Download presentation
Presentation is loading. Please wait.

1
Lipoprotein Metabolism
Jack Blazyk

2
Most figures and tables are from Harper’s Illustrated Biochemistry 27th Edition (2006) web version by Robert K. Murray, Daryl K. Granner, and Victor W. Rodwell [Chapters 25 & 26] Click here for link

3
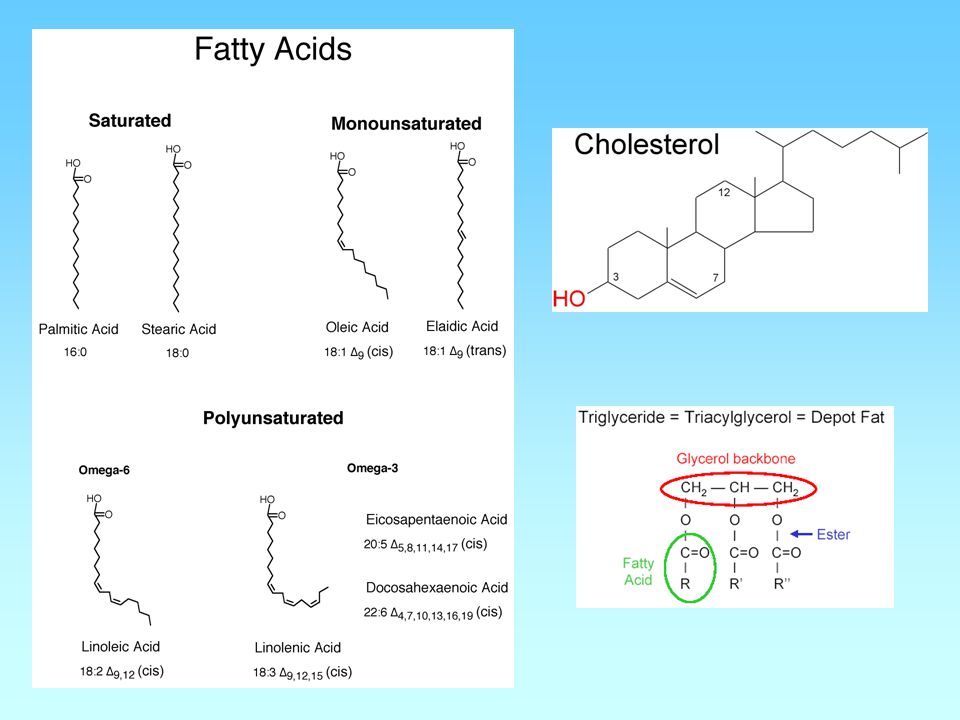
Lipids in the Blood Fatty Acids Bound to albumin
Cholesterol, Triglycerides and Phospholipids Transported by lipoproteins Cholesterol can be free or esterified Triglycerides must be degraded extracellularly to be absorbed by cells

5
Lipids in the Blood Phospholipids Phosphatidylcholine = Lecithin

6
Role of Cholesterol Component of cell membranes
Precursor of bile acids Precursor of steroid hormones

7
Metabolism of Cholesterol
Dietary or de novo synthesis Precursor is Acetyl-CoA Regulated by HMG-CoA reductase Receptor-mediated import

