Download presentation
Presentation is loading. Please wait.

1
A NEW FAMILY-BASED TREATMENT FOR ANOREXIA AND BULIMIA IN ADOLESCENTS Cris Haltom, Ph.D. Eating Disorder Recovery Center of Western NY Oct. 5, 2007 A NEW FAMILY-BASED TREATMENT FOR ANOREXIA AND BULIMIA IN ADOLESCENTS Cris Haltom, Ph.D. Eating Disorder Recovery Center of Western NY Oct. 5, 2007

2
The trouble with parentectomies: old thinking revised Minuchin and colleagues (1975) found family involvement helped patients with anorexia Minuchin and colleagues (1975) found family involvement helped patients with anorexia Dare and Eisler at the Maudsley Hospital in London built on Minuchin et al’s work: families recruited as necessary for recovery Dare and Eisler at the Maudsley Hospital in London built on Minuchin et al’s work: families recruited as necessary for recovery Radical change and new paradigm: parents supervise eating Radical change and new paradigm: parents supervise eating
 found family involvement helped patients with anorexia Minuchin and colleagues (1975) found family involvement helped patients with anorexia Dare and Eisler at the Maudsley Hospital in London built on Minuchin et al’s work: families recruited as necessary for recovery Dare and Eisler at the Maudsley Hospital in London built on Minuchin et al’s work: families recruited as necessary for recovery Radical change and new paradigm: parents supervise eating Radical change and new paradigm: parents supervise eating")
3
Research support for FBT Randomized controlled trials indicate 70-80% of adolescents with anorexia do well, when treated early, with weight restoration, normalization of eating-related thoughts and behaviors, and psychosocial functioning (LeGrange et al, 1992; Eisler et al, 2000; Lock et al, 2005) Randomized controlled trials indicate 70-80% of adolescents with anorexia do well, when treated early, with weight restoration, normalization of eating-related thoughts and behaviors, and psychosocial functioning (LeGrange et al, 1992; Eisler et al, 2000; Lock et al, 2005) Two large controlled trials of FBT for adolescents with bulimia support using FBT (LeGrange and Lock, 2007, LeGrange and Schmidt, 2005) Two large controlled trials of FBT for adolescents with bulimia support using FBT (LeGrange and Lock, 2007, LeGrange and Schmidt, 2005)
 Randomized controlled trials indicate 70-80% of adolescents with anorexia do well, when treated early, with weight restoration, normalization of eating-related thoughts and behaviors, and psychosocial functioning (LeGrange et al, 1992; Eisler et al, 2000; Lock et al, 2005) Two large controlled trials of FBT for adolescents with bulimia support using FBT (LeGrange and Lock, 2007, LeGrange and Schmidt, 2005) Two large controlled trials of FBT for adolescents with bulimia support using FBT (LeGrange and Lock, 2007, LeGrange and Schmidt, 2005)")
4
Overview Who, why, where, what and when of the Maudsley approach or FBT Who, why, where, what and when of the Maudsley approach or FBT Review three phases of Family-Based Treatment (FBT) Review three phases of Family-Based Treatment (FBT) Comparison with traditional family treatment model Comparison with traditional family treatment model Harnessing parents’ anxiety Harnessing parents’ anxiety Facilitating positive parent characteristics Facilitating positive parent characteristics When not to use FBT When not to use FBT Important differences between AN and BN Important differences between AN and BN Description of Phases I and II Description of Phases I and II Transitioning to adolescent autonomy Transitioning to adolescent autonomy What patients and parents have to say What patients and parents have to say
 Review three phases of Family-Based Treatment (FBT) Comparison with traditional family treatment model Comparison with traditional family treatment model Harnessing parents’ anxiety Harnessing parents’ anxiety Facilitating positive parent characteristics Facilitating positive parent characteristics When not to use FBT When not to use FBT Important differences between AN and BN Important differences between AN and BN Description of Phases I and II Description of Phases I and II Transitioning to adolescent autonomy Transitioning to adolescent autonomy What patients and parents have to say What patients and parents have to say")
5
Parents are necessary Included: family is the best resource Included: family is the best resource Empowered: parents challenge/disrupt disordered eating behaviors Empowered: parents challenge/disrupt disordered eating behaviors Informed: parents given information about ED’s as part of therapy, e.g., medical/psych. problems Informed: parents given information about ED’s as part of therapy, e.g., medical/psych. problems Prepared: join with the therapist to persistently deal with the illness and figure out how to take it away Prepared: join with the therapist to persistently deal with the illness and figure out how to take it away Equipped: therapist guides, doesn’t give specific solutions – parents figure out their own mutually agreeable solutions Equipped: therapist guides, doesn’t give specific solutions – parents figure out their own mutually agreeable solutions

6
Parents united against ED Parent ED

7
Who is Family-Based Treatment intended for? Efficacy of the program has been demonstrated with adolescents with anorexia under the age of 18 years old and living at home with their families. Daniel Le Grange and James Lock have recently published a new treatment manual, Treating Bulimia in Adolescents: A Family-Based Approach (2007): a family- based treatment adapted for adolescents with bulimia 19 years of age or younger, at home. Can be used with weight-restored patients who need balanced eating: Prevent weight loss/normalize eating/curtail purging
: a family- based treatment adapted for adolescents with bulimia 19 years of age or younger, at home. Can be used with weight-restored patients who need balanced eating: Prevent weight loss/normalize eating/curtail purging.")
8
Why Family-Based Treatment? Avoid separation of parents from children during a hospitalization Avoid separation of parents from children during a hospitalization Outpatient: child stays in usual surroundings Outpatient: child stays in usual surroundings Less need for hospitalization and specialty care Less need for hospitalization and specialty care Better use of easily available resources Better use of easily available resources Less costly Less costly Not worried about “Why?” Not worried about “Why?” Helps parents not blame themselves: no one to blame Helps parents not blame themselves: no one to blame Helps parents overcome helplessness Helps parents overcome helplessness

