Download presentation
Presentation is loading. Please wait.

1
Best Practices in Disease Management
Deanna Bell, M.D., F.A.A.P. Medical Director, MHIP Tennessee Chapter of the American Academy of Pediatrics

2
Goals of D70 Grant “ to improve medical home provision for children and youth with special healthcare needs by promoting systems and service integration for children through education of parents and providers on medial home concepts of team-based care, care coordination, and disease management.”

3
Who are Your CYSHCN? To be able to institute evidence-based protocols and management of high risk patients, you must have a system of identification of them. 82% are under 200% of the FPL 78% are fully covered or supported by Medicaid 54% do not have access to a medical home 12% have no usual source of care 61% had access to care coordination when needed 23% had any help arranging or coordinating care Top 10% most costly children lead to 70% of pediatric medical expenditures. 49% of top decile in 2000 were in the top decile in 2001. Cost Predictors: older age special needs functional limitations higher psychosocial morbidity

4
MOC QI Aim #3 ----------------------------------------- High Risk Registry Formation
One of the measurable goals of this MOC project is to have practices form a registry of the children and youth with special healthcare needs they care for. Since the care of this group is what we are trying to impact, it is important that we review how we are defining this cohort.

5
Ways to ID CYSHCN Screeners (CSHCN Screener, QuICCC, QuICCC-R)
ICD-9 lists (NHIS, CAHMI, NDP) Administrative with risk stratification (3M-CRG) Physician Referral Payer referral Pharmacy utilization
 Administrative with risk stratification (3M-CRG) Physician Referral. Payer referral. Pharmacy utilization.")
6
Administrative: 3M CRG Combines Dx and consequences based approaches
Uses ICD-9 and procedural codes to classify cases Requires:6 months of claims data 2 or more encounters with same Dx code Takes into account: type and number of Dx, recurrences, number of acute exacerbations, cost/type/combination/frequency of services Strengths: identifies population and individuals; assigns severity rating; assigns groupings: ICD-9 self explanatory healthy/acute/chronic

7
Survey-based Methods QuICCC: 41 question survey sequence
QuICCC-R: 16 question survey sequence CSHCN Screener: 5 questions survey sequence All do not require formal Dx All 3 part sequence: consequences/presence of condition/duration Qualify if positive answers to one or more sequences All identify population cohorts and can identify individuals QuICCC and QuICCC-R: interviewer administered only QuICCC: questionnaire for Identifying Children with Chronic Conditions-Revised CSHCN Screener: Children with Special Health Care Need Screeners CSHCN Screener can be filled out by parent, mailed. Etc.

8
Comparison of Administrative and Survey-based methods
Of CSHCN identified by ICD-9 lists Only 52-53% met CSHCN criteria by survey methods Of CSHCN identified by Survey Methods 20-24% were not identified by ICD-9 lists Concordance between CRG/CSHCN Screener/QuICCC-R= % This is due to many children with chronic illness not having an official diagnosis

9
CSHCN identified by Survey and not by Administrative data are likely to:
Have developmental or emotional disorders not coded in encounter records Use services not reimbursed under benefit structure Have multiple health issues that include a range of educational, developmental, and mental health service needs and consequences Be in transition between health plans or PCPs #2 This is why including those who screen positive for barriers to compliance should be included

10
MCHB/AAP definition CYSHCN
“ those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.” McPherson M, Arrange P, Fox H, et al. “A new definition of children with spe cial health care needs”, Pediatrics, 1998; 102: 137‐140. Consequences-based definition endorsed by MCHB and AAP. For reasons of time, practicality, and concordance between prevailing methods, We suggest the CSHCN Screener be the tool used.