8
Anatomy of a Lipoprotein
Fig. 25-1

9
Apolipoproteins Structural determinants of lipoproteins
Enzyme cofactors Ligands for binding to lipoprotein receptors

10
Albumin / free fatty acids
Table 25–1. Composition of the Lipoproteins in Plasma of Humans. Lipoprotein Source Diameter (nm) Density (g/mL) Protein (%) Lipid (%) Main Lipid Components Apolipoproteins Chylomicrons Intestine 90–1000 < 0.95 1–2 98–99 Triacylglycerol A-I, A-II, A-IV,1 B-48, C-I, C-II, C-III, E Chylomicron remnants 45–150 < 1.006 6–8 92–94 Triacylglycerol, phospholipids, cholesterol B-48, E VLDL Liver (intestine) 30–90 0.95–1.006 7–10 90–93 B-100, C-I, C-II, C-III IDL 25–35 1.006–1.019 11 89 Triacylglycerol, cholesterol B-100, E LDL 20–25 1.019–1.063 21 79 Cholesterol B-100 HDL Liver, intestine, VLDL, chylomicrons Phospholipids, cholesterol A-I, A-II, A-IV, C-I, C-II, C-III, D,2 E HDL1 32 68 HDL2 10–20 1.063–1.125 33 67 HDL3 5–10 1.125–1.210 57 43 Preβ-HDL3 < 5 > 1.210 A-I Albumin / free fatty acids Adipose tissue > 1.281 99 1 Free fatty acids Abbreviations: HDL, high-density lipoproteins; IDL, intermediate-density lipoproteins; LDL, low-density lipoproteins; VLDL, very low density lipoproteins. 1Secreted with chylomicrons but transfers to HDL. 2Associated with HDL2 and HDL3 subfractions. 3Part of a minor fraction known as very high density lipoproteins (VHDL).
 Density (g/mL) Protein (%) Lipid (%) Main Lipid Components. Apolipoproteins. Chylomicrons. Intestine. 90–1000. < –2. 98–99. Triacylglycerol. A-I, A-II, A-IV,1 B-48, C-I, C-II, C-III, E. Chylomicron remnants. 45–150. < –8. 92–94. Triacylglycerol, phospholipids, cholesterol. B-48, E. VLDL. Liver (intestine) 30– – –10. 90–93. B-100, C-I, C-II, C-III. IDL. 25– – Triacylglycerol, cholesterol. B-100, E. LDL. 20– – Cholesterol. B-100. HDL. Liver, intestine, VLDL, chylomicrons. Phospholipids, cholesterol. A-I, A-II, A-IV, C-I, C-II, C-III, D,2 E. HDL HDL2. 10– – HDL3. 5– – Preβ-HDL3. < 5. > A-I. Albumin / free fatty acids. Adipose tissue. > Free fatty acids. Abbreviations: HDL, high-density lipoproteins; IDL, intermediate-density lipoproteins; LDL, low-density lipoproteins; VLDL, very low density lipoproteins. 1Secreted with chylomicrons but transfers to HDL. 2Associated with HDL2 and HDL3 subfractions. 3Part of a minor fraction known as very high density lipoproteins (VHDL).")
11
Fig. 25-2 The formation and secretion of (A) chylomicrons by an intestinal cell and (B) very low density lipoproteins by a hepatic cell. (RER, rough endoplasmic reticulum; SER, smooth endoplasmic reticulum; G, Golgi apparatus; N, nucleus; C, chylomicrons; VLDL, very low density lipoproteins; E, endothelium; SD, space of Disse, containing blood plasma.) Apolipoprotein B, synthesized in the RER, is incorporated into lipoproteins in the SER, the main site of synthesis of triacylglycerol. After addition of carbohydrate residues in G, they are released from the cell by reverse pinocytosis. Chylomicrons pass into the lymphatic system. VLDL are secreted into the space of Disse and then into the hepatic sinusoids through fenestrae in the endothelial lining.
 chylomicrons by an intestinal cell and (B) very low density lipoproteins by a hepatic cell. (RER, rough endoplasmic reticulum; SER, smooth endoplasmic reticulum; G, Golgi apparatus; N, nucleus; C, chylomicrons; VLDL, very low density lipoproteins; E, endothelium; SD, space of Disse, containing blood plasma.) Apolipoprotein B, synthesized in the RER, is incorporated into lipoproteins in the SER, the main site of synthesis of triacylglycerol. After addition of carbohydrate residues in G, they are released from the cell by reverse pinocytosis. Chylomicrons pass into the lymphatic system. VLDL are secreted into the space of Disse and then into the hepatic sinusoids through fenestrae in the endothelial lining.")
12
Triglyceride-Degrading Enzymes
LPL (Lipoprotein Lipase) LPL is extracellular on the walls of blood capillaries, anchored to the endothelium. Triacylglycerol (TG) is hydrolyzed to free fatty acids plus glycerol. Some of the released free fatty acids return to the circulation (bound to albumin) but the bulk is transported into the tissue (mainly adipose, heart, and muscle (80%), while about 20% goes indirectly to the liver.
 LPL is extracellular on the walls of blood capillaries, anchored to the endothelium. Triacylglycerol (TG) is hydrolyzed to free fatty acids plus glycerol. Some of the released free fatty acids return to the circulation (bound to albumin) but the bulk is transported into the tissue (mainly adipose, heart, and muscle (80%), while about 20% goes indirectly to the liver.")
13
Triglyceride-Degrading Enzymes
