Download presentation
Presentation is loading. Please wait.

1
1 Decision-support for Mechanical Ventilation Alan H. Morris, M.D. European Society for Computing and Technology in Anesthesia and Intensive Care, Amsterdam, 8 October 2010 No Conflict of Interest No Commercial Association

2
2 1.Need for decision-support (clinician uncertainty, human performance) 2.Science and reproducibility 3.Decision-support (influence clinician behavior)
 2.Science and reproducibility 3.Decision-support (influence clinician behavior)")
3
PCIRV… LFPPV-ECCO 2 R Mechanical Ventilation ARDS Randomize Extubation Death Extubation Death NIH N01-HL 46062 Alan H. Morris, M.D. Computerized Protocols Developed 1985-87 1987-91

4
4 Clinical Uncertainty- Complexity: >236 Variable Categories

5
5 1.Need for decision-support (clinician uncertainty) 2.Science and reproducibility 3.Decision-support (influence clinician behavior)
 2.Science and reproducibility 3.Decision-support (influence clinician behavior)")
6
Douglas C. Giancoli. Physics. prentice Hall, Englewood Cliffs, NJ 1995:3 Science: testing..experiments..distinguish science from other creative fields (key is the belief that true results can be reproduced by others. Reproducibility requires a detailed and explicit method)
.")
7
7 High-quality clinical trials require consistent compliance with evidence-based guidelines. High compliance makes the clinical trial more reproducible – a requirement of good science. Differences in clinician compliance with guidelines/study protocol could influence the results of clinical trials

8
8 Requirement of good science: Reproducibility is what confirms the proper description of nature’s behavior. If one scientist has properly described nature's behavior, another scientist using the same method should obtain the same result.

9
Requirement of good science: Replication of experimental results is a primary requirement before new scientific information is embraced by the standard works of the domain (e.g., textbooks). Replication of results depends on reproducible methods.

10
10 The hospital, the operating room, and the wards should be laboratories, laboratories of the highest order. William S. Halsted, M.D.

11
11 Experimental Human Clinical Outcomes Research Laboratory: 1.Good Clinical Care 2.Ethical Care 3.Reliable Data Capture 4.Standardized Clinician Response (Reproducible Method)
")
12
12 1.Need for decision-support (clinician uncertainty) 2.Science and reproducibility 3.Decision-support (influence clinician behavior) – adaptive expert system
 2.Science and reproducibility 3.Decision-support (influence clinician behavior) – adaptive expert system")
13
Medical subject headings - Ovid®: Guideline: “A systematic statement of policy rules or principles”-where to go but not how to get there Protocol: “Precise and detailed plans for the study of a medical or biomedical problem and/or for a regimen of therapy.”- how to get there (Adequately explicit protocol: enough detail to lead different clinicians to the same patient-specific decision - reproducible clinical decision method) 13
 13")
14
14 王皓在比赛中 马琳在比赛中

15
15 Guideline “Win the point” Inadequately explicit protocol “Hit the left corner” Adequately explicit protocol “Wait for a high return and hit the ball hard with a left spin, curving to the opponent’s left, to land within 1 inch of the left corner of the table.”

