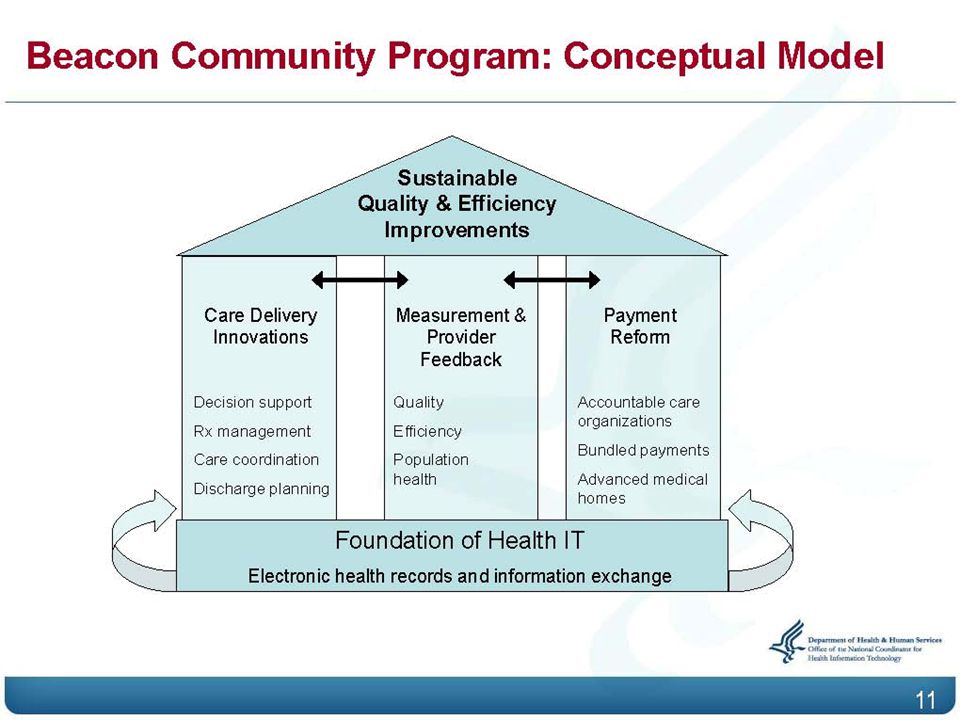
11
Not just about the technology- Ideal Trained People, Efficient Processes and Easy Tools Data Systems, Structured Data Health Information Exchange Quality Analysis, Interventions Understand Outcomes, Reassess

12
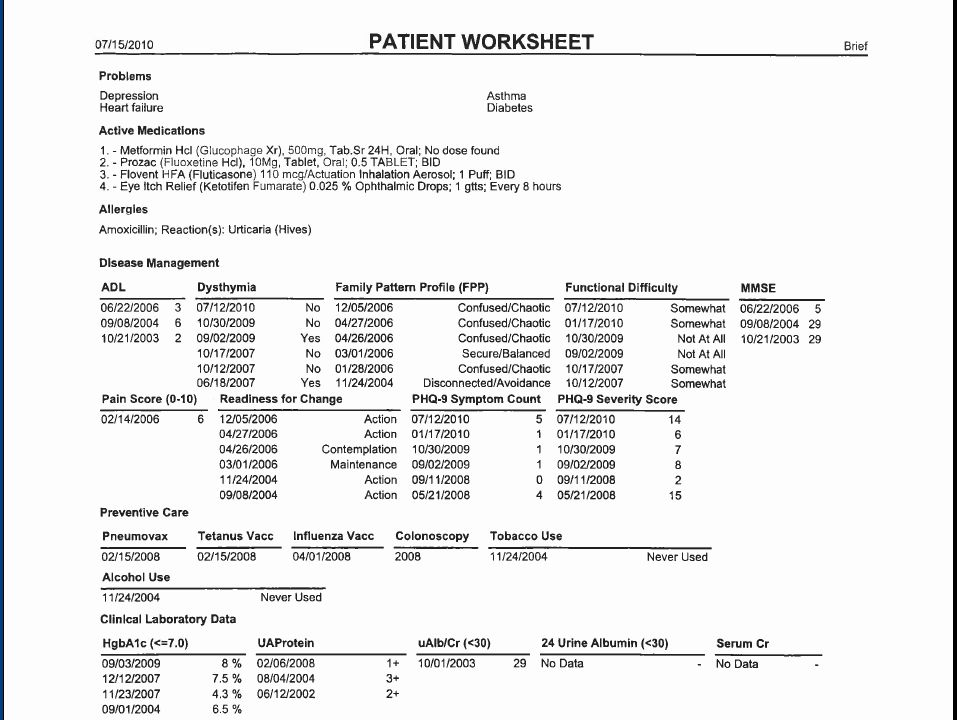
Beacon Utah-who we are Commission on Aging Using web-based technology to connect patients’ end of life wishes to EMTs, ERs, and hospitals Utah Health Information Exchange With UDOH making easier to report communicable diseases through our electronic records Connecting health information for all Utahns and health providers Intermountain Healthcare Making the Patient Worksheet available through Health Information Exchange for DM patients University of Utah Studying effects of patient portal connections and care mangers to improving patient engagement and health