HL (Hepatic Lipase) HL is bound to the sinusoidal surface of liver cells, where it also hydrolyzes TG to free fatty acids plus glycerol. This enzyme, unlike LPL, does not react readily with chylomicrons or VLDL but is concerned with TG hydrolysis in chylomicron remnants and HDL metabolism.
 HL is bound to the sinusoidal surface of liver cells, where it also hydrolyzes TG to free fatty acids plus glycerol. This enzyme, unlike LPL, does not react readily with chylomicrons or VLDL but is concerned with TG hydrolysis in chylomicron remnants and HDL metabolism.")
14
Fig. 25-3 Metabolic fate of chylomicrons. (A, apolipoprotein A; B-48, apolipoprotein B-48; , apolipoprotein C; E, apolipoprotein E; HDL, high-density lipoprotein; TG, triacylglycerol; C, cholesterol and cholesteryl ester; P, phospholipid; HL, hepatic lipase; LRP, LDL receptor-related protein.) Only the predominant lipids are shown.
 Only the predominant lipids are shown.")
15
Fig. 25-4 Metabolic fate of very low density lipoproteins (VLDL) and production of low-density lipoproteins (LDL). (A, apolipoprotein A; B-100, apolipoprotein B-100; © apolipoprotein C; E, apolipoprotein E; HDL, high-density lipoprotein; TG, triacylglycerol; IDL, intermediate-density lipoprotein; C, cholesterol and cholesteryl ester; P, phospholipid.) Only the predominant lipids are shown. It is possible that some IDL is also metabolized via the LRP.
 and production of low-density lipoproteins (LDL). (A, apolipoprotein A; B-100, apolipoprotein B-100; © apolipoprotein C; E, apolipoprotein E; HDL, high-density lipoprotein; TG, triacylglycerol; IDL, intermediate-density lipoprotein; C, cholesterol and cholesteryl ester; P, phospholipid.) Only the predominant lipids are shown. It is possible that some IDL is also metabolized via the LRP.")
16
Enzymes and Transfer Proteins
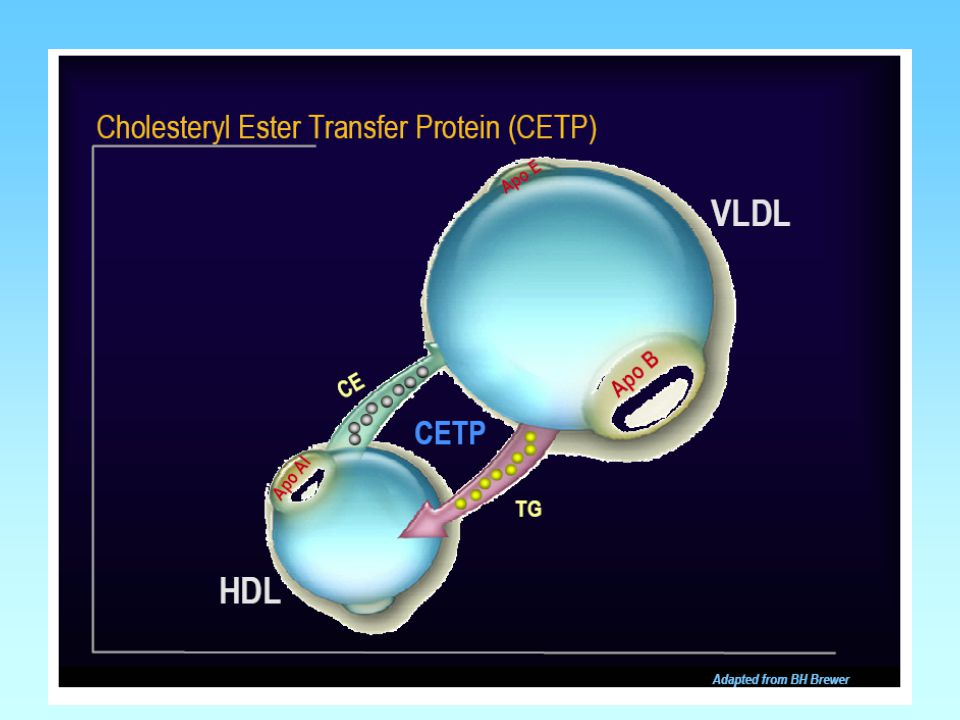
LCAT (Lecithin:Cholesterol Acyltransferase) Formation of cholesterol esters in lipoproteins ACAT (Acyl-CoA:Cholesterol Acyltransferase) Formation of cholesterol esters in cells CETP (Cholesterol Ester Transfer Protein)
 Formation of cholesterol esters in lipoproteins. ACAT (Acyl-CoA:Cholesterol Acyltransferase) Formation of cholesterol esters in cells. CETP (Cholesterol Ester Transfer Protein)")
17
Fig. 25-5 Metabolism of high-density lipoprotein (HDL) in reverse cholesterol transport. (LCAT, lecithin:cholesterol acyltransferase; C, cholesterol; CE, cholesteryl ester; PL, phospholipid; A-I, apolipoprotein A-I; SR-B1, scavenger receptor B1; ABCA 1, ATP binding cassette transporter A1.) Preβ-HDL, HDL2, HDL3 - see Table 25–1. Surplus surface constituents from the action of lipoprotein lipase on chylomicrons and VLDL are another source of pre -HDL. Hepatic lipase activity is increased by androgens and decreased by estrogens, which may account for higher concentrations of plasma HDL2 in women.
 in reverse cholesterol transport. (LCAT, lecithin:cholesterol acyltransferase; C, cholesterol; CE, cholesteryl ester; PL, phospholipid; A-I, apolipoprotein A-I; SR-B1, scavenger receptor B1; ABCA 1, ATP binding cassette transporter A1.) Preβ-HDL, HDL2, HDL3 - see Table 25–1. Surplus surface constituents from the action of lipoprotein lipase on chylomicrons and VLDL are another source of pre -HDL. Hepatic lipase activity is increased by androgens and decreased by estrogens, which may account for higher concentrations of plasma HDL2 in women.")
18
Fig. 26-5 Factors affecting cholesterol balance at the cellular level. Reverse cholesterol transport may be mediated via the ABCA 1 transporter protein (with preβ-HDL as the exogenous acceptor) or the SR-B1 (with HDL3 as the exogenous acceptor). (C, cholesterol; CE, cholesteryl ester; PL, phospholipid; ACAT, acyl-CoA:cholesterol acyltransferase; LCAT, lecithin:cholesterol acyltransferase; A-I, apolipoprotein A-I; LDL, low-density lipoprotein; VLDL, very low density lipoprotein.) LDL and HDL are not shown to scale.
 or the SR-B1 (with HDL3 as the exogenous acceptor). (C, cholesterol; CE, cholesteryl ester; PL, phospholipid; ACAT, acyl-CoA:cholesterol acyltransferase; LCAT, lecithin:cholesterol acyltransferase; A-I, apolipoprotein A-I; LDL, low-density lipoprotein; VLDL, very low density lipoprotein.) LDL and HDL are not shown to scale.")
19
Transport of cholesterol between the tissues in humans
Transport of cholesterol between the tissues in humans. (C, unesterified cholesterol; CE, cholesteryl ester; TG, triacylglycerol; VLDL, very low density lipoprotein; IDL, intermediate-density lipoprotein; LDL, low-density lipoprotein; HDL, high-density lipoprotein; ACAT, acyl-CoA:cholesterol acyltransferase; LCAT, lecithin:cholesterol acyltransferase; A-I, apolipoprotein A-I; CETP, cholesteryl ester transfer protein; LPL, lipoprotein lipase; HL, hepatic lipase; LRP, LDL receptor-related protein.) Fig. 26-6
 Fig")
20
Clinical Implications of Lipoproteins