9
Where does the work take place? Mostly at home: Newer research by LeGrange, Lock and others looking at applications in IP, IOP, PHP settings including multi-family groups Mostly at home: Newer research by LeGrange, Lock and others looking at applications in IP, IOP, PHP settings including multi-family groups Whole family attends therapist-led family meetings in initial phases in outpatient setting Whole family attends therapist-led family meetings in initial phases in outpatient setting Other consultations in other outpatient or clinic settings will likely take place Other consultations in other outpatient or clinic settings will likely take place Other safe, therapeutic settings like partial hospitalization or inpatient may be needed Other safe, therapeutic settings like partial hospitalization or inpatient may be needed

10
Multi-family group applications Multi-family group applications -Dare and Eisler (2000) have adapted FBT to use as part of a multiple family day treatment program -Dare and Eisler (2000) have adapted FBT to use as part of a multiple family day treatment program - Meet with 4-6 families over several long weekends or sessions - Meet with 4-6 families over several long weekends or sessions - aim to help families share, develop skills and become motivated together, united against the eating disorder: especially helpful with unskilled, reluctant, or defeated parents (15-20% poor outcome rates w/ single families) - aim to help families share, develop skills and become motivated together, united against the eating disorder: especially helpful with unskilled, reluctant, or defeated parents (15-20% poor outcome rates w/ single families) -therapist does not have the answer as to what any individual family will need -therapist does not have the answer as to what any individual family will need -Dr. Tantillo will introduce a related MFG method -Dr. Tantillo will introduce a related MFG method

11
WHAT is FBT? FIVE BASIC PRINCIPLES 1. Agnostic 1. Agnostic 2. Parent-empowered 2. Parent-empowered 3. Focus on restoring healthy 3. Focus on restoring healthy eating eating 4. Separate illness from child 4. Separate illness from child 5. Therapist as consultant 5. Therapist as consultant

12
1. Agnostic -Agnostic with regard to causes: for example, “no ‘anorexegenic’ family” and causes are multiple and complex -Family seen as resource rather than the source of the problem: little evidence that families cause ED’s

13
2. Parent-empowerment Adolescent is out-of-control of eating disorder Adolescent is out-of-control of eating disorder Parents take charge of nutrition restoration : manage meals, disrupt extreme dieting, exercise, and purging Parents take charge of nutrition restoration : manage meals, disrupt extreme dieting, exercise, and purging In the case of bulimia, parents seek collaboration with their child to promote healthy eating and disrupt pathological eating and purging behaviors In the case of bulimia, parents seek collaboration with their child to promote healthy eating and disrupt pathological eating and purging behaviors Parents respect need for adolescent control and autonomy in areas other than weight/food Parents respect need for adolescent control and autonomy in areas other than weight/food

14
2. Parent-empowerment Parents in authority : Siblings play patient- supportive (not parent-supportive) role Parents in authority : Siblings play patient- supportive (not parent-supportive) role Parents’ supervision and involvement in adolescent’s eating and weight-related behaviors is temporary: once ED hold is released control is returned to adolescent Parents’ supervision and involvement in adolescent’s eating and weight-related behaviors is temporary: once ED hold is released control is returned to adolescent Parents return control of eating and weight-related behaviors to adolescent after eating patterns normalized and purging discontinued Parents return control of eating and weight-related behaviors to adolescent after eating patterns normalized and purging discontinued
 role Parents in authority : Siblings play patient- supportive (not parent-supportive) role Parents’ supervision and involvement in adolescent’s eating and weight-related behaviors is temporary: once ED hold is released control is returned to adolescent Parents’ supervision and involvement in adolescent’s eating and weight-related behaviors is temporary: once ED hold is released control is returned to adolescent Parents return control of eating and weight-related behaviors to adolescent after eating patterns normalized and purging discontinued Parents return control of eating and weight-related behaviors to adolescent after eating patterns normalized and purging discontinued.")
15
FBT can be demanding …it takes time and focused effort.

16
3. Focus on restoring healthy eating habits Initial task is focus on healthy eating habits and normalizing eating at home: parents manage the eating disorder Initial task is focus on healthy eating habits and normalizing eating at home: parents manage the eating disorder Family encouraged to work out for themselves how to best manage eating disorder symptoms: restore healthy eating and curtail purging Family encouraged to work out for themselves how to best manage eating disorder symptoms: restore healthy eating and curtail purging

17
4. Separate illness from child Adolescent is ill rather than obstinate: prevent criticism of patient Adolescent is ill rather than obstinate: prevent criticism of patient Illness is externalized: symptoms don’t belong to child, illness overtakes child Illness is externalized: symptoms don’t belong to child, illness overtakes child Parents sympathize with the plight the illness has created for their offspring Parents sympathize with the plight the illness has created for their offspring Therapist models sympathy and understanding Therapist models sympathy and understanding

18
5. Therapist as consultant Outpatient family therapist acts as consultant and coach Outpatient family therapist acts as consultant and coach Therapist asks, “What will it take to restore your child’s health?” Therapist asks, “What will it take to restore your child’s health?” Therapist guides, assists, encourages Therapist guides, assists, encourages parents to take an active role parents to take an active role Reminds parents of their skills Reminds parents of their skills Reinvigorates when parents discouraged Reinvigorates when parents discouraged

19
Other professionals on the team: biopsychosocial approach The family therapist leads the treatment philosophy – make regular team contacts The family therapist leads the treatment philosophy – make regular team contacts Co-therapist in family therapy, if available Co-therapist in family therapy, if available Nutritionists, physicians, psychopharmacologists act as consultants Nutritionists, physicians, psychopharmacologists act as consultants Close medical management is important: weights usually taken by therapist, objective weights occur in physician’s office Close medical management is important: weights usually taken by therapist, objective weights occur in physician’s office Everybody on the same page: team members need to be familiar with the treatment philosophy and allow it to guide their contact with the patient and family Everybody on the same page: team members need to be familiar with the treatment philosophy and allow it to guide their contact with the patient and family