11
Children with Special Health Care Needs (CSHCN) Screener©
non-condition specific, consequences- based identifies children across the range and diversity of childhood chronic conditions and special needs identified on the basis of one or more current functional limitations or service use needs Scoring in based on positive cluster (e.g. 5 and 5a= positive; or 1 , 1a, and 1b=positive) Child and Adolescent Health Measurement Initiative (CAHMI),
 Child and Adolescent Health Measurement Initiative (CAHMI),")
12
Children with Special Health Care Needs (CSHCN) Screener©
1. Does your child currently need or use medicine prescribed by a doctor (other than vitamins)? ٱ Yes Go to Question 1a ٱ No Go to Question 2 1a. Is this because of ANY medical, behavioral or other health condition? ٱ Yes Go to Question 1b ٱ No Go to Question 2 1b. Is this a condition that has lasted or is expected to last for at least 12 months? ٱ Yes ٱ No 2. Does your child need or use more medical care, mental health or educational services than is usual for most children of the same age? ٱ Yes Go to Question 2a ٱ No Go to Question 3 2a. Is this because of ANY medical, behavioral or other health condition? ٱ Yes Go to Question 2b ٱ No Go to Question 3 2b. Is this a condition that has lasted or is expected to last for at least 12 months? ٱ Yes ٱ No 3. Is your child limited or prevented in any way in his or her ability to do the things most children of the same age can do? ٱ Yes Go to Question 3a ٱ No Go to Question 4 3a. Is this because of ANY medical, behavioral or other health condition? ٱ Yes Go to Question 3b ٱ No Go to Question 4 3b. Is this a condition that has lasted or is expected to last for at least 12 months? ٱ Yes ٱ No 4. Does your child need or get special therapy, such as physical, occupational or speech therapy? ٱ Yes Go to Question 4a ٱ No Go to Question 5 4a. Is this because of ANY medical, behavioral or other health condition? ٱ Yes Go to Question 4b ٱ No Go to Question 5 4b. Is this a condition that has lasted or is expected to last for at least 12 months? ٱ Yes ٱ No 5. Does your child have any kind of emotional, developmental or behavioral problem for which he or she needs or gets treatment or counseling? ٱ Yes Go to Question 5a ٱ No 5a. Has this problem lasted or is it expected to last for at least 12 months? ٱ Yes ٱ No See Children with Special Healthcare Needs Screener Handout
 ٱ Yes Go to Question 1a ٱ No Go to Question 2 1a. Is this because of ANY medical, behavioral or other health condition ٱ Yes Go to Question 1b ٱ No Go to Question 2 1b. Is this a condition that has lasted or is expected to last for at least 12 months ٱ Yes ٱ No 2. Does your child need or use more medical care, mental health or educational services than is usual for most children of the same age ٱ Yes Go to Question 2a ٱ No Go to Question 3 2a. Is this because of ANY medical, behavioral or other health condition ٱ Yes Go to Question 2b ٱ No Go to Question 3 2b. Is this a condition that has lasted or is expected to last for at least 12 months ٱ Yes ٱ No 3. Is your child limited or prevented in any way in his or her ability to do the things most children of the same age can do ٱ Yes Go to Question 3a ٱ No Go to Question 4 3a. Is this because of ANY medical, behavioral or other health condition ٱ Yes Go to Question 3b ٱ No Go to Question 4 3b. Is this a condition that has lasted or is expected to last for at least 12 months ٱ Yes ٱ No 4. Does your child need or get special therapy, such as physical, occupational or speech therapy ٱ Yes Go to Question 4a ٱ No Go to Question 5 4a. Is this because of ANY medical, behavioral or other health condition ٱ Yes Go to Question 4b ٱ No Go to Question 5 4b. Is this a condition that has lasted or is expected to last for at least 12 months ٱ Yes ٱ No 5. Does your child have any kind of emotional, developmental or behavioral problem for which he or she needs or gets treatment or counseling ٱ Yes Go to Question 5a ٱ No 5a. Has this problem lasted or is it expected to last for at least 12 months ٱ Yes ٱ No See Children with Special Healthcare Needs Screener Handout.")
13
CSHCN Screener© Grading
All three parts of at least one screener question (or in the case of question 5, the two parts) must be answered “yes” in order for a child to meet CSHCN Screener© criteria for having a chronic condition or special health care need. The CSHCN Screener© has three “definitional domains:” 1) Dependency on prescription medications. 2) Service use above that considered usual or routine. 3) Functional limitations. The definitional domains are not mutually exclusive categories.
 must be answered yes in order for a child to meet CSHCN Screener© criteria for having a chronic condition or special health care need. The CSHCN Screener© has three definitional domains: 1) Dependency on prescription medications. 2) Service use above that considered usual or routine. 3) Functional limitations. The definitional domains are not mutually exclusive categories.")
14
Entry Criteria for Registry
Positive screen for barriers to compliance Positive CYSHCN screen Physician referral Health plan referral Diagnosis list All should receive compliance barrier screen and should have individual plans of care written and communicated to team. Subdivide by separate disease-specific registries See packets

