Download presentation
Presentation is loading. Please wait.

1
台北市立 萬芳醫院 Journal Reading Present: 住院醫師 陳志榮

2
Genomic Aberrations are Rare in Urothelial neoplasms of Patients 19 Years or Younger
PJ Wild,J Giedl, R Stoehr, K Junker, S Boehm, JMM van Oers, EC Zwarthoff, H Blaszyk, SW Fine,PA Humphrey, LP Dehner, MB Amin, JI Epstein and A Hartmann J Pathol 2006

3
Introduction Bladder cancer: Older people (sixth decade of life)
<20 year old: distinct unusual Prognostic value: not consensus, but favorable outcome mostly. The definition of “young”: ranging from <20 years to 40–45 years The frequently changing classification of urothelial neoplasms

4
Introduction The 2004 WHO classification 23 patients: ≦20 years
Urothelial neoplasms of low malignant potential (PUNLMP) or low-grade non-invasive papillary tumors Favorable clinical outcome
 or low-grade non-invasive papillary tumors. Favorable clinical outcome.")
5
Introduction The 2004 WHO Classification Papilloma
Papillary neoplasm of low malignant potential (PUNLMP) Low-grade papillary carcinoma High-grade papillary carcinoma
 Low-grade papillary carcinoma. High-grade papillary carcinoma.")
6
Patients and Method 14 patients: ≦20 years with urothelial neoplasms
Johns Hopkins Hospital, Barnes-Jewish Hospital, Washington-University Medical Center. Paraffin wax-embedded tumor tissue. 2004 WHO criteria : Urothelial papilloma (n = 1) PUNLMP (n = 7) pTa low-grade (n = 5) pTa high-grade (n = 1)
 PUNLMP (n = 7) pTa low-grade (n = 5) pTa high-grade (n = 1)")
7
Patients and Method FGFR3 and TP53 mutation screening.
Comparative genomic hybridization (CGH). Multicolour fluorescence in situ hybridization. Human papillomavirus (HPV) DNA. Microsatellite analysis: detection of microsatellite instability (MSI). Markers for loss of heterozygosity (LOH) located on chromosome arms 9p, 9q, and 17p. Immunohistochemistry: TP53, Ki-67, CK20, hMSH2, hMLH1 and hMSH6 (mismatch repair proteins).
. Multicolour fluorescence in situ hybridization. Human papillomavirus (HPV) DNA. Microsatellite analysis: detection of microsatellite instability (MSI). Markers for loss of heterozygosity (LOH) located on chromosome arms 9p, 9q, and 17p. Immunohistochemistry: TP53, Ki-67, CK20, hMSH2, hMLH1 and hMSH6 (mismatch repair proteins).")
8
Laser Microdissection and DNA Isolation:
5 μm tissue section Pure populations: >90% neoplastic bladder tumor cells Extracted normal and tumor DNA

9
LOH Analysis Whole genome amplification: LOH analysis :
Improved primer extension pre-amplification PCR with limited tumor/ normal cells LOH analysis : 9p21 (D9S304, D9S1751) 9q (D9S303, D9S747) 17p13.1 (p53Alu)
 9q (D9S303, D9S747) 17p13.1 (p53Alu)")
10
MSI Analysis MSI detection: PCR MSI:
2 mononucleotide repeats (BAT25, BAT26) 3 dinucleotide repeats (D5S346, D2S123, D17S250) BAT40 PCR MSI: Defined by the presence of new bands after PCR amplification of tumor DNA, which were not present in PCR products of the corresponding normal DNA.
 3 dinucleotide repeats (D5S346, D2S123, D17S250) BAT40. PCR. MSI: Defined by the presence of new bands after PCR amplification of tumor DNA, which were not present in PCR products of the corresponding normal DNA.")
11
TP53 Mutation Analysis Direct sequencing:
Exons 5 to 9 of the TP53 tumor suppressor gene 12/14 (86%) tumors
 tumors")
12
Immunohistochemistry
Tissue microarray: Tissue cores: diameter 1.2 mm of each paraffin block Mismatch repair proteins: hMSH2, hMLH1, and hMSH6 TP53, CK20, and Ki-67 Avidin–biotin peroxidase method