20
Three phases of treatment with Maudsley approach or FBT Phase I: Establish healthy eating and curtail purge behavior (1-10 sessions or as needed) Phase I: Establish healthy eating and curtail purge behavior (1-10 sessions or as needed) Phase II: Return control of eating and weight management to the adolescent (Sessions 11-16 or as needed) Phase II: Return control of eating and weight management to the adolescent (Sessions 11-16 or as needed) Phase III: Address family and normal adolescent developmental issues (Sessions 17-20 or as needed) Phase III: Address family and normal adolescent developmental issues (Sessions 17-20 or as needed)
 Phase I: Establish healthy eating and curtail purge behavior (1-10 sessions or as needed) Phase II: Return control of eating and weight management to the adolescent (Sessions or as needed) Phase II: Return control of eating and weight management to the adolescent (Sessions or as needed) Phase III: Address family and normal adolescent developmental issues (Sessions or as needed) Phase III: Address family and normal adolescent developmental issues (Sessions or as needed)")
21
Phase I: The eating disorder rules Phase I: The eating disorder rules

22
Phase III: Adolescent has mastered the symptoms

23
Phase III Attention to other family and developmental problems deferred until later in therapy when illness no longer basis for interaction unless there is obvious interference with therapy Attention to other family and developmental problems deferred until later in therapy when illness no longer basis for interaction unless there is obvious interference with therapy Phase III already familiar to experienced therapists Phase III already familiar to experienced therapists

24
Duration of FBT Studies (Lock et al, 2005) and others studying FBT show treatment of AN lasts from 6 to 18 months with anywhere from 9 to 47 sessions. Studies (Lock et al, 2005) and others studying FBT show treatment of AN lasts from 6 to 18 months with anywhere from 9 to 47 sessions. Study by Lock, Agras, Bryson, and Kraemer (2005) shows short-term course of family therapy for AN as effective as long term, regardless of intensity and duration, except in case of non-intact family and more severe eating-related obsessive-compulsive features Study by Lock, Agras, Bryson, and Kraemer (2005) shows short-term course of family therapy for AN as effective as long term, regardless of intensity and duration, except in case of non-intact family and more severe eating-related obsessive-compulsive features Length of each phase can vary, especially with BN: be flexible, maintain integrity of protocol Length of each phase can vary, especially with BN: be flexible, maintain integrity of protocol (example: comorbidities with BN) (example: comorbidities with BN)
 and others studying FBT show treatment of AN lasts from 6 to 18 months with anywhere from 9 to 47 sessions. Study by Lock, Agras, Bryson, and Kraemer (2005) shows short-term course of family therapy for AN as effective as long term, regardless of intensity and duration, except in case of non-intact family and more severe eating-related obsessive-compulsive features Study by Lock, Agras, Bryson, and Kraemer (2005) shows short-term course of family therapy for AN as effective as long term, regardless of intensity and duration, except in case of non-intact family and more severe eating-related obsessive-compulsive features Length of each phase can vary, especially with BN: be flexible, maintain integrity of protocol Length of each phase can vary, especially with BN: be flexible, maintain integrity of protocol (example: comorbidities with BN) (example: comorbidities with BN).")
26
Traditional family treatment model: similarities Family support recruited Family support recruited Family-based guidelines commonly given to parents during nutrition restoration Family-based guidelines commonly given to parents during nutrition restoration Like Maudsley or FBT, unity/coordination of treatment professionals across disciplines required Like Maudsley or FBT, unity/coordination of treatment professionals across disciplines required

27
Key differences between traditional family and FBT approaches Traditional approaches: A combination of individual and family sessions are included from the beginning. A combination of individual and family sessions are included from the beginning. Strong emphasis placed on developing assertiveness, autonomy, and self-control in adolescents from early stage. Strong emphasis placed on developing assertiveness, autonomy, and self-control in adolescents from early stage. May involve child meal planning May involve child meal planning

28
Traditional approaches: Buy and keep around the house a wide variety of nutritionally balanced foods for child to chose from Buy and keep around the house a wide variety of nutritionally balanced foods for child to chose from Family meals: encourage parents not to comment on child’s eating behavior at meals: neutral discussion topics Family meals: encourage parents not to comment on child’s eating behavior at meals: neutral discussion topics If patient does not want meal prepared by parent, child prepares an alternative meal to be eaten at family meal If patient does not want meal prepared by parent, child prepares an alternative meal to be eaten at family meal

29
Traditional approaches: Parents avoid responding to requests from child for reassurance about food choices Parents avoid responding to requests from child for reassurance about food choices Binge/purging patients need to clean up any messes and replace binge foods Binge/purging patients need to clean up any messes and replace binge foods Parents do not disrupt dieting, exercise, or purging: child typically reports symptoms to team Parents do not disrupt dieting, exercise, or purging: child typically reports symptoms to team

31
Harnessing parents’ anxiety with FBT Families are highly anxious when they present for treatment Families are highly anxious when they present for treatment Families are often preoccupied with food, weight, and purging and eating behavior Families are often preoccupied with food, weight, and purging and eating behavior Families are often feeling helpless and despairing Families are often feeling helpless and despairing

32
Families are often frozen with fear because of the life-threatening nature of the illness: rigid about change Families are often frozen with fear because of the life-threatening nature of the illness: rigid about change Families may be avoiding any stress or conflict that they think will aggravate their child’s symptoms Families may be avoiding any stress or conflict that they think will aggravate their child’s symptoms If conflict does ensue or there is failure at pre-treatment attempts to restore healthy eating, guilt and blame result If conflict does ensue or there is failure at pre-treatment attempts to restore healthy eating, guilt and blame result

