Download presentation
Presentation is loading. Please wait.

1
CASEPRESENTATION ON FEMORAL SHAFT FRACTURE
PREPARED BY DHANYA VIJAYAN OPERATING ROOM

2
DEMOGRAPHIC DATA NAME : MR.M. K. Z AGE/SEX :19YRS/MALE IP NO :192407
DATE OF ADMISSION : 17/12/12 DIAGNOSIS :FEMORAL SHAFT FRACTURE SURGERY ON :INTRAMEDULLARY NAILING ON 18/12/12 DISCHARGED ON :30/12/12

3
PHYSICAL ASSESMENT GENERAL APPEARANCE
Patient is conscious and coherent. Looks weak and fatigue. Unable to mobilize his left lower extremity. VITAL SIGNS BP :124/86mm of Hg PR :82bpm RR :20cpm Temp :98.6F SPO2 :98%

4
Hair is equally disrtibuted. Absence of dandruff
SKIN Skin is warm . Has swelling on rt leg. Noted abrasions on rt arm and lower limbs HEAD Hair is equally disrtibuted. Absence of dandruff EYES Able to move both eyes On inspection of eyes ,the rt eye is reddish and the eyelid has dark discouloration .

5
Able to hear sounds clearly .
Patients pinna is same colour as fascial. Able to hear sounds clearly . No discharges. MOUTH Lips are pink but dry. Teeth is propely aligned with no dentures. NECK No tenderness of node

6
THORAX CARDIO VASCULAR GENITO URINARY
The Thorax Is Symmetric On Inspection CARDIO VASCULAR Absence Of Chest Pain . Heart sounds are clear. Upon auscultation his Bp is 132/78mmof hg. GENITO URINARY With foley catheter fr.16 . GASTRO INTESTINAL . No Tender Ness Of Abdomen and its soft . Had enema once and he was kept on NPO for 8hrs.

7
NEUROLOGIC Unable To Mobilize His Lt Lower Limb.
. MUSCULOSKELETAL Unable To Mobilize His Lt Lower Limb. Has Pain During Examination. Cannot Perform ADL. Tenderness at site of fracture. Visible deformity. Lower extremity appear shortened. Crepitus noted with movement. NEUROLOGIC Patient Is Mentally Alert And Oriented With Circumstances. Able To Follow Commands. No neurovascular deficit.

8
PATIENT HISTORY PAST MEDICAL AND SURGICAL HISTORY
H/O Adenotonsilectomy 10yrs back PRESENT MEDICAL HISTORY Patient was brought in E.R on 17/12/12 by RED CRESCENT due to R.T.A.After further investigations he was diagnosed with fracture on femoral shaft rt side. PRESENT SURGICAL HISTORY He underwent intramedullary nailing of lt femur on 18/12/12.

9
INVESTIGATIONS DONE FOR THE PATIENT
X-Ray Pelvic And Femur CT lower extremity CT lumbar and thoracic spine Blood investigations like CBC PT INR SERUM ELECTROLYTES RH TYPING

10
TREATMENT SURGICAL INTERVENTION :IM NAILING Inj .Risek 40mg od
MEDICATIONS Inj .Risek 40mg od Inj:Augmentin1.2gm Bd Inj.Amikacin 500mg bd Inj.Perfelgan 1 gm.

11
sodium Ab+ve LAB REPORTS PLT pottassium PT APTT INR RH typing
TEST on 17/12/12 RESULT REFERENCE RANGE CBC HB HCT RBC 12.1g/dl 35.8g/dl 4.81 g/dl g\dl *10^6/ul PLT 198 /ul sodium 138 mmol/l pottassium 4.0 mm0l/l PT 13.4 sec APTT 29.2 sec INR 1.3 2.4theraputic RH typing Ab+ve

12
FEMORAL SHAFT FRACTURE
TOPIC PRESENTATION FEMORAL SHAFT FRACTURE The femur is the anatomical name given to the thigh bone .It is the largest and strongest bone of the body. The long, straight part of the femur is called the femoral shaft. When there is a break anywhere along this length of bone, it is called a femoral shaft fracture. The most common types of femoral shaft fractures include: Transverse fracture. In this type of fracture, the break is a straight horizontal line going across the femoral shaft. b.Oblique fracture. This type of fracture has an angled line across the shaft.