15
Tracking Registry Once your chronic or complex illness cohort is identified, you must decide on a tracking system. Most EMRS have flag systems, so a flag or icon can be added to these patients Many practices on paper charts use stickers of a specific color on the patient’s chart. There needs to be communication of Registry status to patients and staff
![]()
16
High Risk Registry Tracking Tool
TNAAP High Risk Registry Tracking Tool Patient Name/DOB Emergency Plan Updated Last Plan of Care Last updated: Disease States Follow up Interval Last appointment Last WCC Influenza Immunization Given? (Y/N) Barrier to Compliance Screen Last Given Disease Specific Plan of Care Up-to-Date? (Y/N) Needs: Tools such as these are helpful in tracking compliance with care plans for multiple patients.
![]()
17
MOC QI Aim #3 Measurements
Report baseline registry formation based on objective screening (20 charts, alright if 0). Institute CSHCN screener and/or other Enter children with positive screens into registry. Tag record with identifier positive or negative Monthly, select 10 charts from general population that month to audit for use of CSHCN Screener or other evidence of screening for registry entry.
. Institute CSHCN screener and/or other. Enter children with positive screens into registry. Tag record with identifier positive or negative. Monthly, select 10 charts from general population that month to audit for use of CSHCN Screener or other evidence of screening for registry entry.")
18
Care Coordination Framework
Team-based Communication Disease management Case Management Patient For the purposes of this curriculum: Case Management: screening for and overcoming barriers to compliance Disease management: a team approach to evidence-based care. Where evidence base is lacking, a team approach to supporting a care path based on shared knowledge of a patient and his/her disease process. Communication: focused on timely information exchange with entities to which a provider refers.

19
What is Disease Management?

20
Disease Management “Disease management supports the physician or practitioner/patient relationship and plan of care, emphasizes prevention of exacerbations and complications using evidence –based practice guidelines and patient empowerment strategies, and evaluates clinical, humanistic, and economic outcomes on an ongoing basis with the goal of improving overall health” Disease Management Association of America. DMAA Definition of Disease Management. {Accessed: January 26,2007};available from :

21
What are the characteristics of successful disease management programs?

22
Successful Disease Management Programs
Individualized Case Management In-person contacts Focus on hospital discharges Encourage use of cost effective therapies Simple Patient Centered Large/overarching Identified measurement parameters Incentives Mathmatica: -Disease Management-Does it work? *** Mackenzie article on features of successful DzMgt programs *** How defined success:*** Individualized Case Management: plans of care take the patient into account as an individual. Health literacy, social, emotional, medical, developmental, educational realms are addressed and incorporated as part of the care plan. In-person contacts: relationship, face-to-face contact, and accountability with clearly defined roles are important. Focus on hospital discharges: most acute processes and navigating plan of care for most severe/costly domains of a patient’s illness are important. Encourage patients to use cost effective therapies by reducing cost sharing for these components Simple: for patient and staff Patient Centered Large/overarching: to achieve statistical significance and recruit supportive resources. Identified measurement parameters Incentives We cannot manipulate all these variables, but we can influence some.

23
Context of Studies Adult cohorts Pediatric Cohorts
Large volumes of same diagnosis Good evidence base for therapies Costs/Morbidity center around large volume cohorts Few large volume cohorts Many severe illnesses without standardized evidence base for therapy Cost/Morbidity located in 10% of children, small cohorts Focus on hospitalization: most individuals hospitalized are readmissted in 9 months, acute problems not resolved at time of discharge, patients lack adequate support or self care skills at the time of discharge. Focus on cost savings measures: many incentives are there for meds, because 80% of CYSHCN are supported by Medicaid.

24
Considerations in pediatrics
Disease management strategies in pediatrics must be applicable across a variety of disease states. Disease management in pediatrics requires both population approaches and individual case management approaches Processes in pediatrics must be fluid enough to respond to the situational needs of highly specialized/varied patients. Formalized disease management in primary care Formalized disease management programs are often a foreign concept in the private office setting, so it is important that we spend time undergirding changes in job roles and processes that need to take place. Source: AHRQ technical review. A critical Analysis of care coordination strategies for children with special healthcare needs. Quote: Will never be able to investigate most successful strategies in disease management until disease-specific program are abandoned.