33
Therapist harnesses the anxiety Therapist validates, joins, and enhances anxiety in early phase of treatment: use anxiety as motivational tool Therapist validates, joins, and enhances anxiety in early phase of treatment: use anxiety as motivational tool Families are relieved from their helplessness: therapist gives direction, control and clear responsibility to parents under watchful eye of therapist. Families are relieved from their helplessness: therapist gives direction, control and clear responsibility to parents under watchful eye of therapist. Get family organized, consistent, persistent Get family organized, consistent, persistent

34
Families are relieved to have therapist join their primary focus on managing and eliminating eating disorder Families are relieved to have therapist join their primary focus on managing and eliminating eating disorder Enhance therapeutic alliance by searching for and identifying family strengths that may surface in the midst of family helplessness and anxiety, Enhance therapeutic alliance by searching for and identifying family strengths that may surface in the midst of family helplessness and anxiety, e.g., find positives in enmeshment, “This is close knit family with lots of caring and support.” e.g., find positives in enmeshment, “This is close knit family with lots of caring and support.”

35
What family characteristics need to be facilitated with FBT? Parental unity: parental agreement needs to be present Parental unity: parental agreement needs to be present Willingness to take control or supervise: starvation, pathological eating, purging not an option, parents may be reluctant Willingness to take control or supervise: starvation, pathological eating, purging not an option, parents may be reluctant Patience and empathy: parents try to understand the patient’s internal landscape Patience and empathy: parents try to understand the patient’s internal landscape Organized, persistent and consistent: available daily, routinely Organized, persistent and consistent: available daily, routinely Willingness to see the therapist as collaborator: de-mystify therapy as having all the answers Willingness to see the therapist as collaborator: de-mystify therapy as having all the answers

36
Non-blaming of child for eating disorder: parental criticism found to be associated with poor outcomes (LeGrange et al, 1992): Separated family therapy may be necessary Non-blaming of child for eating disorder: parental criticism found to be associated with poor outcomes (LeGrange et al, 1992): Separated family therapy may be necessary Willingness to let go of parental self- blame Willingness to let go of parental self- blame Tolerance of child’s anger and resistance to change Tolerance of child’s anger and resistance to change Knowledgeable of ED’s and Tx goals Knowledgeable of ED’s and Tx goals Flexible, e.g., let go of “why?”, put recovery first, be experimental Flexible, e.g., let go of “why?”, put recovery first, be experimental
: Separated family therapy may be necessary Non-blaming of child for eating disorder: parental criticism found to be associated with poor outcomes (LeGrange et al, 1992): Separated family therapy may be necessary Willingness to let go of parental self- blame Willingness to let go of parental self- blame Tolerance of child’s anger and resistance to change Tolerance of child’s anger and resistance to change Knowledgeable of ED’s and Tx goals Knowledgeable of ED’s and Tx goals Flexible, e.g., let go of why , put recovery first, be experimental Flexible, e.g., let go of why , put recovery first, be experimental")
37
When not to use FBT Excessive marital discord, parental disunity Excessive marital discord, parental disunity Parent(s) too disabled Parent(s) too disabled Lack of understanding child’s eating disorder Lack of understanding child’s eating disorder Excessive, chronic parental self-blame: often results in excessive parental frustration, anger, defensiveness, lack of therapeutic alliance Excessive, chronic parental self-blame: often results in excessive parental frustration, anger, defensiveness, lack of therapeutic alliance Child too ill with other mental health or medical problems Child too ill with other mental health or medical problems Too few resources or opportunities Too few resources or opportunities Unable to attend initial sessions at least 3x per month Unable to attend initial sessions at least 3x per month
 too disabled Parent(s) too disabled Lack of understanding child’s eating disorder Lack of understanding child’s eating disorder Excessive, chronic parental self-blame: often results in excessive parental frustration, anger, defensiveness, lack of therapeutic alliance Excessive, chronic parental self-blame: often results in excessive parental frustration, anger, defensiveness, lack of therapeutic alliance Child too ill with other mental health or medical problems Child too ill with other mental health or medical problems Too few resources or opportunities Too few resources or opportunities Unable to attend initial sessions at least 3x per month Unable to attend initial sessions at least 3x per month")
39
Important differences in AN and BN (LeGrange and Lock, 2007) More adolescents with BN – 2-5% of adolescent girls with BN (Walsh and Wilson, 1997). Some have progressed from AN. More adolescents with BN – 2-5% of adolescent girls with BN (Walsh and Wilson, 1997). Some have progressed from AN. Broader specturm of co-morbid illnesses with BN, e.g., self-harm behaviors common: can derail the therapy Broader specturm of co-morbid illnesses with BN, e.g., self-harm behaviors common: can derail the therapy AN often arouses more fear making it easier to stay focused on ED symptoms AN often arouses more fear making it easier to stay focused on ED symptoms BN more secretive, less obvious: patient may appear well, detracting from parental motivation BN more secretive, less obvious: patient may appear well, detracting from parental motivation
. Some have progressed from AN. Broader specturm of co-morbid illnesses with BN, e.g., self-harm behaviors common: can derail the therapy Broader specturm of co-morbid illnesses with BN, e.g., self-harm behaviors common: can derail the therapy AN often arouses more fear making it easier to stay focused on ED symptoms AN often arouses more fear making it easier to stay focused on ED symptoms BN more secretive, less obvious: patient may appear well, detracting from parental motivation BN more secretive, less obvious: patient may appear well, detracting from parental motivation.")
40
Important differences in AN and BN BN usually ego-dystonic: more shame, embarrassment, & motivation to get rid of binge/purge symptoms – child unable to stop or interrupt symptoms BN usually ego-dystonic: more shame, embarrassment, & motivation to get rid of binge/purge symptoms – child unable to stop or interrupt symptoms BN adolescents often appear more independent: have more active life experiences - parents de-motivated to interfere with adolescent freedoms and emerging independence by supervising eating and purging behaviors BN adolescents often appear more independent: have more active life experiences - parents de-motivated to interfere with adolescent freedoms and emerging independence by supervising eating and purging behaviors BN often more connected to peer group, reactive to others: higher peer exposure and motivation to yield and conform to ideal to be thin or perfect (AN more self-willed) BN often more connected to peer group, reactive to others: higher peer exposure and motivation to yield and conform to ideal to be thin or perfect (AN more self-willed)
 BN often more connected to peer group, reactive to others: higher peer exposure and motivation to yield and conform to ideal to be thin or perfect (AN more self-willed)")
41
FBT in phase I 1. Take weights with patient individually, then join family in session 2. Harness anxiety to motivate family 3. Take a history from each family member about the impact of ED 4. Give parents permission to involve themselves actively with adolescent’ s eating

