Download presentation
Presentation is loading. Please wait.

1
Membrane potentials 膜电位
Xia Qiang, MD & PhD Department of Physiology Room C518, Block C, Research Building, ZJU School of Medicine Tel:

2
Electrocardiogram ECG(心电图)
")
3
Electroencephalogram
EEG(脑电图)
")
4
Electromyogram EMG(肌电图)
")
5
Extracellular Recording(细胞外记录)
")
6
Intracellular Recording(细胞内记录)
")
7
Recording of membrane potentials

8
Extracellular and Intracellular Recording
Video Extracellular and Intracellular Recording Extracellular recording in earthworm giant axons Intracellular recording in crayfish muscle cells

9
Opposite charges attract each other and
will move toward each other if not separated by some barrier.

10
Only a very thin shell of charge difference
is needed to establish a membrane potential.

12
Resting membrane potential(静息电位)
A potential difference across the membranes of inactive cells, with the inside of the cell negative relative to the outside of the cell Ranging from –10 to –100 mV

13
(超射) (复极化) (极化) (超极化) (去极化) Overshoot refers to the development of
a charge reversal. (超射) A cell is “polarized” because its interior is more negative than its exterior. Repolarization is movement back toward the resting potential. (复极化) (极化) Depolarization occurs when ion movement reduces the charge imbalance. Hyperpolarization is the development of even more negative charge inside the cell. (超极化) (去极化)
 A cell is. polarized because. its interior. is more. negative. than its. exterior. Repolarization is. movement back. toward the. resting potential. (复极化) (极化) Depolarization. occurs. when ion. movement. reduces the. charge. imbalance. Hyperpolarization is. the development of. even more negative. charge inside the cell. (超极化) (去极化)")
14
electrochemical balance
chemical driving force electrochemical balance electrical driving force

15
K+ equilibrium potential (EK) (37oC)
The Nernst Equation: K+ equilibrium potential (EK) (37oC) German physical chemist and physicist R=Gas constant T=Temperature Z=Valence F=Faraday’s constant (钾离子平衡电位)
 (37oC) German physical chemist and physicist. R=Gas constant. T=Temperature. Z=Valence. F=Faraday’s constant. (钾离子平衡电位)")
16
Begin: K+ in Compartment 2, Na+ in Compartment 1; BUT only K+ can move. Ion movement: K+ crosses into Compartment 1; Na+ stays in Compartment 1. buildup of positive charge in Compartment 1 produces an electrical potential that exactly offsets the K+ chemical concentration gradient. At the potassium equilibrium potential:

17
Begin: K+ in Compartment 2, Na+ in Compartment 1; BUT only Na+ can move. Ion movement: Na+ crosses into Compartment 2; but K+ stays in Compartment 2. buildup of positive charge in Compartment 2 produces an electrical potential that exactly offsets the Na+ chemical concentration gradient. At the sodium equilibrium potential:

18
Difference between EK and directly measured resting potential
Ek Observed RP Mammalian skeletal muscle cell mV -90 mV Frog skeletal muscle cell mV -90 mV Squid giant axon mV -70 mV

19
Goldman-Hodgkin-Katz equation
The systemic inflammatory response syndrome (SIRS) is a clinical response arising from a nonspecific insult manifested by two or more of the following: Fever or hypothermia Tachycardia Tachypnea Leukocytosis, leukopenia, or a left-shift (increase in immature neutrophilic leukocytes in the blood) Recent evidence indicates that hemostatic changes play a significant role in many SIRS-linked disorders. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Opal SM, Thijs L, Cavaillon JM, et al. Relationships between coagulation and inflammatory processes. Crit Care Med. 2000; 28:S81-2. Goldman-Hodgkin-Katz equation
 is a clinical response arising from a nonspecific insult manifested by two or more of the following: Fever or hypothermia. Tachycardia. Tachypnea. Leukocytosis, leukopenia, or a left-shift (increase in immature neutrophilic leukocytes in the blood) Recent evidence indicates that hemostatic changes play a significant role in many SIRS-linked disorders. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Opal SM, Thijs L, Cavaillon JM, et al. Relationships between coagulation and inflammatory processes. Crit Care Med. 2000; 28:S81-2. Goldman-Hodgkin-Katz equation.")
20
Role of Na+-K+ pump: Electrogenic Hyperpolarizing
Establishment of resting membrane potential: Na+/K+ pump establishes concentration gradient generating a small negative potential; pump uses up to 40% of the ATP produced by that cell! The systemic inflammatory response syndrome (SIRS) is a clinical response arising from a nonspecific insult manifested by two or more of the following: Fever or hypothermia Tachycardia Tachypnea Leukocytosis, leukopenia, or a left-shift (increase in immature neutrophilic leukocytes in the blood) Recent evidence indicates that hemostatic changes play a significant role in many SIRS-linked disorders. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Opal SM, Thijs L, Cavaillon JM, et al. Relationships between coagulation and inflammatory processes. Crit Care Med. 2000; 28:S81-2.
 is a clinical response arising from a nonspecific insult manifested by two or more of the following: Fever or hypothermia. Tachycardia. Tachypnea. Leukocytosis, leukopenia, or a left-shift (increase in immature neutrophilic leukocytes in the blood) Recent evidence indicates that hemostatic changes play a significant role in many SIRS-linked disorders. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Opal SM, Thijs L, Cavaillon JM, et al. Relationships between coagulation and inflammatory processes. Crit Care Med. 2000; 28:S81-2.")
21
Sodium-potassium Pump
Click here to play the Sodium-potassium Pump Flash Animation