25
Disease Manager Functions
Support evidence based care and individual plans of care Disease-specific knowledge a must Provides education for self-management Compliance tracking and reassessment a large role Works with MD and case manager to optimize access, compliance, and education

26
Disease Management Team Tasks
Patient screening and registry formation Evaluates patient/family comprehension of plan of care Performs disease education as appropriate Refers patient to case manager as risks for noncompliance identified

27
Disease Management Team Tasks
Tracks and monitors patient compliance with care plans by registry Augments communication by keeping team members aware of patient status Assists with transitions to/from hospital/adult care Authority to schedule override

28
Disease Management Workflow
Assess Monitor/Evaluate/Adjust Evidence-based plan Maintain Registry Support self Management Communicate Plan Link Community Resources Execute

29
Keep it Simple Form your registry
Support the evidence base with process Educate and involve the team Use Tools Continually reassess Set regular communication times

30
Assess Record which diseases in your practice are leading to increased service utilization or functional capacity limitation Review the evidence base for these diseases Form your registry (General or disease-specific) No one is going to know your practice population better than you do, so you can take a look at the indices you would like to improve and let that guide your protocol development. Involving payers in consideration of the disease states you want to monitor may be a key to increased reimbursements.
 No one is going to know your practice population better than you do, so you can take a look at the indices you would like to improve and let that guide your protocol development. Involving payers in consideration of the disease states you want to monitor may be a key to increased reimbursements.")
31
Evidence-based plan Support evidence base with process
Identify essential action steps that will support evidence base Form office procedure around information exchange that must take place to support evidence-based intervention Describe the responsibilities in this work-flow by job description Don’t forget case management plan

32
Communicate Plan Physician Disease Management
Case Management/Linkage with Resources Referral coordinator/other staff Patients PHYSICIAN MUST HAVE WRITTEN CARE PLAN FOR PATIENTS Explain division of labor by job type. General diagnosis cohort procedures are important to discuss ahead of time. However, written plan of care for each individual patient is essential to communicating the needs and individual nuances of care to the rest of the team.

33
Execute Processes for a diagnosis cohort or individual patient executed Patient expectations communicated to patients Team aware of plan and monitoring compliance

34
Link Community Resources
Screen for barriers to compliance Create care plan for overcoming barriers Monitor patient compliance with this plan Follow-up and reassess Disease manager/nurse screen. Case Management Job role to conduct interview, create care coordination care plan, and follow-up.

35
Support Self Management
Written plan of care to patients Assessment of health literacy for self management Disease or patient-specific patient education for self management Referral to case management as needed. Disease Manager job role

36
Monitor/Evaluate/Adjust
Follow-up interval specified in patient plan of care or part of evidence-based care path Track no shows and compliance with referrals Maintain patient contact/Assure follow-up occurs Reassess response to interventions Adjust plan accordingly Continually reassess for barriers to care Physician establishes follow-up interval/plan Disease manager tracks compliance with medical care plan. Case Manager follows up on compliance with care coordination plan. All reassess.

37
A written plan of care is essential to communicating patient specific expectations to all team members. Your practice must decide what constitutes a finished plan of care. Some examples follow.