16
Meehl P. Clinical versus statistical prediction - a theoretical analysis and a review of the evidence. Minneapolis: University of Minnesota Press 1954. McDonald C, Overhage J. JAMA 1994;271(11):872-873. Tierney WM et al. J Am Med Informatics Assn 1995;2(5):316-22. Zielstorff R. J Am Med Informatics Assn 1998;5(3):227-236. Inadequately explicit Try to return to F I O 2 =0.4 and PEEP=5 as soon as possible.
: Tierney WM et al. J Am Med Informatics Assn 1995;2(5): Zielstorff R. J Am Med Informatics Assn 1998;5(3): Inadequately explicit Try to return to F I O 2 =0.4 and PEEP=5 as soon as possible..")
17
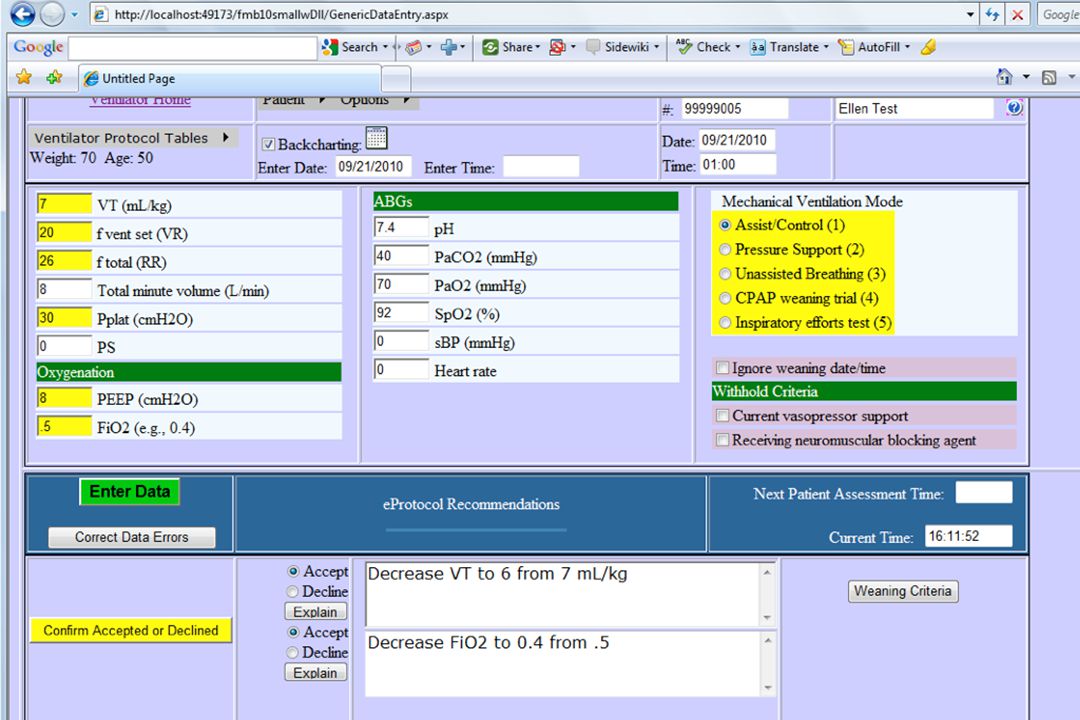
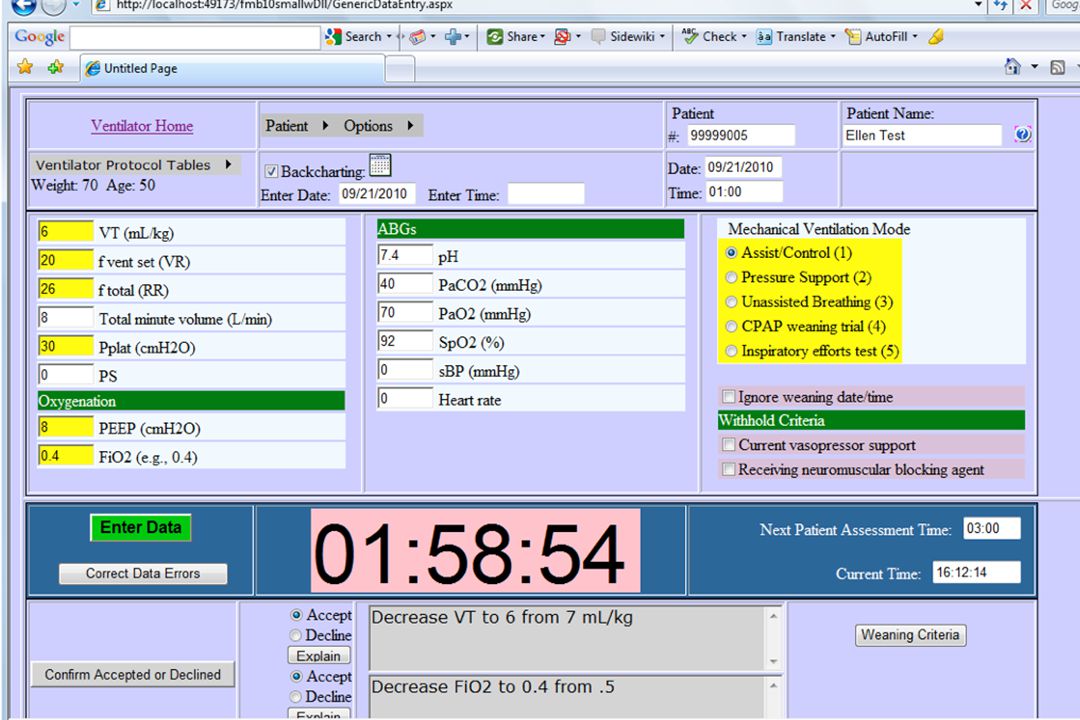
17 Decline 5% of recommendations Accept 95% of recommendations Patient data: SpO2, PaO2, pH Respiratory Care Patient-specific instructions: Mode, Tidal Volume, Rate, FIO2, Ppeak, PEEP Capture reason for declining Clinician Accepts or Declines Patient Computer Protocol Continual Operation (Mechanical Ventilation Protocol Example)
")
18
eProtocol- Mechanical- Ventilation vs. Controls (usual care) Unpublished data from an RCT Box = interquartile range (IQR) and median Bars = IQR limits ± ~1.5 IQR
 Unpublished data from an RCT Box = interquartile range (IQR) and median Bars = IQR limits ± ~1.5 IQR.")
19
97 Patients FIO2 ≤0.6 Pplateau ≤35 cm H 2 O Target V T =7 ml/kg PBW 103 Patients Goals

