Download presentation
Presentation is loading. Please wait.

1
Pediatric Obstructive Sleep Apnea Syndrome: Kids are not simply little adults Ronald J. Green, MD, FCCP Diplomate, American Board of Sleep Medicine Sleep Disorders & Pulmonary Disease, The Everett Clinic Medical Director North Puget Sound Center for Sleep Disorders Everett, WA 425-339-5410; www.ilikesleep.com

2
Obstructive Sleep Apnea Syndrome Obstructive Sleep Apnea Syndrome Common Dangerous Easily recognized Treatable

3
Apnea Patterns Obstructive Mixed MixedCentral Airflow Airflow Respiratoryeffort

4
Measures of Sleep Apnea Frequency Apnea Index –# apneas per hour of sleep Apnea / Hypopnea Index (AHI) –# apneas + hypopneas per hour of sleep
 –# apneas + hypopneas per hour of sleep")
5
Pediatric OSAS Epidemiology 7% to 20% of children snore frequently 1% to 3% of preschool age children have OSAS Peak age is two to five years

6
Pathophysiology of Obstructive Apnea

7
Pathophysiology of OSAS Awake: Small airway + neuromuscular compensation Loss of neuromuscular compensation Sleep Onset Hyperventilate: correct hypoxia & hypercapnia Decreased pharyngeal muscle activity Airway opens Airway collapses Pharyngeal muscle activity restored Apnea Arousal from sleep Hypoxia & Hypercapnia Increased ventilatory effort +

8
Adult OSAS Risk Factors Obesity Increasing age Male gender Anatomic abnormalities of upper airway Family history Alcohol or sedative use Smoking

9
Adult OSAS Risk Factors, cont’d Hypothyriodism Acromegaly Amyloidosis Vocal cord paralysis Marfan syndrome Down syndrome Neuromuscular disorders

10
Pediatric OSAS Risk Factors Adenotonsillar hypertrophy Craniofacial anomalies Down Syndrome Obesity Neurological disorders Family History

11
Adapted from Redline S et al. Am J Resp Crit Care Med 1995;151. Likelihood of Sleep Apnea as Function of Family Prevalence Risk Factor: Family History (Adjusted for age, race, sex, BMI) Odds Ratio 1 2 3 1 2 3 Relative Relatives Relatives Relative Relatives Relatives
 Odds Ratio Relative Relatives Relatives Relative Relatives Relatives.")
12
Adults: Clinical Consequences Obstructive Sleep Apnea Syndrome Excessive daytime sleepiness Sleep fragmentation, Hypoxia / Hypercapnia Cardiovascular Complications MorbidityMortality

13
Adult OSAS consequences Excessive daytime sleepiness Increased motor vehicle crashes & work-related accidents Poor job performance Poor memory and concentrating ability Family discord from loud snoring and above symptoms Chronic headaches Hypertension Increased incidence of depression Decreased quality of life

14
Pediatrics: Clinical Consequences Obstructive Sleep Apnea Syndrome Attention and hyperactivity problems Sleep fragmentation, Hypoxia / Hypercapnia In very severe cases, cor pulmonale and hypertension MorbidityMortality

15
Pediatric OSAS consequences Behavioral problems at home and at school Hyperactivity and inattention (ADHD symptoms) Discipline problems at school Poor school performance Irritability Difficulties with memory and concentrating ability Morning headaches Failure to thrive Decreased quality of life Uncommon symptom in pediatrics: Excessive daytime sleepiness
 Discipline problems at school Poor school performance Irritability Difficulties with memory and concentrating ability Morning headaches Failure to thrive Decreased quality of life Uncommon symptom in pediatrics: Excessive daytime sleepiness")
16
Adult OSAS Diagnosis: History Loud snoring (not all snore) Nocturnal gasping and choking –Ask bed partner (witnessed apneas) Automobile or work related accidents Personality changes or cognitive problems Risk factors Excessive daytime sleepiness (often not recognized by patient) Frequent nocturia Sleep Apnea: Is Your Patient at Risk? NIH Publication, No 95-3803.