22
Origin of the normal resting membrane potential
K+ diffusion potential Na+ diffusion Na+-K+ pump

24
Action potential(动作电位)
Some of the cells (excitable cells) are capable to rapidly reverse their resting membrane potential from negative resting values to slightly positive values. This transient and rapid change in membrane potential is called an action potential
 are capable to rapidly reverse their resting membrane potential from negative resting values to slightly positive values. This transient and rapid change in membrane potential is called an action potential.")
25
Negative after-potential
A typical neuron action potential Positive after-potential Negative after-potential Spike potential After-potential

26
Electrotonic Potential(电紧张电位)
")
27
The size of a graded potential (here, graded depolarizations) is proportionate to the intensity of the stimulus.

28
Graded potentials can be:. EXCITATORY. or. INHIBITORY
Graded potentials can be: EXCITATORY or INHIBITORY (action potential (action potential is more likely) is less likely) The size of a graded potential is proportional to the size of the stimulus. Graded potentials decay as they move over distance.
 is less likely) The size of a graded potential is proportional to the size of the stimulus. Graded potentials decay as they move over distance.")
29
Graded potentials decay as they move over distance.

30
Local response(局部反应) Not “all-or-none” (全或无)
Electrotonic propagation: spreading with decrement(电紧张性扩布) Summation: spatial & temporal(时间与空间总和)
 Summation: spatial & temporal(时间与空间总和)")
31
Threshold Potential(阈电位): level of depolarization needed to trigger an action potential (most neurons have a threshold at -50 mV)
: level of depolarization needed to trigger an action potential (most neurons have a threshold at -50 mV)")
32
Ionic basis of action potential

33
(1) Depolarization(去极化):
Activation of Na+ channel Blocker: Tetrodotoxin (TTX) (河豚毒素)
 (河豚毒素)")
34
(2) Repolarization(复极化): Inactivation of Na+ channel
Activation of K+ channel Blocker: Tetraethylammonium (TEA)(四乙胺)
(四乙胺)")
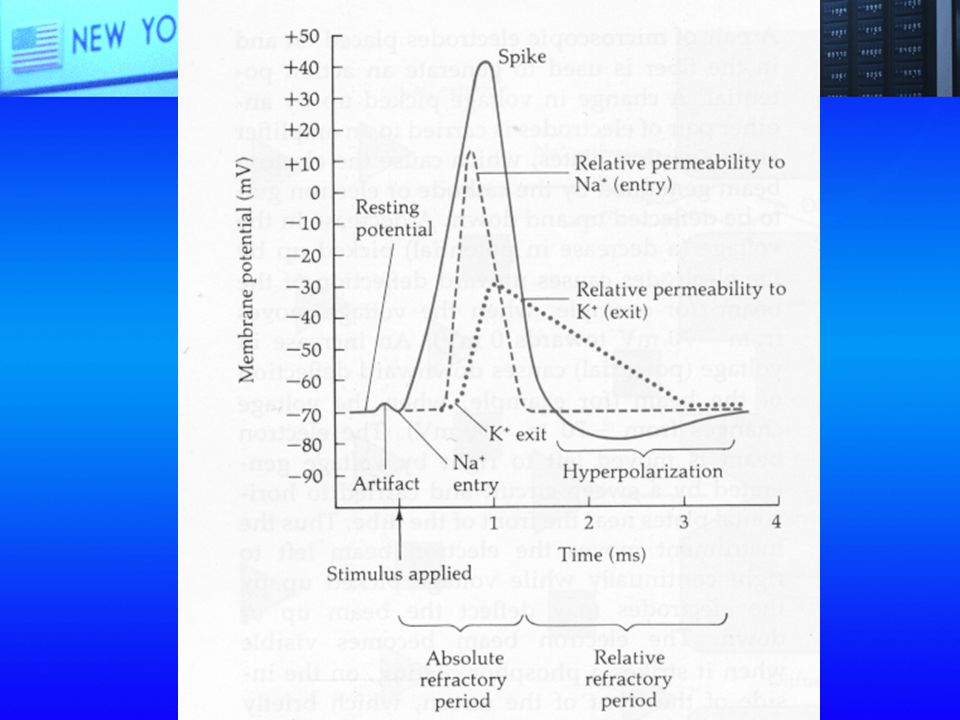
36
The rapid opening of voltage-gated Na+ channels
explains the rapid-depolarization phase at the beginning of the action potential. The slower opening of voltage-gated K+ channels explains the repolarization and after hyperpolarization phases that complete the action potential.