13
d.Open or compound fracture
C.Spiral fracture. The fracture line encircles the shaft like the stripes on a candy cane. A twisting force to the thigh causes this type of fracture. d.Open or compound fracture If a bone breaks in such a way that bone fragments stick out through the skin or a wound penetrates down to the broken bone, the fracture is called an open or compound fracture. They have a higher risk for complications — especially infections— and take a longer time to heal. e.Comminuted fracture In this type of fracture, the bone has broken into three or more pieces.

14
open fracture

15
ANATOMY AND PHYSIOLOGY

16
The femur is the longest and strongest bone in the skeleton, is almost perfectly cylindrical in the greater part of its extent It is divisible into a body and two extremities . The Upper Extremity (proximal extremity), presents a head, a neck, a greater and a lesser trochanter The Head (caput femoris). is globular and forms rather more than a hemisphere and fits in to the acetabulam (a cup shaped socket in the pelvis) . The Neck (collum femoris).—The neck is a flattened pyramidal process of bone, connecting the head with the body The Greater Trochanter (trochanter major; great trochanter) is a large, irregular, quadrilateral eminence, situated at the junction of the neck with the upper part of the body. The Lesser Trochanter (trochanter minor; small trochanter) is a conical eminence it projects from the lower and back part of the base of the neck. Running obliquely downward and medialward from the tubercle is the intertrochanteric line (spiral line of the femur)
, presents a head, a neck, a greater and a lesser trochanter. The Head (caput femoris). is globular and forms rather more than a hemisphere and fits in to the acetabulam (a cup shaped socket in the pelvis) . The Neck (collum femoris).—The neck is a flattened pyramidal process of bone, connecting the head with the body. The Greater Trochanter (trochanter major; great trochanter) is a large, irregular, quadrilateral eminence, situated at the junction of the neck with the upper part of the body. The Lesser Trochanter (trochanter minor; small trochanter) is a conical eminence it projects from the lower and back part of the base of the neck. Running obliquely downward and medialward from the tubercle is the intertrochanteric line (spiral line of the femur)")
17
It consists of two oblong eminences known as the condyles
The Body or Shaft (corpus femoris).—The body, almost cylindrical in form, is a little broader above than in the center, broadest and somewhat flattened from before backward below. it is strengthened by a prominent longitudinal ridge, the linea aspera. The distal extremity of the femur (or lower extremity) is larger than the proximal extremity It consists of two oblong eminences known as the condyles Anteriorly, the condyles are slightly prominent and are separated by a smooth shallow called the patellar surface. posteriorely they project considerably and a deep notch, the Intercondylar fossa of femur, is present between them. The lateral condyle is the more prominent and is the broader both in its antero-posterior and transverse.
.—The body, almost cylindrical in form, is a little broader above than in the center, broadest and somewhat flattened from before backward below. it is strengthened by a prominent longitudinal ridge, the linea aspera. The distal extremity of the femur (or lower extremity) is larger than the proximal extremity. It consists of two oblong eminences known as the condyles. Anteriorly, the condyles are slightly prominent and are separated by a smooth shallow called the patellar surface. posteriorely they project considerably and a deep notch, the Intercondylar fossa of femur, is present between them. The lateral condyle is the more prominent and is the broader both in its antero-posterior and transverse.")
18
Each condyle is surmounted by an elevation, the epicondyle
The lateral condyle is the more prominent and is the broader both in its antero-posterior and transverse. Each condyle is surmounted by an elevation, the epicondyle The medial epicondyle is a large convex eminence to which the tibial collateral ligament of the knee-joint is attached. The lateral epicondyle, smaller and less prominent than the medial, gives attachment to the fibular collateral ligament of the knee-joint. The articular surface of the lower end of the femur occupies the anterior, inferior, and posterior surfaces of the condyles. Its front part is named the patellar surface and articulates with the patella.