13
Beacon Utah-who we are Clinical Interventions Team 62 Primary Care clinics 330 providers Potential to impact 50,000 patients with Diabetes Eye care specialists-in recruitment YOU

15
Aims of the IC 3 Beacon Community To demonstrate that health IT-enabled quality, cost/efficiency, and population health improvements are possible in diverse communities by 2013. To support lasting innovation networks in our community through which a wide range of stakeholders can continue to collaborate, design, and implement new technology- enabled ideas that improve health care beyond 2013. To provide lessons, implementation insights, and best practices for other communities eager to improve health, health care, and cost-efficiency in their communities.

16
Beacon Clinic Intervention QI Process Select Clinic Provider Champion Designate the clinic QI team Feedback session, review clinical data, Set SMART QI aim Begin PDSA cycle with HI support DATA IC3 Beacon Community cHIE UCIT Learning Sessions Public Health registry HealthScape website Other Beacon Sites State, national political arena Complete assessment with HI coach

18
Population Health Improvement Interventions Performance feedback to providers Provider Reminders Clinical Guideline Use/Dissemination Patient Reminders Care Managers Depression Screening and Treatment Provider Communication Skill Improvement Low cost medications/diabetes products Tailoring care to specific demographics of populations Patient self-management support Diabetes Educator Availability

19
Authored by a multidisciplinary panel Resources for providers and patients http://health.utah.gov/diabetes/diabetesprac ticerecommendations/udpr.htm http://health.utah.gov/diabetes/diabetesprac ticerecommendations/udpr.htm Utah Diabetes Practice Recommendations Diabetes Management for Adults 2011

20
What’s New in 2011 Diabetes screening protocol – Clarifies the role of A1C in diagnosis Cardiovascular disease – Addresses the controversy concerning ASA New insulin protocols for type 2 diabetes Updated medication summary New sections – Depression and vaccinations New tools – Active links, referral forms, CKD management, updated protocols for lipids, extensive references and blood pressure management

21
Key Treatment Targets UDPRs, 2011

22
Initiating a Basal Insulin Page 12, UDPR for Adults 2011

23
UDPR Appendices Comprehensive foot examination form Foot care information for patients Medication summaries CKD management Referral form for eye examination Tobacco quit line information Healthy eating tips for patients Glucose monitoring State certified self management programs, topics covered and when to refer patients Vaccination guidelines Diabetes and depression

