Download presentation
Presentation is loading. Please wait.

1
Long-Term Care Discussion Group May 24, 2012

2
National Commission for Quality Long-Term Care »Co-Chairs –Former Senator Bob Kerrey –Former Speaker Newt Gingrich –21 Commissioners »Quality »Workforce »Technology »Finance Funded by Leading Age, AHCA, Alliance for Quality Nursing Home Care

3
Mathematica Policy Research A Strategic Plan for LTQA »Potential for LTQA to make a difference by – –Facilitating dialogue and partnerships among all provider groups that serve people needing LTSS and help break down the silos –Bringing consumers and family caregivers together the LTSS providers and government agencies –Making stronger links between quality measurement goals and evidence based practices –Collaborating with other quality improvement organizations on common priorities and goals

4
»Launched January 30 th – Brookings Institution »30 member Board appointed – –Inagural Executive Committee Mary Naylor – Chair Carol Raphael – Vice-Chair Gail Hunt – Secretary Larry Minnix – Treasurer Mark McClellan – At large »Developed Statement of Principles

5
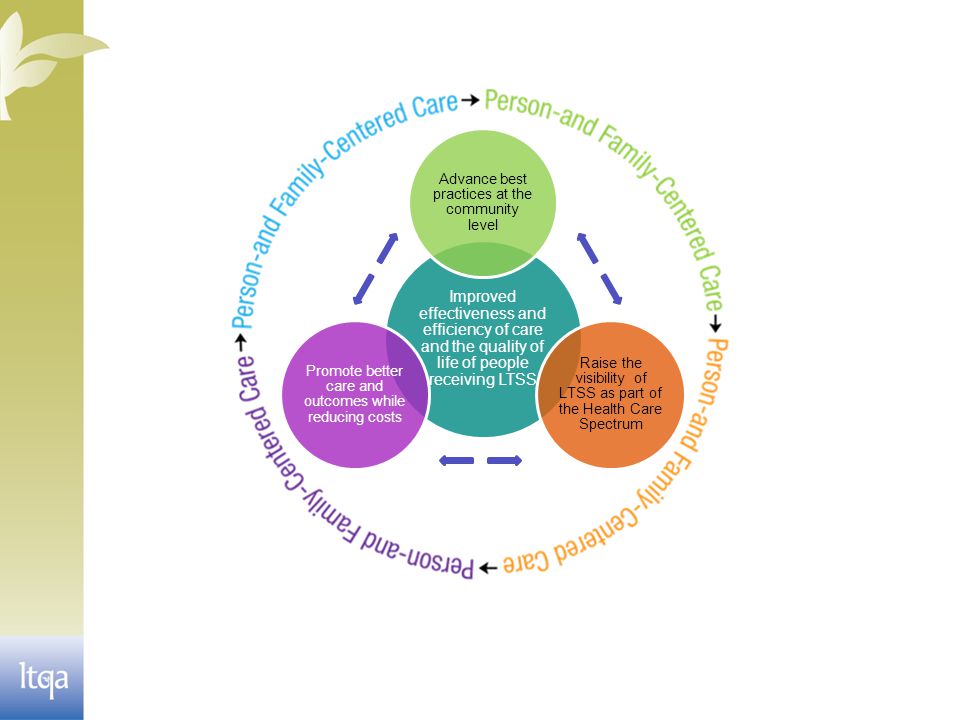
Mission Statement To improve the effectiveness and efficiency of care and the quality of life of people receiving long- term services and supports by fostering person- and family-centered quality measurement and advancing innovative best practices.