19
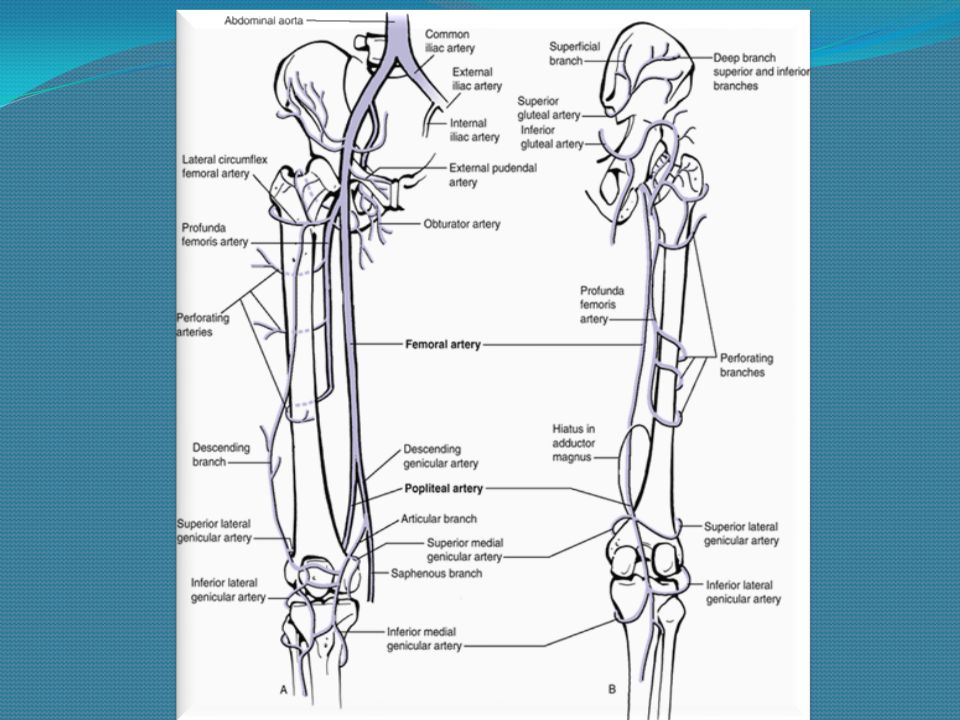
BLOOD SUPPLY TO THE FEMUR
THE FEMORAL ARTERY PASSES roundthe medial aspect of the femur to enter the popiliteal space where it becomes the popiliteal artery .it supplies blood to the structures of the thigh. Branches from the femoral artery Deep artery of the thigh (arteriaprofunda femoris) is the largest and main branch of the femoral artery and branches off the femoral artery about 2 to 5 cm below the inguinal ligament. Medial circumflex artery and lateral circumflex artery may arise from the deep artery or directly from the femoral artery. Great saphenous vein joins the femoral vein about 3 cm below the inguinal ligament Deep vein of the thigh (profunda femoris vein) joins the femoral vein about 8cm below the inguinal ligament.
 is the largest and main branch of the femoral artery and branches off the femoral artery about 2 to 5 cm below the inguinal ligament. Medial circumflex artery and lateral circumflex artery may arise from the deep artery or directly from the femoral artery. Great saphenous vein joins the femoral vein about 3 cm below the inguinal ligament. Deep vein of the thigh (profunda femoris vein) joins the femoral vein about 8cm below the inguinal ligament.")
21
MUSCLES The muscles in the front of the thigh are the sartorius and the quadriceps femoris. T he quadriceps is actually a powerful muscle made of 4 parts – the rectus femoris, vastus lateralis, vastus medialis and vastus intermedius. While the sartorius flexes both the hip and knee joints, the quadriceps femoris is an extensor of the knee joint. The muscles in the inner aspect of the thigh are the pectineus, gracilis, adductor longus, adductor magnus, adductor brevis, obturator externus The adductor muscles also help rotate the thigh in an inward direction while the iliopsoas flexes the hip joint . The back of the thigh holds the powerful hamstring muscles, the biceps femoris, semitendinosus and semimembranosus. nd the iliopsoas. The hamstrings are all flexors of the knee joint.