42
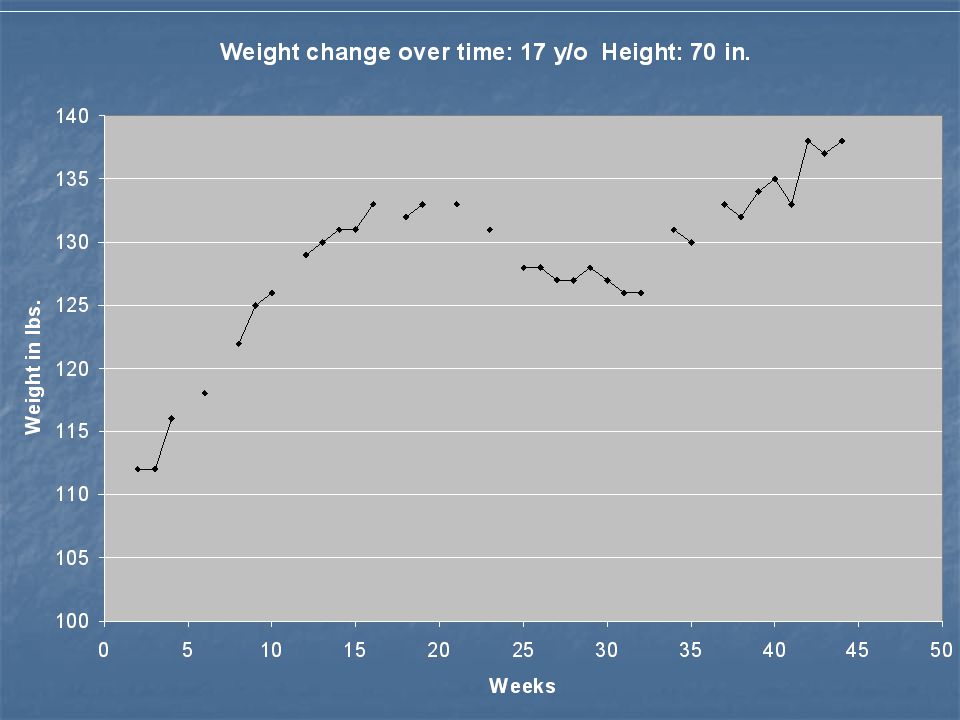
Weight chart Weight In Lbs. or kg. Date of session 1 2 3 4 5 6 7 8 9 10 11 12 100 105 110 115

43
Phase I: Family picnic 5. Family picnic: forbidden foods + healthy amounts of food Role play Role play

44
Phase I 6. Re-emphasize goal is to normalize eating and eliminate binge eating and purging. 7. Congratulate any progress, sympathize with lack of progress, reinforce vigilant stance against ED

45
Phase I 8. Regularize, organize family meals: parents supervise eating 9. Sibling support defined 10. Therapist helps parents eliminate criticism and judgment as well as avoid arguments with patient: will improve patient’s honesty, reduce shame and guilt common with BN

46
Differences between AN & BN treatment interventions in Phase I Take more firm control with AN: With AN review weight charts each session. Look for progress in the form of an upward trajectory as sessions progress With BN, keep binge and purge charts, take weights with patient individually, then join family in session. Report B/P progress to family, not weight with BN, unless extreme weight loss

47
Patient binge/purge log (LeGrange and Lock, 2007, p. 29 ) DayBingePurge 1 2 3 4 5 6 7
 DayBingePurge")
48
Therapist binge/purge charts (LeGrange and Lock, 2007, p. 30-31 ) 8 7 6 5 4 3 2 12345678910 Date of session or session number # O F P U R G E S Or B I N G E S
 Date of session or session number # O F P U R G E S Or B I N G E S.")
49
Show respect for the adolescent’s point of view and experience: adolescents with AN more regressed than adolescents with BN - help shape eating behavior of adolescent with BN while carefully keeping some distance from adolescent’s other life activities: Say to parents: “Your role is to help your child get better with your daughter’s (or son’s) help.” Say to parents: “Your role is to help your child get better with your daughter’s (or son’s) help.”
 help. Say to parents: Your role is to help your child get better with your daughter’s (or son’s) help.")
50
With BN parents negotiate with adolescent to help disrupt binge eating and purge episodes : examples: examples: (1) negotiate planned distractions (1) negotiate planned distractions (2) adolescent fills out B/P chart with parent (2) adolescent fills out B/P chart with parent reminders reminders (3) parents and child agree to work on one (3) parents and child agree to work on one problem at a time problem at a time
 negotiate planned distractions (1) negotiate planned distractions (2) adolescent fills out B/P chart with parent (2) adolescent fills out B/P chart with parent reminders reminders (3) parents and child agree to work on one (3) parents and child agree to work on one problem at a time problem at a time")
51
Dealing with parental hostility The Effective Meal Support for Family and Friends video: British Columbia Children’s Hospital The Effective Meal Support for Family and Friends video: British Columbia Children’s Hospital