21
Blood Lipid Levels

22
Blood Lipid Levels

23
Initial detailed analysis of plasma LDL in control subjects and CHD patients with hypertriglyceridemia and low HDL have revealed the presence of two distinct major lipoprotein phenotypes based on LDL subclasses. One subclass is characterized by a predominance of large buoyant LDL particles (pattern A), and the second subclass is characterized by small, dense LDL particles (pattern B). Pattern B is often associated with hypertriglyceridemia and low HDL, and is frequently referred to as the atherogenic lipoprotein profile. Franceschini, Am. J. Cardiol. 2001; 88 (12A): 9N-13N
: 9N-13N.")
24
LDL – Does Size Matter? “LDL size correlates positively with plasma HDL levels and negatively with plasma triglyceride concentrations, and the combination of small, dense LDL, decreased HDL cholesterol and increased triglycerides has been called the ‘atherogenic lipoprotein phenotype’. This partly heritable trait is a feature of the metabolic syndrome, and is associated with increased cardiovascular risk. LDL size seems to be an important predictor of cardiovascular events and progression of coronary artery disease, and a predominance of small, dense LDL has been accepted as an emerging cardiovascular risk factor by the National Cholesterol Education Program Adult Treatment Panel III. However, other authors have suggested that LDL subclass measurement does not add independent information to that conferred by the simple LDL concentration, along with the other standard risk factors.7 Thus it remains debatable whether to measure LDL particle size for cardiovascular risk assessment, and if so, in which categories of patients.” Rizzo & Berneis, Q. J. Med. 2006; 99:1-14.