20
20 Pplateau >35 cm H 2 O x Days Inspired %O 2 >60 x Days AHCPR #HS06954 (T East, PhD, PI)
")
21
Patient is ready for a 5 min test for inspiratory effort. Reduce Ventilator Set Rate to 10. Enter Total Ventilatory Rate when it exceeds 10 or at the end of 5 min. 21

22
22

23
Complexity is transparent (hidden) 23
 23")
24
24

25
C. Fluid Bolus (Non-shock, except cell #19): 1. Administer 15 ml/kg PBW normal saline, Plasmalyte, or Ringer’s lactate (rounded to the nearest 250 ml) or 1 unit RBCs or 25 grams albumin (choice at discretion of physician) over <= 1 hour then reassess patient. For cells 5, 6, 9, 10, reassess within one hour. Administer up to 3 boluses over 24 hours if indicated by protocol. This 24 hour period begins with the first protocol- mandated non-shock bolus OR the first protocol- mandated bolus following shock reversal. 2. Additional fluid boluses are allowed at the discretion of the physician. 25
 or 1 unit RBCs or 25 grams albumin (choice at discretion of physician) over <= 1 hour then reassess patient. For cells 5, 6, 9, 10, reassess within one hour. Administer up to 3 boluses over 24 hours if indicated by protocol. This 24 hour period begins with the first protocol- mandated non-shock bolus OR the first protocol- mandated bolus following shock reversal. 2. Additional fluid boluses are allowed at the discretion of the physician. 25.")
26
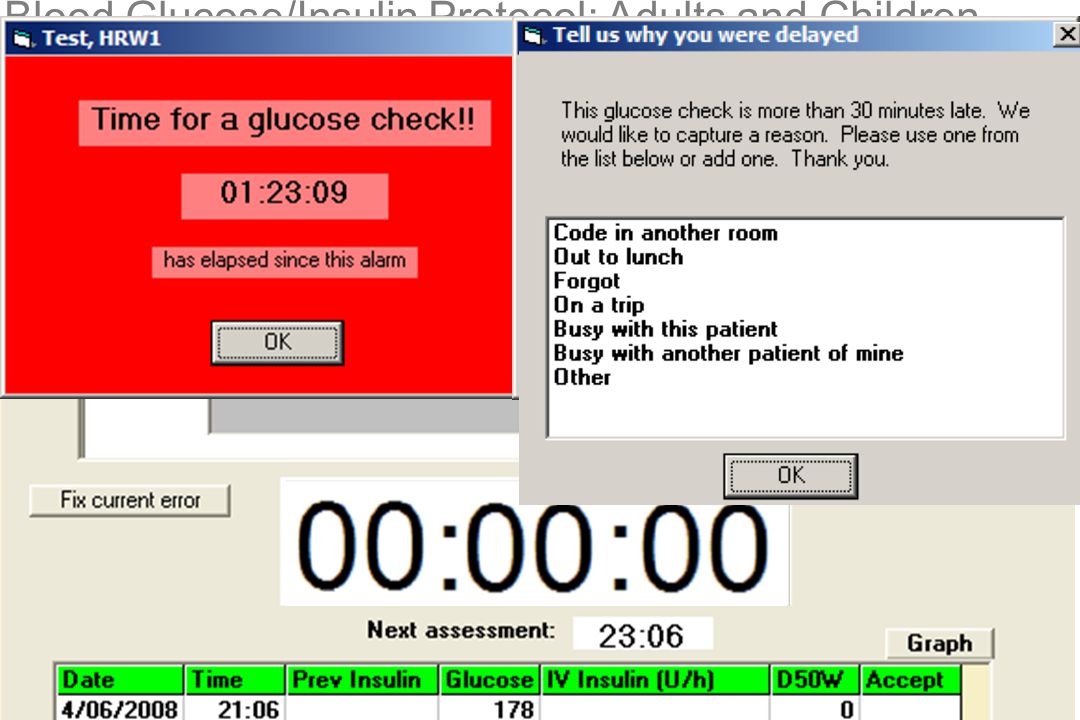
Blood Glucose/Insulin Protocol: Adults and Children

28
% Measurements Blood Glucose (mg/dl) 8642086420 04080120160200240280320 Bedside Computer Protocol Bedside Paper Protocol Simple Guideline P<0.0001 786 Patients 44,979 Measurements → Target Range
 Bedside Computer Protocol Bedside Paper Protocol Simple Guideline P< Patients 44,979 Measurements → Target Range")
29
% Measurements Blood Glucose (mg/dl) 8642086420 04080120160200240280320 Western USA Southeast USA Northeast USA Singapore P=0.18 753 Patients 36,302 Measurements → Target Range Blood Glucose Computer Protocol
 Western USA Southeast USA Northeast USA Singapore P= Patients 36,302 Measurements → Target Range Blood Glucose Computer Protocol")
30
1Mar07 Thompson, BT et al. J Diabetes Sci Technol 2008;2(3):357-68 99 Adults - 6 ICUs 48 Children - 5 ICUs % Blood Glucose Measurements 98765432109876543210 04080120160200240280320 Blood Glucose (mg/dl by 5 mg/dl groups) Δ Adult Pediatric
: Adults - 6 ICUs 48 Children - 5 ICUs % Blood Glucose Measurements Blood Glucose (mg/dl by 5 mg/dl groups) Δ Adult Pediatric.")
31
Translation: Research Practice 13 Adult ICUs: Intermountain Healthcare Intensive Medicine Clinical Program in 7 hospitals ranging from a: 72 bed primary care hospital to a 480 bed tertiary care hospital

32
% Measurements Blood Glucose (mg/dl) 8642086420 04080120160200240280320 ICU Type Pa- tients Measure- ments Research49321,321 Clinical Care 2,296109,458 → Target Range Blood Glucose Computer Protocol
 ICU Type Pa- tients Measure- ments Research49321,321 Clinical Care 2,296109,458 → Target Range Blood Glucose Computer Protocol")
33
eProtocols: reproducible method Adult and pediatric ICUs (bridge different disciplines) In usual clinical care (translate research to practice)
 In usual clinical care (translate research to practice)")
34
34 1.Need for decision-support (clinician uncertainty, human performance) 2.Science and reproducibility 3.Decision-support (influence clinician behavior)
 2.Science and reproducibility 3.Decision-support (influence clinician behavior)")
35
35