7
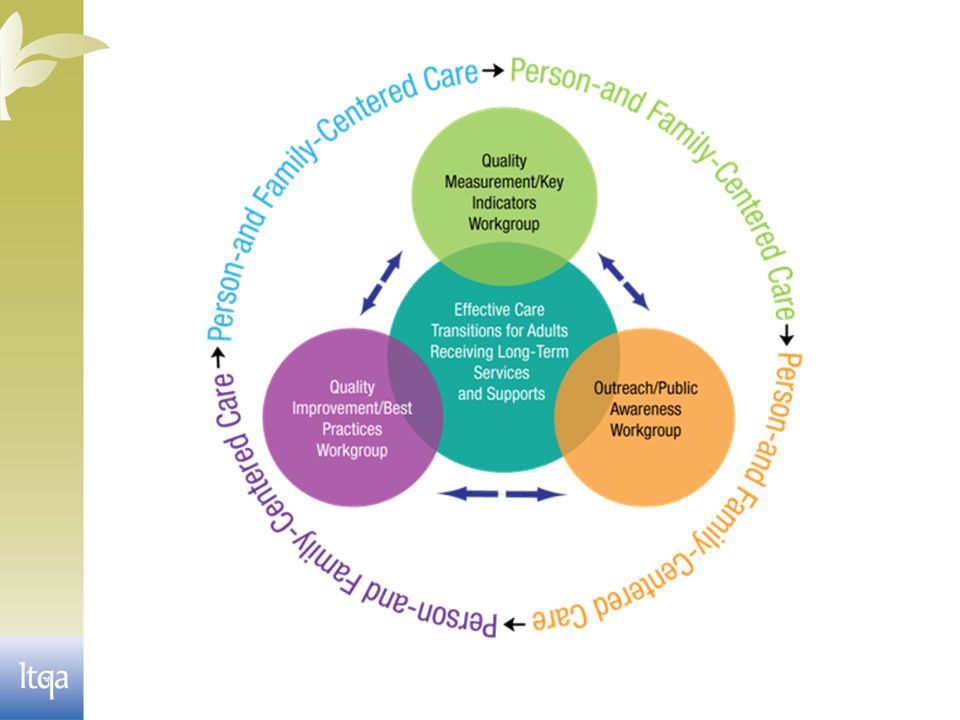
Strategic Agenda ( 2010-2012) Care transitions; impact on people’s health and QoL; effects on potentially avoidable hospitalizations, re-hospitalizations and total health care costs. Quality Measurement Key Strategy: Address a national health challenge, TRANSITIONS IN CARE, affecting people receiving LTSS in order to produce demonstrable improvement in quality and cost reductions Person- and family-centered, effective transitional care practices Quality Improvement Information and policies that advance high quality, person- and family-centered transitional care Outreach/Public Awareness

8
Members

10
GRANTS »The SCAN Foundation »The Commonwealth Fund »AHRQ- The Agency for Healthcare Research and Quality

11
Quality Measurement Workgroup Report » Achieved consensus on domains for measurement of transitional care in LTSS – Person/Family Centered Care – Transitional Care Processes – Performance Outcomes » Identified and recommended set of 12 transitional care measures » Identified gaps in measurement relevant to transitional care which represent areas for measure development and/or research

12
Gaps in Transitional Care Measurement » Person and family-centeredness (beyond clinical outcomes) » Process and outcome measures for older adults with cognitive impairment and those receiving palliative care » Transitional care management across episodes of care » Discharge readiness and social support » Preventive care » Access to, cost and cost-effectiveness of transitional care » Disparities and measures reflective of unique subpopulations » Performance of measure “bundle” 12
 » Process and outcome measures for older adults with cognitive impairment and those receiving palliative care » Transitional care management across episodes of care » Discharge readiness and social support » Preventive care » Access to, cost and cost-effectiveness of transitional care » Disparities and measures reflective of unique subpopulations » Performance of measure bundle 12")
13
Next Steps » These consensus-based recommendations synchronize and align with the work of NQF and Measures Application Partnership’s (MAP) roles in recommending measures to CMS » Initial testing of this set of measures can begin through additional LTQA programs including the launch of the Innovative Communities Initiative » Further research is needed to develop and test measures that address LTSS priorities 13
 roles in recommending measures to CMS » Initial testing of this set of measures can begin through additional LTQA programs including the launch of the Innovative Communities Initiative » Further research is needed to develop and test measures that address LTSS priorities 13")
14
White Paper on Preventable Hospitalizations » Although the decision to go to the hospital is often made in LTSS settings, there are no available validated measures to help long-term care organizations determine what is a preventable hospitalization. » The paper includes seven recommendations for the LTQA to pursue. These include: – Defining preventable hospitalizations in general instead of by setting. – Defining as precisely as possible the population receiving LTSS. – Beginning a process to develop appropriate measures or measure-based procedures to identify potentially preventable hospitalizations in the LTQA population. – Advocating for studies of measures. – Advocating with CMS for rigorous monitoring of programs designed to reduce preventable hospitalizations. – Expanding education for clinicians who trigger hospitalizations. – Advocating for expanded implementation of existing tools for reducing preventable hospitalizations.