24
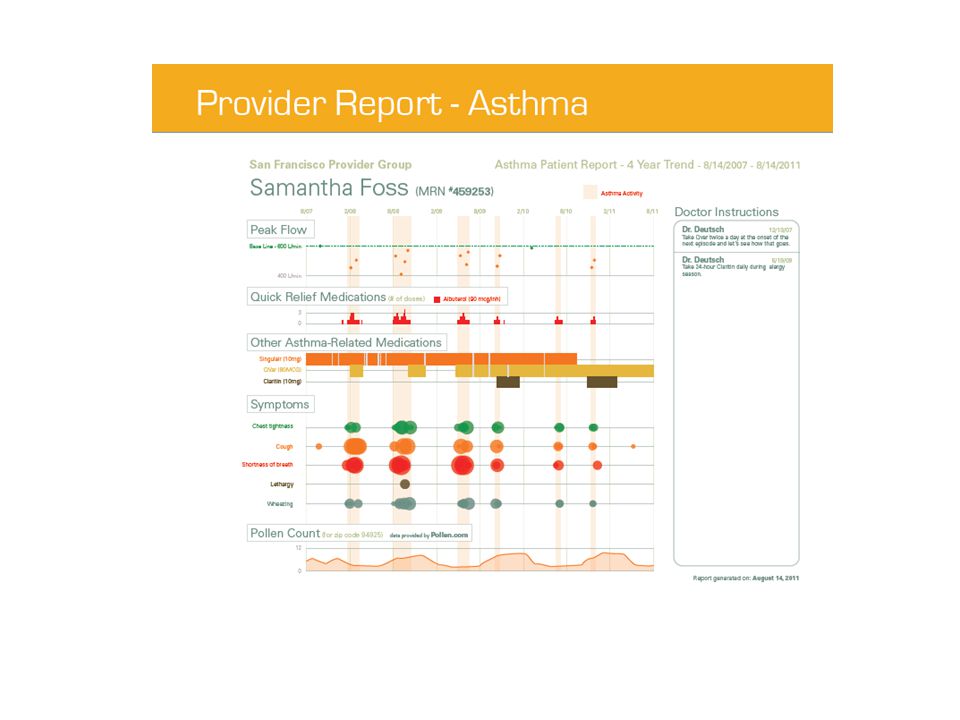
Intermountain Diabetes Worksheet

27
Utah Beacon Consumer Engagement

29
In the Clinic Outside the Clinic A ratio problem: 1% to 99% How can we support patients beyond the physician office to improve self care and diabetes management? “Look, it’s very simple: Lose weight, take your meds, stop smoking, eat right…and try not to be so depressed about it.” Easy, right? Great, see you in six months! ?

30
Behavior Change: The $3 Trillion Dollar Question How can we leverage technology to help patients change behaviors? How can we improve health care decision making – from choice of a health plan to daily self-care practices?

31
Beacon Patient Engagement Tools Performance reporting Web site Support patient healthcare decision making Diabetes tracking Web tools Organize, simplify care regimens Provide ongoing, data-driven feedback to pt Improve self-tracking and focus on improvement Smartphone innovations Can we make tracking and self management fun??? Mobile Health “Care Manager-lite” Cost-effective Address health disparities

32
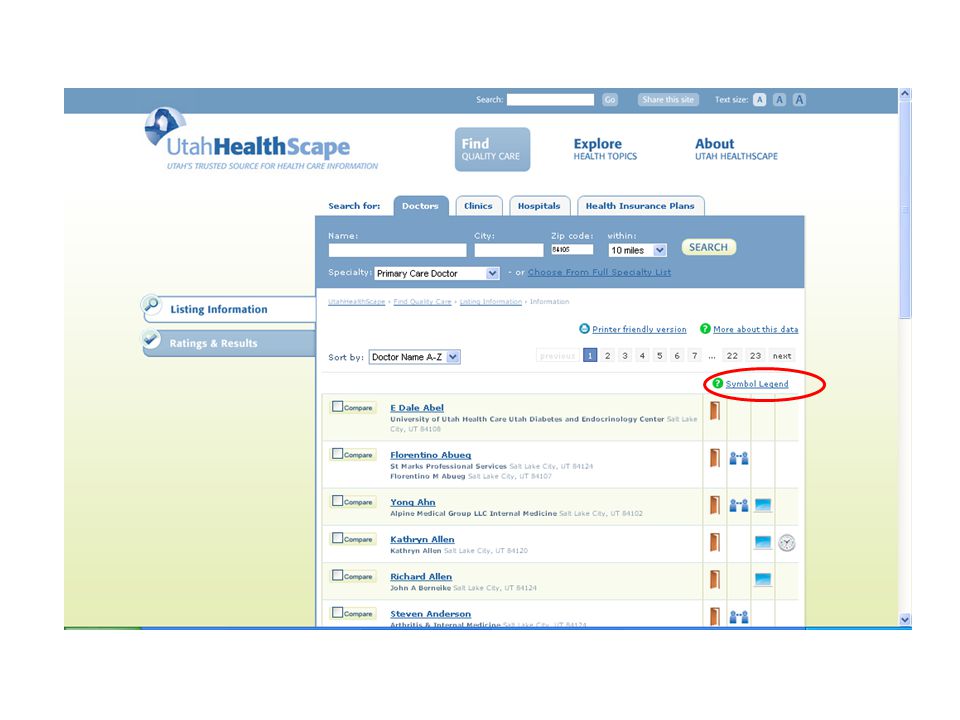
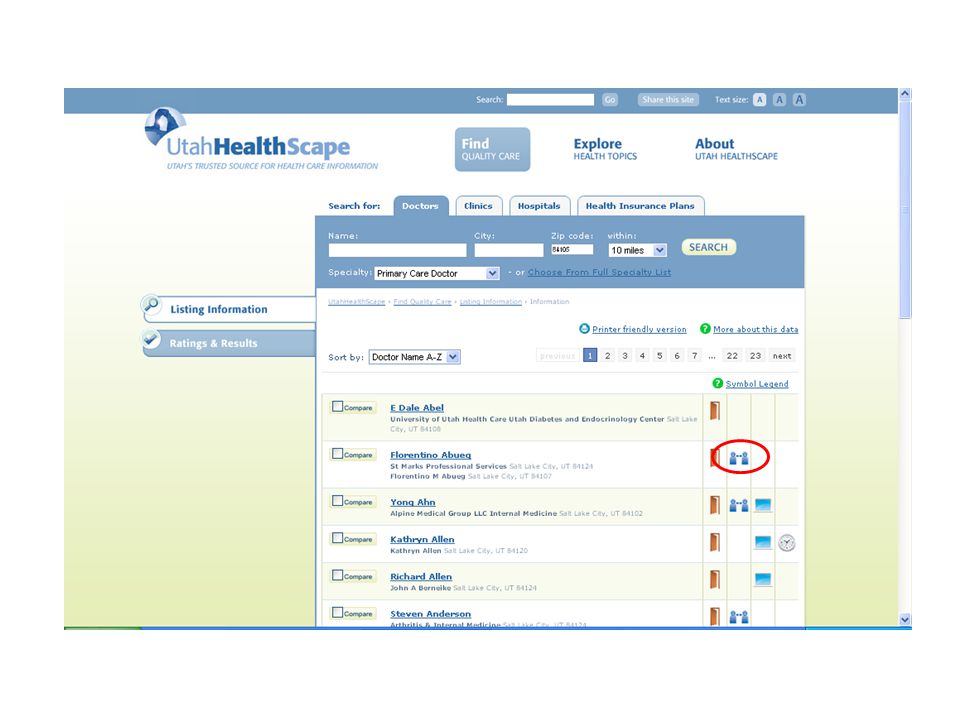
Utah HealthScape Patient decisions about health plans and providers impact the care they receive and the system they receive it in Goal: To develop a consumer-directed website Educates consumers about quality variation; Helps consumers find and demand high quality care Increases competition, accountability to consumers of healthcare, and lowers costs Motivates consumers to advocate for public reporting on nationally- recognized indicators of quality care