13
Immunohistochemistry
TP53 and Ki-67: Cutoff levels for 10%. CK20 staining: CK20 is a sensitive marker of urothelial differentiation. Normal (superficial staining pattern of umbrella cells). Abnormal (negative or more than 10% stained other than umbrella cells).
. Abnormal (negative or more than 10% stained other than umbrella cells).")
15
FGFR3 Mutation Analysis
The SNaPshot method Three regions of the FGFR3 gene comprising all FGFR3 mutations detected in bladder cancer so far were amplified simultaneously in a multiplex PCR reaction

16
FISH Analysis Chromosomes 3, 7, and 17: centromeric probes
Chromosomes 9p21(p16): deletions 6 μm deparaffinized tissue sections Hybridization Scoring: selected 50 nuclei according to morphological criteria using DAPI staining. Two investigators (JG, AH) independently
: deletions. 6 μm deparaffinized tissue sections. Hybridization. Scoring: selected 50 nuclei according to morphological criteria using DAPI staining. Two investigators (JG, AH) independently.")
17
FISH Analysis An Aberrant cell:
At least one out of three centromeric signals amplified (>2 signals per cell) Or 9p21 deleted Euploid: Polyploid cells (four signals of all the three probes) were regarded as normal p16 locus deletion: recognized if the signal number of 9p21 was more than 1 unit lower than the mean value of the centromeric signals.
 Or 9p21 deleted. Euploid: Polyploid cells (four signals of all the three probes) were regarded as normal. p16 locus deletion: recognized if the signal number of 9p21 was more than 1 unit lower than the mean value of the centromeric signals.")
18
FISH Analysis Cutoff point: threefold of the standard deviation of non-tumor urothelium (n = 10, data not shown) An aberrant case: >9 per 50 cells showed polysomy (>18% of the cells). deletion of p16: >7 per 50 cells (>14% of the cells) with relative deletion of 9p21.
. deletion of p16: >7 per 50 cells (>14% of the cells) with relative deletion of 9p21.")
20
Isolate eupoloid nucleus
7 17 3 p16 Isolate eupoloid nucleus Aneuploid nucleus with polysomy of chromosome 7 p16 deletion

21
Comparative genomic hybridization (CGH)
Degenerate oligonucleotide-primed PCR Labeling of tumor DNA (biotin-16-dUTP ) and normal DNA(digoxigenin-11-dUTP) Hybridization of tumor DNA and normal DNA: 1 μg + 50 μg of Cot-1 DNA on normal metaphases at 37 .C for 48 h.
 and normal DNA(digoxigenin-11-dUTP) Hybridization of tumor DNA and normal DNA: 1 μg + 50 μg of Cot-1 DNA on normal metaphases at 37 .C for 48 h.")
22
Comparative genomic hybridization (CGH)
Detection of fluorescent signals Software module for CGH (MetaSystems, Altlussheim, Germany) Loss of chromosomal region in the tumor DNA: Shifts of the CGH profile to the red borderline Gain of chromosomal region in the tumor DNA: Shifts to the green borderline
 Loss of chromosomal region in the tumor DNA: Shifts of the CGH profile to the red borderline. Gain of chromosomal region in the tumor DNA: Shifts to the green borderline.")
25
HPV DNA Analysis Nested primers : PCR MY09/MY11 MYN9/MYN10 CP65/CP70

26
Results One patient: All patients:
Recurrent papillomas (four additional papillomas). Bacillus Calmette–Guerin + mitomycin treatment course. All patients: Alive with no evidence of disease. Median follow-up of 3 years (6 months ~ 13 years). No molecular alternation: 8 of the 14 tumors,
. Bacillus Calmette–Guerin + mitomycin treatment course. All patients: Alive with no evidence of disease. Median follow-up of 3 years (6 months ~ 13 years). No molecular alternation: 8 of the 14 tumors,")
27
Result No mutations in FGFR3, deletions of chromosome arms 9p, 9q or 17p, MSI or MRP loss. FGFR3 mutation analysis: performed in 71% (10/14) Microsatellite studies: 8 cases: insufficient amounts of normal DNA HPV-DNA: not detected in 7 investigated tumors TP53 mutation: Only one tumor Non-sense mutation in exon 5 Simultaneous TP53 over-expression using immunohistochemistry.