36
36

37
37 NIH Roadmap contract # HHSN268200425210C: 1Mar07

38
38 NIH Roadmap contract # HHSN268200425210C: 1Mar07 0.5% stop - a priori

39
CPAP weaning trial successful. Click red CONFIRM button and switch ventilator to Pressure Support mode with PS=20 cm H2O, PEEP=5 and FIO2=0.5 if you want to proceed. Then wait and enter total ventilatory rate, SpO2 and evaluate for respiratory distress within 5 min. 39

40
40

41
41 Crit Care Med ‘08;361787–95)
")
42
% Measurements Blood Glucose (mg/dl) Bedside Computer Protocol ∆ Bedside Paper Protocol + Simple Guideline P<0.0001 → Target Range 8642086420 04080120160200240280320
 Bedside Computer Protocol ∆ Bedside Paper Protocol + Simple Guideline P< → Target Range")
48
Local research group Multiple IH sites Multiple sites- geographically dispersed Increasing levels of clinician trust - must abandon personal style Clinician leader

49
49 Unnecessary variation, and error, exist in medical care. Computer protocols help clinicians deliver consistent, evidence-based, care with a reproducible method.

50
50 1.Need for decision-support (clinician uncertainty, human performance) 2.Science and reproducibility 3.Decision-support (influence clinician behavior)
 2.Science and reproducibility 3.Decision-support (influence clinician behavior)")
51
% of 15,381 Heart Failure Outpatients Receiving Appropriate Guideline- Based Treatment In 165 clinics Maximum 90% of clinics Median 10% of clinics Minimum Legend: Range of results by study clinic %

52
52 0 1 2 3 4 Survival Months Following Discharge Re: (Kfoury, French – Intermountain Nov 2008) Adherence to Heart Failure Core Measures
 Adherence to Heart Failure Core Measures")
53
53 % 0 20 40 60 80 100 Audit 4 Interview 92 1816141210876543210 40 30 20 10 0 N V T (ml/kg PBW) Evidence Adhere to “Best Practice?“ Brunkhorst F, Engel C, Ragaller M, Welte T, Rossaint R, Gerlach H, et al. Practice and perception—A nationwide survey of therapy habits in sepsis. Crit Care Med. 2008;36(10):1-6
:1-6.")
54
54 Miller, GA. Psychological Review 1956;63(2):81-97 East, TD et al. Chest 1992; 101:697-710 (PCIRV) Cowan N. Behav Brain Sci 2001;24:87 # Conceptual Objects Humans Can Accommodate (“Chunks” in Short Term Memory) Before Decisions are Degraded ~ 7 ~ 4
 Cowan N. Behav Brain Sci 2001;24:87 # Conceptual Objects Humans Can Accommodate ( Chunks in Short Term Memory) Before Decisions are Degraded ~ 7 ~ 4.")
55
Proteomics Functional Genetics Structural Genetics Clinical Phenotype Facts / Decision 55 The Roundtable on Evidence-Based Medicine: Learning Healthcare System Concepts v. 2008. Annual Report, IOM, Nat Acad Sci. P9, IOM Meeting, 8 October 2007. Growth in facts affecting provider decisions versus human cognitive capacity. This limit makes protocol rule generation easier, and manageable. 1000 100 10 Human Cognitive 5 Capacity William Stead, MD – Challenges to Providers

56
Decision-support (patient- clinician encounter scale) Involve end-users Quick testing of an idea Trust
 Involve end-users Quick testing of an idea Trust")
57
R Clemente H Aaron L Gehrig “Strike him out” 57 W Mays B Ruth

58
58 Guideline “Strike him out” Inadequately explicit protocol “Curve ball low and inside” Adequately explicit protocol “Throw a 67 mile per hour curve ball low and inside within 1 inch of the back corner of the plate and 2 inches above the left knee, after a 45 second pause”

Similar presentations