15
Work In Review » Advancing Effective Care Transitions Among Older Adults Receiving Long-Term Services and Supports –Selected ACA Provisions—Impact on Transitions Among Older Adults Receiving LTSS Readmissions - Section 3025 Bundled payments – Section 3023 CCTP - Section 3026 »Two webinars This work is funded by The Commonwealth Fund

16
In Development »White Paper - Achieving Higher Value Person- Centered LTSS Through Statewide Payment and Delivery System Reform –Why do states need to ‘fix’ LTSS? –A vision for higher value, person-centered LTSS –Challenges in achieving higher value, person-centered LTSS –Description of statewide approaches and analysis of each in addressing core values and features of higher value, person-centered LTSS –Policy recommendations »Two webinars This work is funded by The Commonwealth Fund

17
How do communities navigate this transition? ? Nursing Home Assisted Living Rehabilitation Continuing Care Retirement Community Home County Council/ Department on Aging Area Agency on Aging Cooperative Extension Mental Health Provider Community Resource Connection Home Health Care Senior Center Adult Day Services Faith Community County Social Services

18
Community-Based Approach »Communities across the US are beginning to consider transitions of care as a community –based challenge that requires shared ownership and close collaboration across settings. » (Institute for Healthcare Improvement)
.")
19
Innovative Communities – Why? “Without the involvement of long-term services and supports, ACO’s or other new collaborative models of service delivery will not be able to achieve sustained quality improvements and reduced costs.” -Mark McClellan, MD, Ph.D CAST Chair Director, Engelberg Center for Health Care Reform Leonard D. Schaeffer Chair in Health Policy Studies Brookings Institution, Washington DC

20
Innovative Communities - Why? “…LTQA is convinced that the most important health reform victories will take place at the local level, in cities and towns… A broad range of community stakeholders…is needed to help older people and people with disabilities remain healthy and independent…” - “Innovative Communities: Breaking Down Barriers for the Good of Consumers and their Family Caregivers.” p.3

21
Innovative Communities Summit Philosophical Principles “Large-scale social change requires broad cross- sector coordination, yet the social sector remains focused on the isolated intervention of individual organizations.” -John Kania, Mark Kramer, “Collective Impact,” Stanford Social Innovation Review, Winter, 2011, p.36

22
Innovative Communities Summit Kania and Kramer* Five Conditions of Collective Success* »Common Agenda Shared vision for change. Common understanding of the problem. Joint approach to solution. »Shared Measurement Systems Agreement for success measures. Consistent data collection and indicators. Group accountability. Shared learning for success and failure.

23
Innovative Communities Summit Kania and Kramer* Five Conditions of Collective Success* »Mutually Reinforcing Activities Each party plays their unique role. Coordination of efforts. Mutual support. »Continuous Communications Trusting relationships. Common motivation regardless of sector. Regular meetings. Best solutions instead of self-interest. »Backbone Support Organization Separate organization of stakeholders. Coordination of leadership talent.