39
voltage-gated Na+ channels allows rapid entry of Na+,
An action potential is an “all-or-none” sequence of changes in membrane potential. The rapid opening of voltage-gated Na+ channels allows rapid entry of Na+, moving membrane potential closer to the sodium equilibrium potential (+60 mv) Action potentials result from an all-or-none sequence of changes in ion permeability due to the operation of voltage-gated Na+ and K + channels. The slower opening of voltage-gated K+ channels allows K+ exit, moving membrane potential closer to the potassium equilibrium potential (-90 mv)
 Action potentials result. from an all-or-none. sequence of changes. in ion permeability. due to the operation. of voltage-gated. Na+ and K + channels. The slower opening of. voltage-gated K+ channels. allows K+ exit, moving membrane potential. closer to the potassium. equilibrium potential (-90 mv)")
40
Voltage Gated Channels
Click here to play the Voltage Gated Channels and Action Potential Flash Animation

41
Mechanism of the initiation and termination of AP

42
Re-establishing Na+ and K+ gradients after AP
Na+-K+ pump “Recharging” process

43
Properties of action potential (AP)
Depolarization must exceed threshold value to trigger AP AP is all-or-none AP propagates without decrement

46
Nobel Prize in Physiology or Medicine 1963
How to study ? Nobel Prize in Physiology or Medicine 1963 "for their discoveries concerning the ionic mechanisms involved in excitation and inhibition in the peripheral and central portions of the nerve cell membrane" Eccles Hodgkin Huxley Voltage Clamp

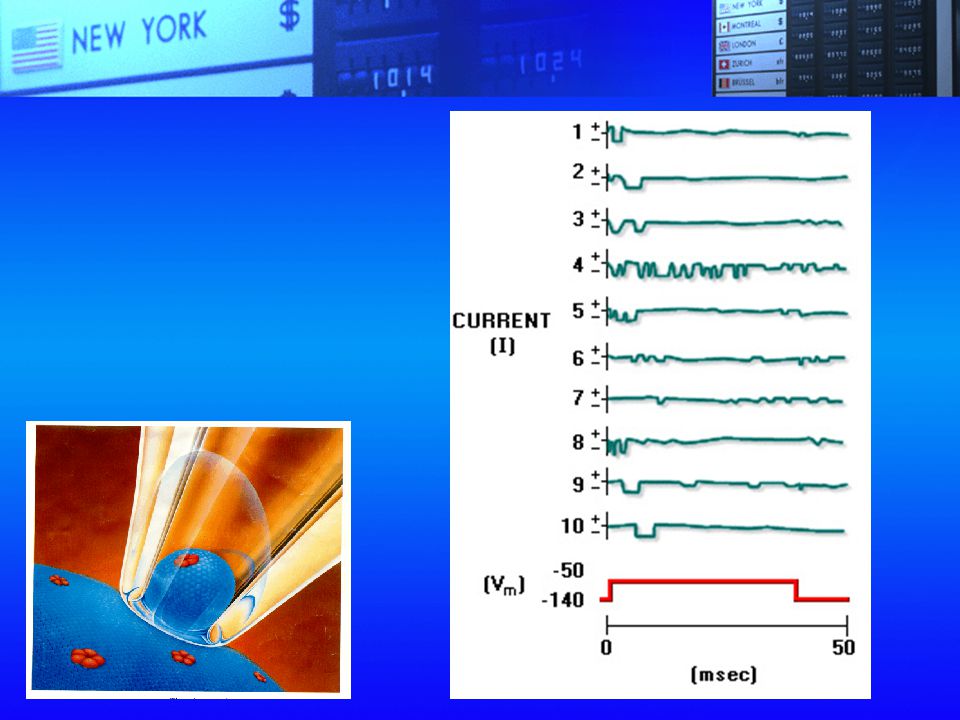
47
Currents recorded under voltage clamp condition