17
Pediatric OSAS Diagnosis: History Loud snoring (almost all snore loudly) Snorting/gasping/choking Observed apneic pauses (often not seen) Restless sleep Diaphoresis Abnormal sleeping position Paradoxical chest wall movement Secondary enuresis
 Snorting/gasping/choking Observed apneic pauses (often not seen) Restless sleep Diaphoresis Abnormal sleeping position Paradoxical chest wall movement Secondary enuresis")
18
Pediatric OSAS Diagnosis: History, cont’d Attention deficit and hyperactivity symptoms Behavioral problems Poor school performance Difficulty awakening in AM Morning headaches Uncommon symptom in pediatrics: daytime somnolence Symptoms from adenotonsillar hypertrophy

19
Adult diagnosis: Physical Examination Obvious airway abnormality Upper body obesity / thick neck > 17” males > 16” females Hypertension

20
Adult Physical Exam: Oropharynx

21
Adult Physical Examination Guilleminault C et al. Sleep Apnea Syndromes. New York: Alan R. Liss, 1978.

22
Pediatric diagnosis: Physical Examination Tonsillar hypertrophy Nasal obstruction Overbite Morbid obesity Behavior in exam room Note: PE often is normal

23
Exam: Tonsillar Hypertrophy Shepard JW Jr et al. Mayo Clin Proc 1990;65.

24
Why Get a Sleep Study? Signs and symptoms poorly predict disease severity Appropriate therapy dependent on severity Failure to treat leads to: –Increased morbidity and mortality –Motor vehicle crashes and job-related accidents in adults Other sleep disorders can cause same symptoms (especially restless legs syndrome in both pediatrics and adults)
.")
25
Diagnosis of Sleep Apnea In-laboratory polysomnography –Gold standard –Assess severity –Initiate treatment –Look for other sleep disorders

26
Polysomnography

27
Nocturnal Polysomnogram

28
Nocturnal Polysomnography In contrast to adults, children have: Fewer obstructive apneas Desaturation with shorter events Higher respiratory rate Lower functional residual capacity Smaller oxygen stores

29
Pediatric OSAS treatment Surgery –Adenotonsillectomy (treatment of choice) –Turbinate reduction if indicated –Maxillofacial surgery –Tracheostomy (very rarely) Weight loss if obese Nasal Continuous Positive Airway Pressure (CPAP)----Will discuss in more detail under adult treatment options
 –Turbinate reduction if indicated –Maxillofacial surgery –Tracheostomy (very rarely) Weight loss if obese Nasal Continuous Positive Airway Pressure (CPAP)----Will discuss in more detail under adult treatment options")
30
Pediatric OSAS treatment: Adenotonsillectomy Usually highly effective in children with adenotonsillar hypertrophy, even in the presence of other underlying conditions Children with severe pre-operative OSAS should have post-op PSG to confirm complete remission of OSA

31
Pediatric groups at high risk for postoperative T&A complications Age less than two Severe OSAS by nocturnal polysomnography Associated medical conditions –Craniofacial anomalies –Hypotonia –Severe obesity Complications of OSAS already present –Failure to thrive –Cor pulmonale

32
Postoperative monitoring of high risk pediatric patients Postoperatively, high risk patients should be observed overnight in a facility where appropriate monitoring and care are available.

33
Adult OSAS treatment: Adenotonsillectomy Adenotonsillectomy by itself does not work in adults

34
Adult OSAS treatment Risk counseling –Motor vehicle crashes –Job-related hazards –Judgment impairment Apnea and comorbidity treatment –Behavioral –Medical (non-surgical) –Surgical
 –Surgical")
35
The High-Risk Driver Educate patient Document warning Resolve apnea quickly Follow-up –Effectiveness –Compliance

36
Adults: Behavioral Interventions Encourage patients to: –Lose weight –Avoid alcohol and sedatives –Avoid sleep deprivation –Avoid supine sleep position –Stop smoking

37
Adults and kids: Weight loss Should be prescribed for all obese patients Can be curative but has low success rate Other treatment is required until optimal weight loss is achieved

38
Medical Interventions Positive airway pressure –Continuous positive airway pressure (CPAP) –Bi-level positive airway pressure Oral appliances Other (limited role) –Medications---don’t work –Oxygen
 –Bi-level positive airway pressure Oral appliances Other (limited role) –Medications---don’t work –Oxygen")
39
Positive Airway Pressure