22
(superiorly) the inguinal ligament
The important nerves of the thigh are the femoral and the sciatic nerves The femoral triangle is an anatomical region of the upper inner human thigh. It is bounded by: (superiorly) the inguinal ligament (medially) the medial border of the adductor longus muscle (laterally) the medial border of the sartorius muscle The three compartments of the femoral sheath (From lateral to medial): femoral artery and its branches femoral veins and its tributaries femoral canal, Which contains lymphatic vessels and some lymph nodes (Specifically, the deep inguinal lymph nodes
 the inguinal ligament. (medially) the medial border of the adductor longus muscle. (laterally) the medial border of the sartorius muscle. The three compartments of the femoral sheath (From lateral to medial): femoral artery and its branches. femoral veins and its tributaries. femoral canal, Which contains lymphatic vessels and some lymph nodes (Specifically, the deep inguinal lymph nodes.")
23
ETIOLOGY SIGNS AND SYMPTOMS
due to a fall (usually from a height and often on to hard surface) due to direct blow to femur such as rta osteo porosis or malignan SIGNS AND SYMPTOMS Common Symptoms Are BLEEDING DEFORMITY OF THE LEG INABILITY TO MOVE THE AFFECTED LEG MUSCLE SPASMS NUMBNESS Or TINGLING SEVERE PAIN SWELLING
 due to direct blow to femur such as rta. osteo porosis or malignan. SIGNS AND SYMPTOMS. Common Symptoms Are. BLEEDING. DEFORMITY OF THE LEG. INABILITY TO MOVE THE AFFECTED LEG. MUSCLE SPASMS. NUMBNESS Or TINGLING. SEVERE PAIN. SWELLING.")
24
CONTUSION OR LOC EVEN FOR A BRIEF MOMENT HEAVY UNCONTROLLABLE BLEEDING
SERIOUS SYMPTOMS THAT MIGHT INDICATE A LIFE THREATENING CONDITION ARE. CONTUSION OR LOC EVEN FOR A BRIEF MOMENT HEAVY UNCONTROLLABLE BLEEDING INAVBILITY TO MOVE LEG HYPOTENSION PROTRUDING FRAGMENTS OF BONE THROUGH THE sKIN

25
TREATMENT Nonsurgical Treatment Surgical Treatment
Most femoral shaft fractures require surgery to heal. It is unusual for femoral shaft fractures to be treated without surgery. Very young children are sometimes treated with a cast. For the time between initial emergency care and surgery, doctor will place leg either in a long-leg splint or in skeletal traction. This is to keep broken bones as aligned as possible and to maintain the length of leg. (Skeletal traction is a pulley system of weights and counterweights that holds the broken pieces of bone together. It keeps leg straight and often helps to relieve pain.) EXTERNAL FIXATION External fixation is usually a temporary treatment for femur fractures. This device is stabilizing frame that holds the bones in the proper position so they can heal. Extensive comminution and open fractures were considered to be relative indications for the use of femoral external fixation as a definitive treatment for femoral shaft fractures. Surgical Treatment
 EXTERNAL FIXATION. External fixation is usually a temporary treatment for femur fractures. This device is stabilizing frame that holds the bones in the proper position so they can heal. Extensive comminution and open fractures were considered to be relative indications for the use of femoral external fixation as a definitive treatment for femoral shaft fractures. Surgical Treatment.")
26
PLATE AND SCREWS IM NAILING
INTRAMEDULLARY NAILING. It is the most common treatment for femoral shaft fractures in adults,An intramedullary nail can be inserted into the canal either at the hip or the knee through a small incision. It is screwed to the bone at both ends. This keeps the nail and the bone in proper position during healing. to determine how PLATE AND SCREWS EXTERN AL FIXATION PLATE AND SCREWS The use of plate fixation for the routine treatment of femoral shaft fractures has decreased with the increased use of intramedullary nails. The main disadvantages associated with plate fixation when compared with intramedullary nailing are the need for an extensive surgical approach with its associated blood loss, infectious complications, and soft tissue insult. Because the plate is a load-bearing implant, implant failure is expected if union does not occur. IM NAILING