48
Nobel Prize in Physiology or Medicine 1991
Patch Clamp Nobel Prize in Physiology or Medicine 1991 "for their discoveries concerning the function of single ion channels in cells" Erwin Neher Bert Sakmann

50
The Squid and its Giant Nerve Fiber
Video The Squid and its Giant Nerve Fiber "The Squid and its Giant Nerve Fiber" was filmed in the 1970s at Plymouth Marine Laboratory in England. This is the laboratory where Hodgkin and Huxley conducted experiments on the squid giant axon in the 1940s. Their experiments unraveled the mechanism of the action potential, and led to a Nobel Prize. Long out of print, the film is an historically important record of the voltage-clamp technique as developed by Hodgkin and Huxley, as well as an interesting glimpse at how the experiments were done.

51
Video Patch Clamp

52
Conduction of action potential(动作电位的传导)
Continuous propagation in the unmyelinated axon

53
Action Potential Propagation in an Unmyelinated Neuron Flash Animation
Click here to play the Action Potential Propagation in an Unmyelinated Neuron Flash Animation

54
Saltatory propagation in the myelinated axon

55
Saltatorial Conduction: Action potentials jump from one node to the
next as they propagate along a myelinated axon. (跳跃性传导)
")
56
Action Potential Propagation
Click here to play the Action Potential Propagation in Myelinated Neurons Flash Animation

57
Excitation and Excitability (兴奋与兴奋性)
To initiate excitation (AP) Excitable cells Stimulation Intensity Duration dV/dt
 Excitable cells. Stimulation. Intensity. Duration. dV/dt.")
58
Strength-duration Curve(强度-时间曲线)
")
59
Threshold intensity(阈强度) & Threshold stimulus(阈刺激)
Four action potentials, each the result of a stimulus strong enough to cause depolarization, are shown in the right half of the figure.

60
Refractory period following an AP:
1. Absolute Refractory Period: inactivation of Na+ channel(绝对不应期) 2. Relative Refractory Period: some Na+ channels open(相对不应期)
 2. Relative Refractory Period: some Na+ channels open(相对不应期)")
62
Factors affecting excitability
Resting potential Threshold Channel state

63
The propagation of the action potential from the dendritic
to the axon-terminal end is typically one-way because the absolute refractory period follows along in the “wake” of the moving action potential.

64
SUMMARY Resting potential: Graded potential K+ diffusion potential
Na+ diffusion Na+ -K+ pump Graded potential Not “all-or-none” Electrotonic propagation Spatial and temporal summation

65
Action potential Refractory period
Depolarization: Activation of voltage-gated Na+ channel Repolarization: Inactivation of Na+ channel, and activation of K+ channel Refractory period Absolute refractory period Relative refractory period