38
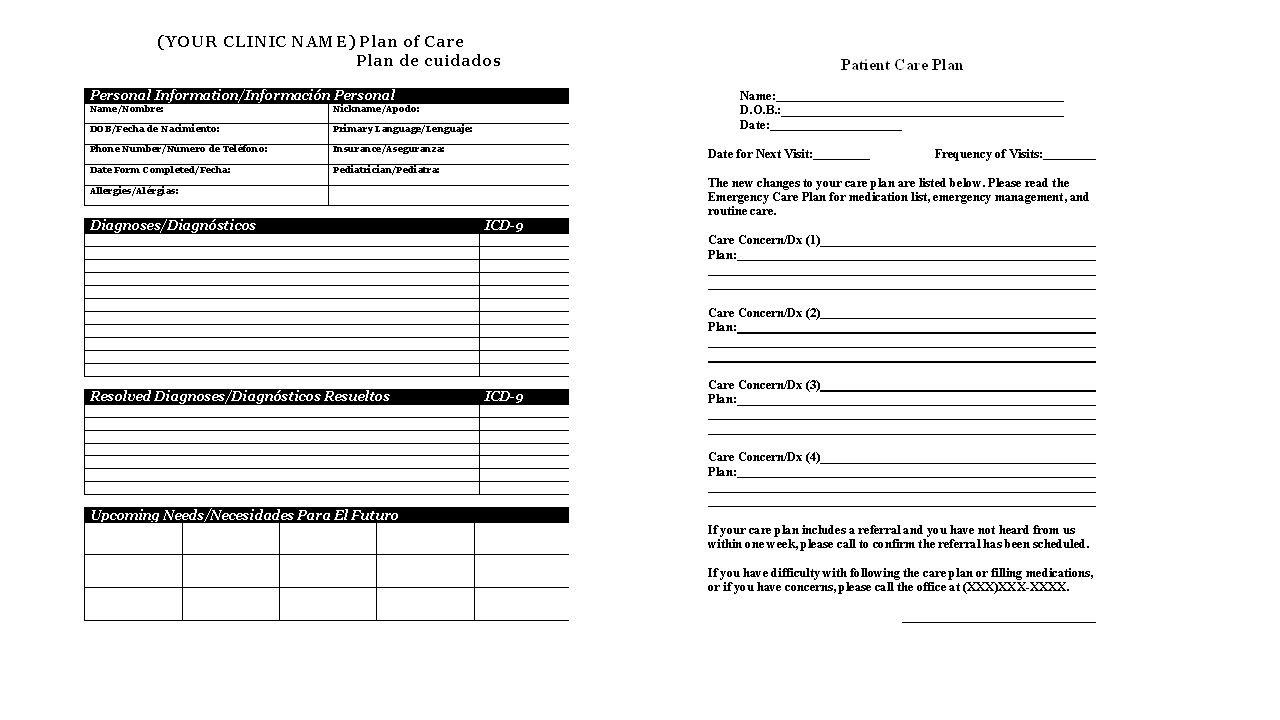
Three types of plans for CYSHCN
Patient Summary: Problem list, PMH, Meds, Allergies, Specialists, Therapies, Typical Laboratory Values and Exam, Cultural and Social Considerations, Legal Action Plan: today’s additions, changes Emergency Plan

39
MOC QI Aim #4 ---------------------------------- Written plans of care for team
To be able to institute evidence-based protocols and management of high risk patients, you must have a system of identification of them.

40
MOC QI Aim #4 Measurements
Report baseline proportion of chronic disease registry patients with written plans of care on chart (20 patients from baseline chronic illness registry, alright if 0) Institute team management strategies Monthly, select 10 charts from patients seen in the chronic/complex disease registry to audit for presence of written plan of care Wanted to keep open, so practices could address different disease states at their discretion. May general care plan for all in the chronic/complex disease registry, or specify per disease.
 Institute team management strategies. Monthly, select 10 charts from patients seen in the chronic/complex disease registry to audit for presence of written plan of care. Wanted to keep open, so practices could address different disease states at their discretion. May general care plan for all in the chronic/complex disease registry, or specify per disease.")
41
Example Forms You and your team must decide what constitutes a completed plan of care. At the very least, it should include the diagnosis, medications, therapies, referrals, and/or instructions for follow-up. Many practices will conduct a more extensive baseline emergency plan that is updated periodically and supplemented with visit-specific plans of care.

43
Baseline Measurements, 20 charts
Evidence of screening for barriers to compliance Evidence of linking patients with barriers to compliance to community resources Evidence of screening for CSHCN registry Evidence of written care path in the record for those in CSHCN registry

44
Monthly Measurements 10 charts general population:
Were they screened for barriers to compliance? Were they screened for CSHCN registry 10 charts with positive barrier to compliance screen: Is there documentation of linking patient with a resource to overcome barrier to compliance? 10 charts CSHCN Registry: Is there evidence of the written care plan you have agreed to use?

45
Overall AIM Statement Involved practices will improve chronic disease registry formation by 50% by the end of data collection. 25% of registry patients of involved practices will have a care plan with therapeutic recommendations and/or goal by the end of data collection. Involved practices will improve screening for risk factors for noncompliance by 50% by the end of data collection. 25% of patients with a risk factor for non-compliance will be linked with community resources needed to promote compliance by the end of data collection.

46
Requirements for MOC participation
Summit Participation Baseline/follow-up NCQA PCMH Medical Home Survey Baseline/monthly (4 month) data entry/analysis for QIDA parameters Participation in 2 of 4 technical assistance webinars/conference calls Participation in final QI Program Synopsis call/meeting PCMH survey intended to be a GAP analysis. Can be used for NCQA certification in future.
 data entry/analysis for QIDA parameters. Participation in 2 of 4 technical assistance webinars/conference calls. Participation in final QI Program Synopsis call/meeting. PCMH survey intended to be a GAP analysis. Can be used for NCQA certification in future.")
Similar presentations















 Assuring No Child Enters Kindergarten With an Undetected Developmental.>")