27
COMPLICATIONS Complications from Femoral Shaft Fractures
The ends of broken bones are often sharp and can cut or tear surrounding blood vessels or nerves. Acute compartment syndrome may develop. (This is a painful condition that occurs when pressure within the muscles builds to dangerous levels. This pressure can decrease blood flow, which prevents nourishment and oxygen from reaching nerve and muscle cells. Unless the pressure is relieved quickly, permanent disability may result. This is a surgical emergency.) Open fractures expose the bone to the outside environment. Even with good surgical cleaning of the bone and muscle, the bone can become infected. Bone infection is difficult to treat and often requires multiple surgeries . Complications from Surgery. Infection. Injury to nerves and blood vessels. Blood clots. Fat embolism (bone marrow enters the blood stream and can travel to the lungs; this can also happen from the fracture itself without surgery). Malalignment or the inability to correctly position the broken bone fragments. Delayed union or nonunion (when the fracture heals slower than usual or not at all). Hardware irritation (sometimes the end of the nail or the screw can irritate the overlying muscles and tendons.)
 Open fractures expose the bone to the outside environment. Even with good surgical cleaning of the bone and muscle, the bone can become infected. Bone infection is difficult to treat and often requires multiple surgeries . Complications from Surgery. Infection. Injury to nerves and blood vessels. Blood clots. Fat embolism (bone marrow enters the blood stream and can travel to the lungs; this can also happen from the fracture itself without surgery). Malalignment or the inability to correctly position the broken bone fragments. Delayed union or nonunion (when the fracture heals slower than usual or not at all). Hardware irritation (sometimes the end of the nail or the screw can irritate the overlying muscles and tendons.)")
28
NURSING INTERVENTIONS
1.Provide emergency care if requires (hemostasis, respiratory care, prevention of shock). 2. Provide fracture fixation to prevent following injury of tissues. 3. Observe signs of fat embolism (especially during first 48 hours after the fracture). 4. Monitor fluids input and output continuously, insert IV catheter, urinary catheter. 5. Monitor client’s vital signs. 6. Monitor client’s laboratory tests results for abnormal values. 7. Administer IV therapy, analgesics, antibiotics, and other medications as prescribed. 8. Prepare client and his family for surgical intervention if required. 9. For client after surgical intervention provide routine postoperative care and teach about possible postoperative complications. 10. Provide care to client with cast (observe signs of circulatory impairment – change in skin color and temperature, diminished distal pulses, pain and swelling of the extremity; protect the cast from damage). 11. Provide care to client in traction (check the weights are hanging freely, observe skin for irritation and site of skeletal traction insertion for signs of infection; use aseptic technique when cleaning the site of insertion). 12. In case of hip fracture and hip replacement maintain the adduction of the affected extremity. 13. Provide respiratory exercises to prevent lung complications. 14. Observe for signs of thrombophlebitis, report immediately. 15. Provide appropriate skin care to prevent pressure sores. 16. Encourage fluid intake and high-protein, high-vitamin, high-calcium diet.
. 2. Provide fracture fixation to prevent following injury of tissues. 3. Observe signs of fat embolism (especially during first 48 hours after the fracture). 4. Monitor fluids input and output continuously, insert IV catheter, urinary catheter. 5. Monitor client’s vital signs. 6. Monitor client’s laboratory tests results for abnormal values. 7. Administer IV therapy, analgesics, antibiotics, and other medications as prescribed. 8. Prepare client and his family for surgical intervention if required. 9. For client after surgical intervention provide routine postoperative care and teach about possible postoperative complications. 10. Provide care to client with cast (observe signs of circulatory impairment – change in skin color and temperature, diminished distal pulses, pain and swelling of the extremity; protect the cast from damage). 11. Provide care to client in traction (check the weights are hanging freely, observe skin for irritation and site of skeletal traction insertion for signs of infection; use aseptic technique when cleaning the site of insertion). 12. In case of hip fracture and hip replacement maintain the adduction of the affected extremity. 13. Provide respiratory exercises to prevent lung complications. 14. Observe for signs of thrombophlebitis, report immediately. 15. Provide appropriate skin care to prevent pressure sores. 16. Encourage fluid intake and high-protein, high-vitamin, high-calcium diet.")
29
NURSING MANAGEMENT CLOSED FRACTURES Instruct the patient regarding the proper methods to control pain and edema (elevate extremity to heart level,take analgesia as prescribed etc). Teach patient how to use assistive devices safely. teach exercises to maintain the health of unaffected muscles and to strengthen muscles needed for transferring and for using assistive devices (crutches,walker). provide health teaching regarding self care ,medication information,monitoring potential complications . need for continuing health care supervision . OPEN FRACTURES Administer IV antibiotics immediately upon the patients arrival in hospital Perform wound irrigation and debridement . Asses neurovascular status frequently Take the patient temperature regularly and monitor signs of infection (The objective of the management is to prevent infection and promote healing of bone and tissue.)
. Teach patient how to use assistive devices safely. teach exercises to maintain the health of unaffected muscles and to strengthen muscles needed for transferring and for using assistive devices (crutches,walker). provide health teaching regarding self care ,medication information,monitoring potential complications . need for continuing health care supervision . OPEN FRACTURES. Administer IV antibiotics immediately upon the patients arrival in hospital. Perform wound irrigation and debridement . Asses neurovascular status frequently. Take the patient temperature regularly and monitor signs of infection. (The objective of the management is to prevent infection and promote healing of bone and tissue.)")
30
PRIORITIZATION OF NURSING PROBLEMS
1.Acute Pain Related To Fracture And Surgery. 2. Impaired Physical Mobility Secondary To Fracture And Surgery. 3.Knowledge Deficit Regarding Treatment Regimen And Disease Condition. 4.Risk For Fat Embolism Due To Fractutre Of Long Bones. 5.Risk For Infection Due To Surgical Intervention And Injury .