24
December 2010 Innovative Communities Summit » Participants in the inaugural meeting worked together to create a common vision for a more collaborative future for those who provide and those who receive care and services. » That vision, as outlined in our first report, called for: – Empowerment of consumers through a customized, coordinated life-care plan that is person-centered and developed with the involvement of family. – Development of community teams made up of equal partners and led by an independent and invested leadership. » To help make this vision a reality, participants in the 1st Innovative Communities Summit encouraged LTQA to: – Serve as a repository for information that could help local stakeholders create and support Innovative Communities at the local level. – Serve as a cheerleader for Innovative Communities by coaching fledgling communities and convening regular meetings to encourage sharing of ideas and best practices. – Help Innovative Communities identify federal and state sources of funding and offer them advice on ways to access that funding.

25
June 2011 Innovative Communities Summit » Summit participants represented – 20 Innovative Communities – 20 federal agencies – 15 state and local governments – 5 foundations – 7 consumers – 32 providers – 14 health-care purchasers and payers – 16 academicians » Leaders explored how LTQA can support Innovative Communities and how these communities can work together to improve care transitions and reduce unnecessary rehospitalizations. » 11 presenters facilitated panels and small- group discussions. Presenters represented three major categories of stakeholders: – Innovative Communities – National & State Support Programs – Private Foundations

26
The Health Care Innovation Challenge » Innovative Communities Initiative (ICI) –Engage 300 communities in an outcomes- oriented Collaborative Action Network (CAN) Measured Component –3 Domains – Change Management; Action- Oriented Improvement Skills; Best Practices/Enabling Technologies to – Reduce ED/Hospital use for target population –Request - $24,526,425 Save Medicare $78 M – net savings of $ 53M – ROI of 2.19
 –Engage 300 communities in an outcomes- oriented Collaborative Action Network (CAN) Measured Component –3 Domains – Change Management; Action- Oriented Improvement Skills; Best Practices/Enabling Technologies to – Reduce ED/Hospital use for target population –Request - $24,526,425 Save Medicare $78 M – net savings of $ 53M – ROI of 2.19")
27
3 rd Innovative Communities Summit

28
SO WHAT’S NEXT?

29
Don Berwick Brought ‘Triple Aim’ to CMS »Better Care for Individuals –Described by 6 dimensions listed in the IOM’s “Crossing the Quality Chasm” report - Safety, Effectiveness, Patient-Centeredness, Timeliness, Efficiency, Equity »Better Health for Populations –Through attacking “the upstream causes of so much of our ill health” »Reducing Per-Capita Costs

30
CMS Vision of Post-Acute Care » “ The person-centered post-acute system of the future will: –Optimize choice and control of services; –Ensure that placement decisions are based on patient needs; –Provide coordinated, high quality care with seamless transition between settings; –Reward excellence by reflecting performance on quality measures in payment; –Recognize the critical role of family care giving; and –Utilize health information technology

31
The Affordable Care Act

33
Long-Term Care Spending in the US Share of total spending, 2006 Medicaid 43% Medicare 18% Private insurance 7% Out-of-pocket 28% Other 4% Source: Avalere Health, the SCAN Foundation.

34
By 2030, more than 1/3 of the entire budget will be devoted to Medicare and Medicaid Source: The Center for American Progress. The Math is Clear: Reducing Our Long-Term Federal Budget Deficit Mean Enhancing Health Care Reform

36
Payment & Delivery System Reforms to Support a High Performance Health Care System »Accountable Care Organizations: Broad responsibility for quality and cost of patient care, rewards for quality, shared savings »Primary Care and Medical Homes: Expansion of current Medicare demonstration, new Medicare pilots, Medicaid initiatives »Value-based purchasing »More transparency on quality and cost »Prevention, health promotion, patient safety, hospital-acquired infections, quality »Center for Medicare and Medicaid Innovation » Source: The Commonwealth Fund, The New Wave of Innovation: How the Health Care System is Reformin g, (New York: Columbia Journalism Review, November, 2011).
.")
37
Health Care Table HospitalsGovernmentInsurancePharmaBusinessPhysiciansNursesLabor Special Interests LTSS

39
Doug Pace dpace@leadingage.org 202-508-9454 Abbey Ammerman aammerman@leadingage.org 202-508-9474 www.ltqa.org

Similar presentations