52
How to deal with parents’ hostility Model non-critical acceptance of patient and symptoms Model non-critical acceptance of patient and symptoms Help parents blame the illness, not the child Help parents blame the illness, not the child Carefully identify ways instance of criticism/hostility got in the way of progress – look at pain underneath hostility, e.g., parents overburdened, exhausted, frustrated Carefully identify ways instance of criticism/hostility got in the way of progress – look at pain underneath hostility, e.g., parents overburdened, exhausted, frustrated Find alternative ways to handle hostile interaction: Find alternative ways to handle hostile interaction: “The eating disorder (rather than child) is a very selfish “The eating disorder (rather than child) is a very selfish illness right now – it is trying to stop you from eating.” illness right now – it is trying to stop you from eating.” Call on less critical parent/caretaker to support and assist in decreasing critical comments, finding alternatives Call on less critical parent/caretaker to support and assist in decreasing critical comments, finding alternatives
 is a very selfish The eating disorder (rather than child) is a very selfish illness right now – it is trying to stop you from eating. illness right now – it is trying to stop you from eating. Call on less critical parent/caretaker to support and assist in decreasing critical comments, finding alternatives Call on less critical parent/caretaker to support and assist in decreasing critical comments, finding alternatives")
53
Returning autonomy to adolescent: phase II In Phase II, use treatment to begin introducing return to normal adolescent development: foster autonomy In Phase II, use treatment to begin introducing return to normal adolescent development: foster autonomy Parents’ anxiety reduced and confidence in managing illness is high Parents’ anxiety reduced and confidence in managing illness is high In case of AN, patient has surrendered to the parents’ demands in Phase I In case of AN, patient has surrendered to the parents’ demands in Phase I In case of BN, begin to return control of eating and related purge behaviors to adolescent under parental supervision. In case of BN, begin to return control of eating and related purge behaviors to adolescent under parental supervision.

54
Phase II: When? Patient able to eat without cajoling by parents The hold of the AN or BN over excessive weight preoccupation, diet strategies, and binge and purge behaviors broken by collaborative efforts in Phase 1: Binge/purges less than 1-2 times per month. The hold of the AN or BN over excessive weight preoccupation, diet strategies, and binge and purge behaviors broken by collaborative efforts in Phase 1: Binge/purges less than 1-2 times per month. Family ready for increased independence from therapist Family ready for increased independence from therapist Healthy weight is restored/weight stable Healthy weight is restored/weight stable

55
Phase II Use of diet supplement drinks or bars discouraged heading into phase II Use of diet supplement drinks or bars discouraged heading into phase II Sessions more spread apart: every 2-3 weeks OK Sessions more spread apart: every 2-3 weeks OK Examine relationship between adolescent issues and development of ED Examine relationship between adolescent issues and development of ED Therapist introduces previously set aside non-eating-disorder-related issues Therapist introduces previously set aside non-eating-disorder-related issues Continue to monitor and modify criticism of adolescent by parents or sibling Continue to monitor and modify criticism of adolescent by parents or sibling

56
Weights and binge/purge behaviors continue to be monitored until Phase III Weights and binge/purge behaviors continue to be monitored until Phase III Continued reinforcing of the difference between illness-driven thinking and healthy thinking Continued reinforcing of the difference between illness-driven thinking and healthy thinking Monitor parents’ increased temptation to criticize patient as she or he takes over: support best efforts of patient. Monitor parents’ increased temptation to criticize patient as she or he takes over: support best efforts of patient. Healthy eating habits and absence of purging behavior remain the focus of treatment even as parent supervision is phased out Healthy eating habits and absence of purging behavior remain the focus of treatment even as parent supervision is phased out

57
Ways to decrease parental supervision 1. Adolescent gradually makes more food choices as long as choices are healthy and in adequate volume: e.g., allow some healthy substitutions 2. Reduce supervision of snacks 2. Reduce supervision of snacks 3. Reduce supervision of one meal at a time 3. Reduce supervision of one meal at a time 4. Increase food shopping responsibility and 4. Increase food shopping responsibility and meal preparation meal preparation

58
Decreasing parental involvement 5. Eat alone sometimes versus with family 6. Adolescent able to report urges to purge/restrict/binge to parents and ask for support, when needed 7. Adolescent dishes out own portions under watchful eye of parents

59
Role play Phase II Phase II

60
Pitfalls of negotiating Phase II Patient sees the lull coming out of Phase I as a long-awaited opportunity to resume unhealthy eating and purge behavior and therapist/parents fail to renew supervision Patient sees the lull coming out of Phase I as a long-awaited opportunity to resume unhealthy eating and purge behavior and therapist/parents fail to renew supervision With AN, family and/or therapist mistake a suboptimal plateau in weight as adequate for moving to Phase II: encourage appropriate anxiety about relapse With AN, family and/or therapist mistake a suboptimal plateau in weight as adequate for moving to Phase II: encourage appropriate anxiety about relapse Therapist influenced by other team members Therapist influenced by other team members

61
Other pitfalls Parents/therapist too exhausted to move on and wish to stop treatment once health restored: make sure adolescent well on the way to normal adolescence before moving on, e.g., adolescent realigned with peers while parents refocused on normal adult lives Parents/therapist too exhausted to move on and wish to stop treatment once health restored: make sure adolescent well on the way to normal adolescence before moving on, e.g., adolescent realigned with peers while parents refocused on normal adult lives Failure to see connections between adolescent issues and development of ED: must understand ways in which ED is a form of communication, currency in family Failure to see connections between adolescent issues and development of ED: must understand ways in which ED is a form of communication, currency in family Therapist takes too much responsibility for family problem solving: therapist must advocate family arriving at their own solutions, assist the family process Therapist takes too much responsibility for family problem solving: therapist must advocate family arriving at their own solutions, assist the family process Parents too traumatized/anxious to let go of control: become critical Parents too traumatized/anxious to let go of control: become critical An artificial deadline for “getting finished” looms: e.g., college An artificial deadline for “getting finished” looms: e.g., college