35
“I need to find a Spanish-speaking doctor in my area.”

43
“My husband and I work full time. We need an eye clinic with extended hours.”

46
Multi-Channel Health Tracker A Beacon primary care clinic requested our help in designing an online patient tool to help with self- management Health 2.0 invitation to meet with health care technology start-ups We met “The Carrot”

48
Health Tracking Support

49
EMR Integration

51
Social Media Component

52
Integrated “App”

53
Mobile Phone Tools

54
Utah Department of Health Program, co- branded with Utah Beacon Studies: Text messaging support can double the quit rate. Free and available now to any patient in Utah. Free C, Knight R, Robertson S, et al. Smoking cessation support delivered via mobile phone text messaging (txt2stop): a single-blind, randomized trial. Lancet 2011;378(9785):49-55.
: a single-blind, randomized trial. Lancet 2011;378(9785):")
55
Text to Quit Smoking increases the risk for Type 2 diabetes and makes it harder to manage Text to Quit = text messaging service that offers patients daily tips to help get through the quitting process Used in Utah since 2009 Content developed by New Zealand government

56
Text to Quit (cont’d) Messages both encourage and educate participants how to manage day-to-day stresses associated with quitting and offers useful tips for avoiding triggers and controlling cravings Free and available across cellular networks 2 messages per day x 21 days (one way) For Beacon partnership, tracking reported outcomes at exit
 Messages both encourage and educate participants how to manage day-to-day stresses associated with quitting and offers useful tips for avoiding triggers and controlling cravings Free and available across cellular networks 2 messages per day x 21 days (one way) For Beacon partnership, tracking reported outcomes at exit")
57
Your Turn

58
hLog For Diabetes

59
Confidential

60
How is it Different? Users cannot track all metrics from day one They have to achieve mastery of simple tracking Unlock higher levels to track multiple metrics Compete with other diabetics to be on time in tracking and medication Confidential

61
Features Users start with blood sugar tracking to earn yellow belt Consistently track once a day to earn green stripe Goal is to reach black belt where they track blood sugar, insulin, carbs and exercise Confidential

62
Badges and Milestones Users earn badges for continuous tracking They can share these on Facebook and Twitter for motivation Signing up beta testers: See me if you are interested Confidential