28
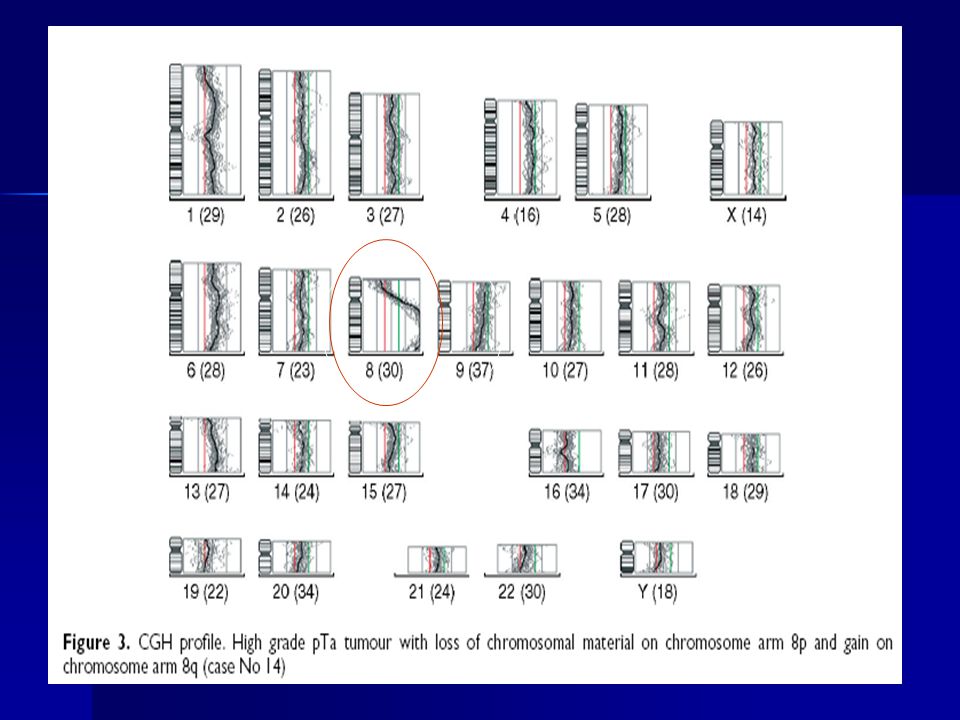
Result CGH analysis: One low-grade non-invasive papillary carcinoma:
Deletions of 7q, 9q and 15q Without any other genetic alterations. One high-grade tumor: Deletion of 8p and gain of 8q The remaining 12 tumors: No chromosomal alterations

29
Result FISH analysis: Immunohistochemical studies:
Three tumors both polysomy and relative deletions of chromosome 9p21 One PUNLMP, one low-grade tumor, and one High-grade tumor Either polysomy or p16 deletions: Other two low-grade tumors Immunohistochemical studies: Two tumors: Increased proliferative activity (10%) Two tumors:Abnormal (full-thickness) CK20 expression
 Two tumors:Abnormal (full-thickness) CK20 expression.")
31
Discussion (Outline) Relative absence of genetic changes, commonly found in urothelial carcinomas of adults. Absence of FGFR3 mutations and chromosome 9 alterations in most of the (low-grade) urothelial neoplasms tested. Previous changes commonly encountered in adults with low-grade urothelial neoplasm. Aged 20 years or younger: non-invasive papillary tumors (PUNLMP), and almost never recurred or progressed. The bladder tumors occurring in this age group are genetically stable, with only few molecular alteration characteristic of low grade tumors.
 urothelial neoplasms tested. Previous changes commonly encountered in adults with low-grade urothelial neoplasm. Aged 20 years or younger: non-invasive papillary tumors (PUNLMP), and almost never recurred or progressed. The bladder tumors occurring in this age group are genetically stable, with only few molecular alteration characteristic of low grade tumors.")
32
Discussion Eight papilloma or PUNLMP: One papillary high-grade tumor:
One (PUNLMP) with aneuploidy and p16 deletion. The other tumors: Genetically stable with a very low frequency of chromosomal alterations detected by CGH, a low level of aneuploidy, and only one TP53 mutation. One papillary high-grade tumor: Alterations with deletions 8p and gains 8q, aneuploidy, 9p21 deletions, and increased proliferation.
 with aneuploidy and p16 deletion. The other tumors: Genetically stable with a very low frequency of chromosomal alterations detected by CGH, a low level of aneuploidy, and only one TP53 mutation. One papillary high-grade tumor: Alterations with deletions 8p and gains 8q, aneuploidy, 9p21 deletions, and increased proliferation.")
33
Discussion Lack of FGFR3 mutations (4p16.3): An unexpected finding.
Characteristic for pTa tumours compared with pT2–4 tumors. Somatic FGFR3 mutations: Mis-sense mutations located in exons 7, 10, or 15. Germline FGFR3 mutations: associated with skeletal dysplasia syndromes. Constitutive receptor activation and have been linked to a lower risk of tumor recurrence in patients with a favorable disease course.