63
What parents have to say Helpful: Laura Collins, “Olympia’s mind came back incrementally. It was one bite at a time.” (p. 142) Helpful: Laura Collins, “Olympia’s mind came back incrementally. It was one bite at a time.” (p. 142) Anxiety-provoking to have so much responsibility Anxiety-provoking to have so much responsibility In beginning difficult to let go of pursuing “why” ED occurred. In beginning difficult to let go of pursuing “why” ED occurred. Parents say they second-guess themselves about letting go of supervision, e.g., give adolescent a choice then act disappointed Parents say they second-guess themselves about letting go of supervision, e.g., give adolescent a choice then act disappointed Parents sometimes say they didn’t know what their child was eating before FBT: chaotic meal times Parents sometimes say they didn’t know what their child was eating before FBT: chaotic meal times Parents find occasional nutrition consultation important Parents find occasional nutrition consultation important Parents usually need consultation about restricting exercise : how much? how often? Parents usually need consultation about restricting exercise : how much? how often?
 Helpful: Laura Collins, Olympia’s mind came back incrementally. It was one bite at a time. (p. 142) Anxiety-provoking to have so much responsibility Anxiety-provoking to have so much responsibility In beginning difficult to let go of pursuing why ED occurred. In beginning difficult to let go of pursuing why ED occurred. Parents say they second-guess themselves about letting go of supervision, e.g., give adolescent a choice then act disappointed Parents say they second-guess themselves about letting go of supervision, e.g., give adolescent a choice then act disappointed Parents sometimes say they didn’t know what their child was eating before FBT: chaotic meal times Parents sometimes say they didn’t know what their child was eating before FBT: chaotic meal times Parents find occasional nutrition consultation important Parents find occasional nutrition consultation important Parents usually need consultation about restricting exercise : how much. how often. Parents usually need consultation about restricting exercise : how much. how often .")
64
What patients have to say Two studies (Krautter and Lock, 2004 and le Grange and Gelman, 1998) have found both patients and parents find FBT helpful and successful, although many adolescents reported a need for more individual therapy. Two studies (Krautter and Lock, 2004 and le Grange and Gelman, 1998) have found both patients and parents find FBT helpful and successful, although many adolescents reported a need for more individual therapy. Observations of patients: Observations of patients: - Adolescents appreciate seeing their parents relieved from their anxiety. Many tend to worry about their parents’ distress. - Adolescents appreciate seeing their parents relieved from their anxiety. Many tend to worry about their parents’ distress. - If given a choice between a more traditional model and FBT, many choose FBT because they felt out-of control of ED - If given a choice between a more traditional model and FBT, many choose FBT because they felt out-of control of ED
 have found both patients and parents find FBT helpful and successful, although many adolescents reported a need for more individual therapy. Observations of patients: Observations of patients: - Adolescents appreciate seeing their parents relieved from their anxiety. Many tend to worry about their parents’ distress. - Adolescents appreciate seeing their parents relieved from their anxiety. Many tend to worry about their parents’ distress. - If given a choice between a more traditional model and FBT, many choose FBT because they felt out-of control of ED - If given a choice between a more traditional model and FBT, many choose FBT because they felt out-of control of ED.")
65
Adolescents’ reactions to FBT Adolescents generally form a good therapeutic alliance even though therapist supporting their parents’ supervising their eating and weight management behavior: they know you know and know they need help they know you know and know they need help

66
“Yelling at my mother about food was the first time I ever yelled at her since I was little.” “I hate this even though I understand why my parents had to do it.” “I can tell my father when I feel like purging and he helps me think about it and not vomit.” “I have learned the best way to eat things I am afraid of is just do it.” “Later on when I went to college I had trouble eating enough consistently but I never lost my ability to eat all kinds of foods I learned to eat with my parents. That did not change.” “I might as well gain weight because my parents won’t give up.”

67
“Don’t give up too soon, as the family is the best resource for recovery.” “Don’t give up too soon, as the family is the best resource for recovery.” (Lock et al. 2001. Treatment Manual for Anorexia Nervosa: A Family-based Approach. NY: The Guilford Press. p. 21.) (Lock et al. 2001. Treatment Manual for Anorexia Nervosa: A Family-based Approach. NY: The Guilford Press. p. 21.)
 (Lock et al Treatment Manual for Anorexia Nervosa: A Family-based Approach. NY: The Guilford Press. p. 21.).")
68
REFERENCES British Columbia Children’s Hospital (2002) Effective Meal Support for Family and Friends (DVD-R and VHS film) Collins, Laura (2005) Eating with Your Anorexic. NY: McGraw Hill. Eisler, I The empirical and theoretical base of family therapy and multiple family day therapy for adolescent anorexia. Journal of Family Therapy, 2005; 27:2, 104-131. Eisler, I., Dare, C., Hodes, M., Russell, G.F. M., Dodge, E. and LeGrange, D. “Family therapy for adolescent anorexia nervosa: The results of a controlled comparison of two family interventions.” Journal of Child Psychology and Psychiatry. 2000; 41, 727-736. Haltom, C. (2004) A Stranger at the Table: Dealing with Your Child’s Eating Disorder. Denton, TX: Ronjon Pub. (in Gurze on-line catalog)
 A Stranger at the Table: Dealing with Your Child’s Eating Disorder. Denton, TX: Ronjon Pub. (in Gurze on-line catalog).")
69
Krautter, T. and Lock, James. Is manualized family-based treatment for adolescent anorexia nervosa acceptable to patients? Patient satisfaction at the end of treatment. Journal of Family Therapy. 2004; 26: 65-81. Le Grange, D., Eisler, I, Dare, C., and Hodes, M. Family criticism and self-starvation: A study of expressed emotion. Journal of Family Therapy. 1992; 14: 177-192. Le Grange, D., Eisler, I., Dare, C., Russell, G. Evaluation of family treatments in adolescent anorexia nervosa: A pilot study. International Journal of Eating Disorders. 1992; 12:4: 347-357. Le Grange, D., Gelman, T. The patient’s perspective of treatment in eating disorders: A preliminary study. South African Journal of Psychology. 1998; 28: 182-186. 28: 182-186. Le Grange, D. and Lock, J. The dearth of psychological treatment studies for anorexia nervosa, International Journal of Eating Disorders 2005; 37,79-81