64
Rationale Diabetes education and care management have been shown to improve patient engagement and self-care activities mHealth may be able serve this function at much lower cost, thus increasing access to care management services Cluster-Randomized Trial, Mobile Coaching – University of MD, 163 patients, 1 year – Showed 1.9% HbA1c reduction vs 0.7% in usual control (p>0.001) C. C. Quinn, M. D. Shardell, M. L. Terrin, E. A. Barr, S. H. Ballew, A. L. Gruber- Baldini. Cluster-Randomized Trial of a Mobile Phone Personalized Behavioral Intervention for Blood Glucose Control. Diabetes Care, 2011

65
Care4Life Adapted from 2 systems deployed in Mexico Interaction is customized and two-way. “Pocket care manager”. Developed with content from the National Institutes of Health and the Centers for Disease Control and Prevention Testing in 66 Beacon clinics Implementation and Evaluation Sept. 2011-Dec. 2012 Received IRB approval October 2011 Preparing to sign up clinics in November 2011

66
Tailored to IndividualTargeted MessagesTargeted Med and App. RemindersPersonal Health Portal Key Features

67
Personal Web Portal Manage Subscriptions Exercise Progress Weight Loss Progress Medication Adherence Glucose Readings Medication Reminders Appointment Reminders

68
68 a)User can set glucose reminders according to their doctor’s recommendations (i.e. before breakfast daily) b)System sends glucose reminders & provides immediate feedback c)User can track all glucose recordings on web portal d)System sends education messages & tips Care4Life | Increase Blood Glucose Monitoring Care4Life. Reminder: Time to check your BEFORE meal glucose. Reply with your BEFORE meal glucose reading (e.g. 125). Care4Life. Before meal readings under 70 can be dangerous. Do you know what to do when readings fall below your target? Text LOW for more info Glucose recordings graph on web portal Glucose reminderSystem feedback
 b)System sends glucose reminders & provides immediate feedback c)User can track all glucose recordings on web portal d)System sends education messages & tips Care4Life | Increase Blood Glucose Monitoring Care4Life. Reminder: Time to check your BEFORE meal glucose. Reply with your BEFORE meal glucose reading (e.g. 125). Care4Life. Before meal readings under 70 can be dangerous. Do you know what to do when readings fall below your target. Text LOW for more info Glucose recordings graph on web portal Glucose reminderSystem feedback.")
69
Things you can do now 1.Tell your patients about Text to Quit 2.Check out www.UtahHealthscape.org 3.Tell me if you or someone you know would like to be a beta tester for hLog 4.kcapozza@healthinsight.org 5.Attend our Learning Session, November 10th

70
Clinical Health Information Exchange (CHIE) PROVIDERS E-prescribe E-referrals to any other participating cHIE clinician Electronically order and deliver reports Share with other cHIE clinicians through the Virtual Health Record (VHR) Hospital reports Lab results Medication histories Allergies Clinician documents Patient Worksheet PATIENTS Patient consent required All or Emergency options Free Recommended for Chronic Conditions Multiple medications Children (vaccination records) Anyone
 PROVIDERS E-prescribe E-referrals to any other participating cHIE clinician Electronically order and deliver reports Share with other cHIE clinicians through the Virtual Health Record (VHR) Hospital reports Lab results Medication histories Allergies Clinician documents Patient Worksheet PATIENTS Patient consent required All or Emergency options Free Recommended for Chronic Conditions Multiple medications Children (vaccination records) Anyone")
71
Clinical Health Information Exchange (CHIE) Data Source(s) General Lab Micro Reports Radiology Reports Transcription Reports Medication History Brigham City Community Hospital 10/2010 8/20106/2010 Central Utah Clinic1/2010 Lakeview Hospital8/20112/2011 Medicaid1/2010 Moab Regional Hospital8/2009 Mountain View Hospital 3/20112/2011 Ogden Regional Hospital 8/20112/2011 PAML5/2011 St. Marks Hospital8/20112/2011 Timpanogos Hospital3/20112/2011

72
Not just about the technology- Ideal Trained People, Efficient Processes and Easy Tools Data Systems, Structured Data Health Information Exchange Quality Analysis, Interventions Understand Outcomes, Reassess

73
June 22, 2011

Similar presentations



















 & Medical Center Hospital Partnerships.>")




>")








- PBHCI Washtenaw Community Health Organization Cohort-II-III Learning Community Region 4 Ypsilanti, Michigan.>")
 is a Mobile phone and.>")