31
No pain and discomfort Subjective
ASSESSMENT PLANNING IMPEMENTATION EVALUATION CUES/EVIDENCE NURSING DIAGNOSIS GOALS AND DESIRED OUTCOME NURSING ORDER/ACTION RATIONAL FOR ACTION Subjective “I have severe pain while moving my lower limb” as verbalized by the patient Pain scale - 5/10 as 0 is the lowest and 10/10 is the highest objective Facial grimace Verbal report of pain. Acute Pain Related To Fracture And Surgery. After series of nursing interventions the client should manifest a decrease in pain scale from 5/10 to 0/10. 1.Asses the patients pain scale and perception. 2.Monitor vital signs and pain scale . 3.Maintain immobilization of affected part using cast,and skin traction. 4.Elevate and support injured extremity. 5.Teach divertional activities 6.Administer analgesia as prescribed . 1.To identify the onset ,intensity and duration of pain. 2.To obtain base line vital signs . (Vital signs changes during pain and for future comparison after intervention. 3.Relieves pain and prevents bone displacement and extension of tissue injury . 4.Promotes venous return, decreases edema, and may reduce pain. 5.To destract clients attention from pain. 6.To relieve the pain. After 12 Hrs Of Nursing Interventions The Goals Were Met As Evidenced By- Decrease in Pain scale from 5/10 to 0/10 No pain and discomfort Verbalize relief of pain. Positive response during evaluation. Display relaxed manner, able to participate in activities, and sleep and rest appropriately. Pain Control

32
Participates in activities of daily living
ASSESMENT PLANNING IMPLEMENTATION EVALUATION CUES/EVIDENCE NURSING DIAGNOSIS GOALS AND DESIRED OUTCOME NURSING ORDER/ACTION RATIONAL FOR ACTION SUBJECTIVE ‘’ I cannot move my leg properly and I have pain during motion ‘’ as verbaluized by the patient. OBJECTIVE Limited range of motion. Inability to perform action as instructed. with cast on left leg . decreased IMPAIRED PHYSICAL MOBILITY ,ACUTE PAIN SECONDARY TO FRACTURE AND SURGERY Patient will be able to Perform his physical activity and free of complications as evidenced by …. Participates in activities of daily living Performs physical activities independently Intact skin and abcence of thrombophlebitis Normal bowel pattern. 1.Support affected part using pillows. Provide footboard, wrist splints, trochanter. 2.Determine presence of complications related to immobility such as pneumonia ,elimination problem ,decubitus ulcer. 3.Encourage adequate intake of fluids 2-3L/day 4.Instruct /assist patient with active and passive ROM excercises of affected and unaffected limb like flexion,extension abduction and adduction. 1.To maintain position and function and reduce risk of pressure ulcers. . 2.To assess presence of complications 3.Promote well being and maximize and energy production... 4.Increases blood flow to muscles and bone to improve muscle tone, maintain joint mobility; prevent contractures/atro phy and calcium resorption from disuse . AFTER 12 HOURS OF NURSING INTERVENTIONS THE GOALS WERE MET AS EVIDENCED BY… Patient performs physical activities independently or with assistive devices as needed. Free of complications of immobility as evidenced by intact skin ,absence of thrombophlebitis ,normal bowel pattern Pt able to fully complete passive range of motion exercises withassistance from the staff by the end of this shift. Pt did not complain of any pain associated with exercise session.

33
Conclusion Bibiliography
A case of RTA patient with fracture of femoral shaft and was unable to move his left lower extremity. Initially patient was on skin traction. Surgical treatment Intra Medullary Nailing done on 18/12/12. Patient is able to move on walker. Health education given on home care including physiotherapy . Patient was discharged on 30/12/2012. Patient was told to come for follow-up after 2 weeks. Bibiliography 1.Lippincott manual of nursing practices 9 th edition. 2. health.com. 3.ortho info.aas.org. 4.Gray”s femur anatomy and physiology of human body. 5. type .com

34
THANK YOU THANK YOU

Similar presentations













 Joint>")