25
From Medical Biochemistry, Baynes & Dominiczak, Mosby, 1999.

26
Genetic Disorders Familial Hypercholesterolemia Types
* Heterozygous FH (incidence 1:500-1,000) * Homozygous FH (incidence 1:1,000,000) Causes Both forms are caused by the same problem: a mutation in either the LDL receptor or the ApoB protein. There is one known ApoB defect (R3500Q) and a multitude of LDL receptor defects, the frequency of which is different for each population.
 * Homozygous FH (incidence 1:1,000,000) Causes. Both forms are caused by the same problem: a mutation in either the LDL receptor or the ApoB protein. There is one known ApoB defect (R3500Q) and a multitude of LDL receptor defects, the frequency of which is different for each population.")
27
From Medical Biochemistry, Baynes & Dominiczak, Mosby, 1999.

28
Statins Atorvastatin (Lipitor - Pfizer) Cerivastatin - (Baycol - Bayer) Fluvastatin (Lescol - Novartis) Lovastatin (Mevacor - Merck) Pravastatin (Pravachol - BMS) Rosuvastatin (Crestor - AstraZeneca) Simvastatin (Zocor- Merck)
 Cerivastatin - (Baycol - Bayer) Fluvastatin (Lescol - Novartis) Lovastatin (Mevacor - Merck) Pravastatin (Pravachol - BMS) Rosuvastatin (Crestor - AstraZeneca) Simvastatin (Zocor- Merck)")
29
Statins Atorvastatin (Lipitor - Pfizer) Withdrawn in Fluvastatin (Lescol - Novartis) Lovastatin (Mevacor - Merck) Pravastatin (Pravachol - BMS) Rosuvastatin (Crestor - AstraZeneca) Simvastatin (Zocor- Merck)
 Withdrawn in 2001 Fluvastatin (Lescol - Novartis) Lovastatin (Mevacor - Merck) Pravastatin (Pravachol - BMS) Rosuvastatin (Crestor - AstraZeneca) Simvastatin (Zocor- Merck)")
30
Statins Atorvastatin (Lipitor - Pfizer) Fluvastatin (Lescol - Novartis) Lovastatin (Mevacor - Merck) Pravastatin (Pravachol - BMS) Rosuvastatin (Crestor - AstraZeneca) Simvastatin (Zocor- Merck)
 Fluvastatin (Lescol - Novartis) Lovastatin (Mevacor - Merck) Pravastatin (Pravachol - BMS) Rosuvastatin (Crestor - AstraZeneca) Simvastatin (Zocor- Merck)")
31
Statins

33
Big Pharma Woes Statin patents are expiring Simvastatin (Zocor) – 2006
Lipitor – 2010 All statins by 2012 What to do? Convert to OTC (e.g., Mevacor) Combine with other drugs (e.g., Vytorin)
 Combine with other drugs (e.g., Vytorin)")
34
Your Health FDA Weighs Statin Drug Sales by Joanne Silberner Morning Edition, December 13, 2007 Statin drugs that lower cholesterol have become popular. Merck, which manufactures the statin drug, Mevacor, thinks its product is safe enough to be sold without a prescription. An advisory committee for the Food and Drug Administration will meet to discuss whether that is a good idea.

35
Vytorin Zetia Zocor

36
Disappointing results were announced from the long-awaited ENHANCE trial (completed in 2006) of the best-selling cholesterol drug Vytorin, which combines the unique cholesterol drug Zetia with the traditional statin drug Zocor (simvastatin). Vytorin was found to be no better than simvastatin alone for reducing plaque buildup in the carotid arteries. In fact, patients taking Vytorin actually had slightly more plaque buildup during the trial than those taking simvastatin alone.