34
Discussion FGFR3 mutation in adult PTa tumor:
75% of papillomas, 85% of PUNLMP, and 88% of low-grade pTa tumours. Supporting these histological categories represent morphological variations of a single genetically stable tumor entity. Papillomas should be classified together with all well-differentiated urothelial neoplasms. van Rhijn et al Pathol 2002. Absence of FGFR3 mutations in this study: In children and young adult May represent a biologically distinct form of the disease

35
Discussion Infrequent deletions of chromosome 9 :
Another unusual finding Total or partial loss of chromosome 9. Most common cytogenetic alteration, occurring in about 50% of bladder cancers of all grades and stages. Supporting a different tumourigenic process in young patients. May not involve chromosomal instability and alterations of tumor suppressor genes or oncogenes.

36
Discussion ? Germline mutation ? in bladder tumors in children or young adults: No through the pathway of patients with germline mutations in mismatch repair genes (HNPCC syndrome) Urinary bladder tumor in these age group is unlike a manifestation of the HNPCC syndrome. Distinct lack of a history of cancer in our patients and their families.
 Urinary bladder tumor in these age group is unlike a manifestation of the HNPCC syndrome. Distinct lack of a history of cancer in our patients and their families.")
37
Discussion HPV infection of bladder is controversial.
Urol Res 1992 Pathologica 1994 Not seen in seven patients of this study with successful HPV PCR analysis. HPV does not seem to play an important role in bladder cancer .

38
Discussion TP53 mutation and urinary bladder tumor.
One study of 73 tumors in patients younger than 30 years: High frequency of TP53 nuclear staining in the majority of tumors, including those with low stage and grade. Suggested that TP53 immunoreactivity may not correlate with clinical outcome in all populations with bladder cancer. This study: only one tumor had a non-sense mutation in the TP53 gene together with positive TP53 immunoreactivity.

39
Discussion Proliferative activity: Migaldi et al :
Immunohistochemical proliferation markers. Young (<45 years) and older (>55 years) patients: Higher MIB1 expression levels: the elderly The lower proliferation rate may explain the overall better clinical course seen in young patients.
 and older (>55 years) patients: Higher MIB1 expression levels: the elderly. The lower proliferation rate may explain the overall better clinical course seen in young patients.")
40
Discussion CK20 expression pattern might be used in the identification of urothelial papillomas. All PUNLMPs in our study had normal urothelial differentiation, as indicated by CK20 expression.

41
Conclusion Urothelial neoplasms in people younger than 20 years are predominantly low grade and have a favourable clinical outcome. The genetic alterations often found in sporadic non-invasive urothelial bladder neoplasms of elderly patients are extremely rare in the young. HPV infection or a mutator phenotype and/or genetic predisposition within the HNPCC syndrome do not seem to play a role in urothelial tumourigenesis in this patient group. Urothelial neoplasms in young patients may represent a biologically distinct and genetically stable form of bladder disease in most cases.

42
Thank You for Your Attention!
台北市立 萬芳醫院 Thank You for Your Attention!

Similar presentations












. Outline Introduction to gene copy numbers and CGH technology DNA copy number alterations in breast cancer (Pollack.>")
, ER and ER ,>")