70
Le Grange, D. and Lock, J. Treating Bulimia in Adolescents: A Family-Based Approach (2007) NY: Guilford Press. A Family-Based Approach (2007) NY: Guilford Press. Le Grange, D., Lock, J., and Dymek, M. Family-based therapy for adolescents with bulimia nervosa. American Journal of Psychotherapy. 2003; 67, 237. Le Grange, D., Loeb, K., Van Orman, S., Jellar, C. Bulimia nervosa in adolescents: A disorder of evolution? Archives of Pediatrics & Adolescent Medicine. 2004; 158:5, 478- 482. LeGrange, D. and Schmidt, U. (2005) The treatment of adolescents with bulimia nervosa. Journal of Mental Health. 14:6, 587-597. Lock, J. (2006) The role of family therapy for adolescents with anorexia nervosa. Psychiatric Times. Sept 1, 2006. CMP Media LLC. Lock, J., Agras, W.S., Bryson, S., Kraemer, H. A comparison of short-and long-term family therapy for adolescent anorexia nervosa. Journal of the Academy of Child & Adolescent Psychiatry. 2005; 44:7, 632-639.
 NY: Guilford Press. A Family-Based Approach (2007) NY: Guilford Press. Le Grange, D., Lock, J., and Dymek, M. Family-based therapy for adolescents with bulimia nervosa. American Journal of Psychotherapy. 2003; 67, 237. Le Grange, D., Loeb, K., Van Orman, S., Jellar, C. Bulimia nervosa in adolescents: A disorder of evolution. Archives of Pediatrics & Adolescent Medicine. 2004; 158:5, LeGrange, D. and Schmidt, U. (2005) The treatment of adolescents with bulimia nervosa. Journal of Mental Health. 14:6, Lock, J. (2006) The role of family therapy for adolescents with anorexia nervosa. Psychiatric Times. Sept 1, CMP Media LLC. Lock, J., Agras, W.S., Bryson, S., Kraemer, H. A comparison of short-and long-term family therapy for adolescent anorexia nervosa. Journal of the Academy of Child & Adolescent Psychiatry. 2005; 44:7,")
71
Lock, J., Courtier, J., Bryson, S., Agras, S. (2006) Predictors of dropout and remission in family therapy for adolescent anorexia nervosa in a randomized clinical trial. International Journal of Eating Disorders. 39:8, 639-647. 39:8, 639-647. Lock, J. and Gowers, S. (2005) Effective interventions for adolescents with anorexia nervosa. Journal of Mental Health. 14:6, 599-610. Lock, James and Le Grange, Daniel. (2005) Help Your Teenager Beat an Eating Disorder. NY: Guilford Press. Lock et al. (2001) Treatment Manual for Anorexia Nervosa: A Family-based Approach. NY: Guilford Press. Lock, J. LeGrange, D., Forsberg, S., and Hewell, K. (2006) Is family therapy useful for treating children with anorexia nervosa? Results of a case series. Journal of the American Academy of Child and Adolescent Psychiatry. 45:11, 1323-1328. Is family therapy useful for treating children with anorexia nervosa? Results of a case series. Journal of the American Academy of Child and Adolescent Psychiatry. 45:11, 1323-1328.
 Predictors of dropout and remission in family therapy for adolescent anorexia nervosa in a randomized clinical trial. International Journal of Eating Disorders. 39:8, :8, Lock, J. and Gowers, S. (2005) Effective interventions for adolescents with anorexia nervosa. Journal of Mental Health. 14:6, Lock, James and Le Grange, Daniel. (2005) Help Your Teenager Beat an Eating Disorder. NY: Guilford Press. Lock et al. (2001) Treatment Manual for Anorexia Nervosa: A Family-based Approach. NY: Guilford Press. Lock, J. LeGrange, D., Forsberg, S., and Hewell, K. (2006) Is family therapy useful for treating children with anorexia nervosa. Results of a case series. Journal of the American Academy of Child and Adolescent Psychiatry. 45:11, Is family therapy useful for treating children with anorexia nervosa. Results of a case series. Journal of the American Academy of Child and Adolescent Psychiatry. 45:11,")
72
Minuchin, S. et al (1978) Psyhosomatic Families: Anorexia Nervosa In Context. Cambridge, MA: Harvard University Press. Siegel, M., Brisman, J. and Weinshel, M. (1997) Surviving an Eating Disorder: Strategies for Families and Friends. New York: Harper Collins Publishers. Tantillo, M. “Staying afloat in a sea of disconnections: using a multifamily therapy group to engage patients, families and providers in the treatment of eating disorders,” Presentation at Renfrew Center Foundation Conference. Philadelphia, Pa. Nov. 11, 2006. Treasure, J. Whitaker, W., Whitney, J., and Schmidt, U. Working with families of adults with anorexia. Journal of Family Therapy. 2005; 27:2, 158-170.
 Surviving an Eating Disorder: Strategies for Families and Friends. New York: Harper Collins Publishers. Tantillo, M. Staying afloat in a sea of disconnections: using a multifamily therapy group to engage patients, families and providers in the treatment of eating disorders, Presentation at Renfrew Center Foundation Conference. Philadelphia, Pa. Nov. 11, Treasure, J. Whitaker, W., Whitney, J., and Schmidt, U. Working with families of adults with anorexia. Journal of Family Therapy. 2005; 27:2,")
Similar presentations






 Drive for Thinness, intense fear of gaining weight >= 15% below expected weight Body image distortion (feel fat) Preoccupation with.>")