66
Case Primary Hyperkalemic Periodic Paralysis (原发性高血钾性周期性麻痹) A l0-year-old boy has sporadic attacks of muscle paralysis. The patient has four brothers, all of whom have suffered similar symptoms. The onset of these attacks is characterized by pain associated with contractures of the affected muscles. Later in the attack those muscles may become paralyzed and more flaccid. Episodes of pain and contracture frequently occur without subsequent paralysis. Analysis of blood samples taken during an attack indicates that the patient is hyperkalemic. Plasma K+ levels are normal when the patient is not having an attack. Biopsies of the patient's muscle show a significantly diminished level of intracellular K+ (83 mmol/kg wet tissue) compared with control muscle (95 mmol/kg wet tissue). Basal tissue activity of Na+, K+-ATPase is normal. Paralytic attacks are accompanied by diuresis with increased K+ excretion. Electrophysiologic studies of the patient show that during an attack the excitability and conduction times of motor neurons are normal, as is the function of the neuromuscular junction. Microelectrode studies show that during an attack the magnitude of the resting membrane potential of skeletal muscle cells is diminished compared with control muscle fibers. Electromyography shows that early pared with control muscle fibers. Electromyography shows that early in an attack the muscle contractures are associated with spontaneous action potentials in the affected muscle fibers. Later, during the paralytic phase of an attack, muscle cells become electrically inexcitable - the muscle cells do not respond electrically to stimulation of the motor axons that innervate them. A paralytic attack can be relieved by treating the patient with an insulin injection. Long-term administration of the 2-agonist salbutamol dramatically diminishes the occurrence of episodes of both contractures and subsequent paralytic attacks.
 A l0-year-old boy has sporadic attacks of muscle paralysis. The patient has four brothers, all of whom have suffered similar symptoms. The onset of these attacks is characterized by pain associated with contractures of the affected muscles. Later in the attack those muscles may become paralyzed and more flaccid. Episodes of pain and contracture frequently occur without subsequent paralysis. Analysis of blood samples taken during an attack indicates that the patient is hyperkalemic. Plasma K+ levels are normal when the patient is not having an attack. Biopsies of the patient s muscle show a significantly diminished level of intracellular K+ (83 mmol/kg wet tissue) compared with control muscle (95 mmol/kg wet tissue). Basal tissue activity of Na+, K+-ATPase is normal. Paralytic attacks are accompanied by diuresis with increased K+ excretion. Electrophysiologic studies of the patient show that during an attack the excitability and conduction times of motor neurons are normal, as is the function of the neuromuscular junction. Microelectrode studies show that during an attack the magnitude of the resting membrane potential of skeletal muscle cells is diminished compared with control muscle fibers. Electromyography shows that early pared with control muscle fibers. Electromyography shows that early in an attack the muscle contractures are associated with spontaneous action potentials in the affected muscle fibers. Later, during the paralytic phase of an attack, muscle cells become electrically inexcitable - the muscle cells do not respond electrically to stimulation of the motor axons that innervate them. A paralytic attack can be relieved by treating the patient with an insulin injection. Long-term administration of the 2-agonist salbutamol dramatically diminishes the occurrence of episodes of both contractures and subsequent paralytic attacks.")
67
Questions l. What might account for the patient being hyperkalemic during an attack, while the potassium concentration in his skeletal muscle cells is diminished? What types of alterations of basic cellular processes might underlie this situation? 2. What explains the observation that the magnitude of the resting membrane potentials of the patient's skeletal muscle fibers is diminished during an attack? 3. Does the diminished resting membrane potential have anything to do with the spontaneous action potentials and contractures that occur early in an attack, before paralysis sets in? 4. How might the diminished resting membrane potential contribute to the paralytic phase of an attack, in which muscle cells are electrically inexcitable? 5. How might insulin terminate a paralytic attack? 6. How might long-term administration of salbotamol diminish the occurrence of attacks of contractures and paralysis?

68
Answers l. The hyperkalemia with a concomitant decrease in the amount of K+ in muscle cells suggests that the hrperkalemia is caused bf K+ efflux from the cells, but the cause of K+ efflux is not known. Net K+ efflux from muscle cells might occur because of diminished fate of K+ accumulation by the Na+, K+-ATPase, or an increased rate of K+ efflux from the cell, or a combination of both factors. The observation that Na+, K+-ATPase is normal does not completely rule out a malfunction of this protein during an attack. 2. Elevating extracellular K+ and decreasing the intracellular level of K+ would decrease the potassium equilibrium potential and thus decrease the magnitude of the resting membrane potential. 3. The decreased magnitude of the resting membrane potential initially brings the muscle cells closer to threshold for firing an action potential. For this reason, spontaneous, small fluctuations in the resting membrane potential may reach threshold. This results in spontaneous action potentials and contractions of skeletal muscle cells and leads to the contractures experienced by the patient early in an attack. 4. Prolonged depolarization of the muscle cell plasma membrane will lead to voltage inactivation of Na+ channels in the membrane, which will result in the muscle cell's being unable to fire an action potential. This is believed to be the cause of the paralytic phase of an attack and is supported by the observation that during the paralytic phase, the patient's skeletal muscle cells may be electrically inexcitable. 5. Insulin immediately and powerfully promotes the uptake of K+ by cells and the extrusion of Na+ from cells. Administration of insulin thus corrects the hyperkalemia restores cellular K+ levels toward normal, and causes the resting membrane potential for the affected skeletal muscle cells to become closer to the normal resting value. In this way insulin is believed to terminate an attack of contractures or paralysis in these patients. 6. Long-term administration of salbutamol, a β2-agonist, increases the activity of the Na+, K+-ATPase in skeletal muscle cells. In this way, salbutamol administraion leads to increased sequestration of K+ in muscle cells. Apparently this helps to prevent the K+ efflux that underlies episodes of hyperkalemia with resultant contractures that may be followed by periods of paralysis.

69
THANK YOU FOR YOUR ATTENTION!

Similar presentations











>")









 due to the asymmetrical.>")