37
1/15/08 – Steven E. Nissen, MD, chairman of the department of cardiovascular medicine at the Cleveland Clinic and a past president of the American College of Cardiology, called the results "a stunning reversal for Zetia and Vytorin." "Zetia works only by blocking the absorption of cholesterol, but it has not been shown to produce any health benefits," he says. "I have been skeptical of these drugs from the beginning because I wasn't sure that Zetia's mechanism of cholesterol lowering would produce the same benefits that we see with statins."

38
New Drugs Beyond Statins?

42
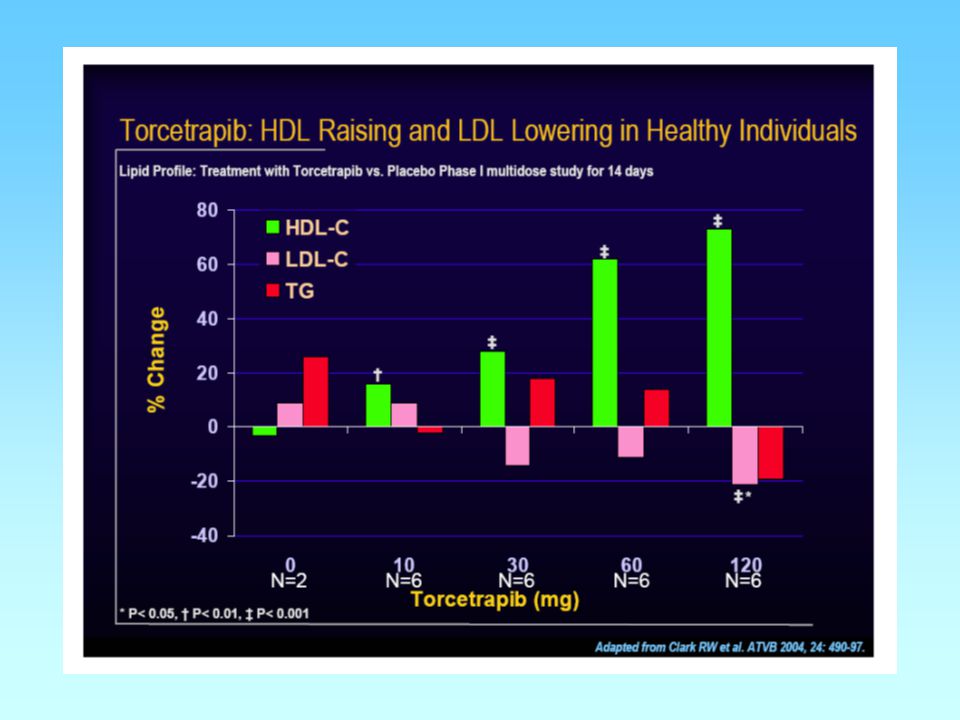
Pfizer - Torcetrapib CETP Inhibitor Development began around 1990
First administered in humans in 1999

44
Pfizer was developing a combination tablet containing torcetrapib, a cholesteryl ester transfer protein (CETP) inhibitor and high-density lipoprotein (HDL) cholesterol enhancer, with Lipitor (atorvastatin), for the potential treatment of atherosclerosis and hypercholesterolemia. Torcetrapib had been regarded as Pfizer's most important developmental drug and was predicted to become a top selling medicine in the cardiovascular market. Pfizer had invested $800 million in its development, with the hope that it would have become available before the 2011 patent expiry of its leading cardiovascular drug, Lipitor.

45
In December 2006, Pfizer announced that data from the ILLUMINATE trial showed that the combination of Lipitor plus torcetrapib was linked to a 60% increase in mortality rate and cardiovascular events compared to Lipitor alone. Pfizer subsequently discontinued the development of the drug following recommendations from the Data Safety Monitoring Board which was supervising the study. Since December, Pfizer eliminated 10,000 jobs (10% of its work force) and faced a corporate shakeup with the ouster of the head of R&D. Expectations for other CETP inhibitors under development are guarded, with intense scrutiny by the FDA, which will likely require very large Phase III trials in light of torcetrapib’s problems.
 and faced a corporate shakeup with the ouster of the head of R&D. Expectations for other CETP inhibitors under development are guarded, with intense scrutiny by the FDA, which will likely require very large Phase III trials in light of torcetrapib’s problems.")
Similar presentations







 LDL derived from VLDL as TAG in VLDL (and IDL) removed by lipoprotein lipase LDL major cholesterol-carrying lipoprotein.>")






>")





 are connected to a cyclopentane ring (D). Significantly different structure.>")