42
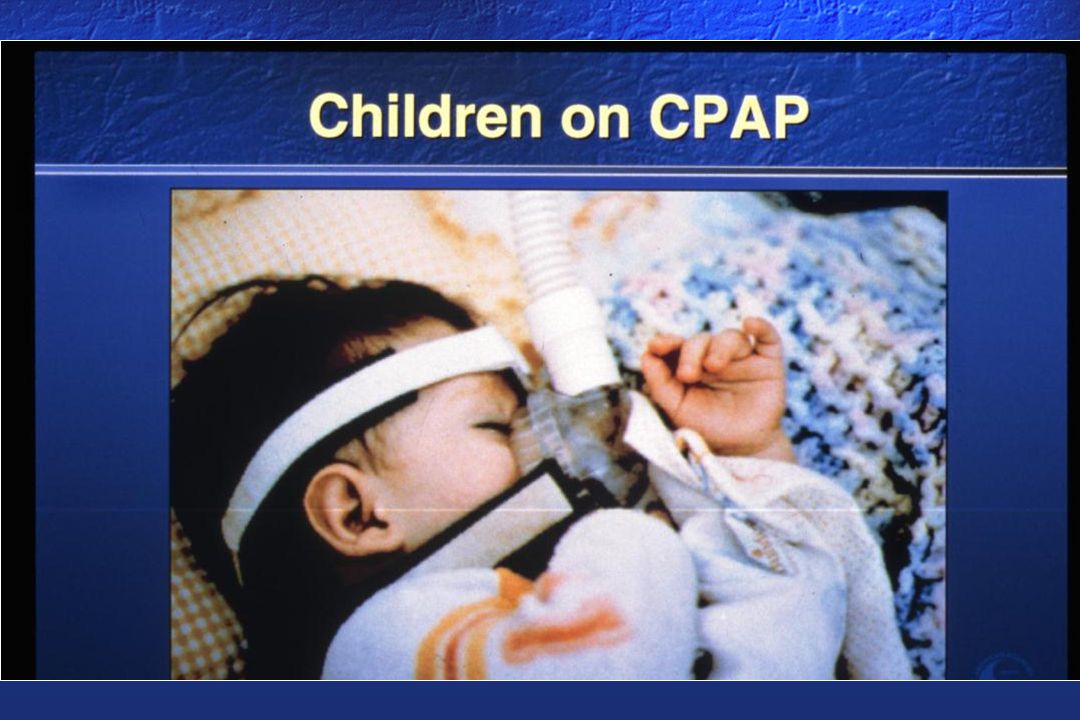
Special considerations for CPAP in children Not FDA approved Need wide variety of mask sizes and styles to fit children Compliance may be enhanced by behavioral techniques –Empowerment –Positive reinforcement –Desensitization –Role modeling

43
Positive Airway Pressure: Problems

45
CPAP Compliance Patient report: 75% Objectively measured use > 4 hrs for > 5 nights / week: 46% Asthma-medicine compliance: 30%

46
Strategies to Improve Compliance Improve nasal patency--THIS IS THE KEY Machine-patient interfaces –Masks –Nasal pillows –Chin straps Humidifiers Ramp Desensitization Bi-level pressure

47
Oral Appliances

48
Uvulopalatopharyngoplasty (UPPP)
")
49
Surgical alternatives in adults Reconstruct upper airway –Uvulopalatopharyngoplasty (UPPP) –Laser-assisted uvulopalatopharyngoplasty (LAUP) –Radiofrequency tissue volume reduction –Genioglossal advancement –Nasal reconstruction –Tonsillectomy Bypass upper airway –Tracheostomy
 –Laser-assisted uvulopalatopharyngoplasty (LAUP) –Radiofrequency tissue volume reduction –Genioglossal advancement –Nasal reconstruction –Tonsillectomy Bypass upper airway –Tracheostomy")
50
Uvulopalatopharyngoplasty (UPPP) Usually eliminates snoring 41% chance of achieving AHI < 20 No accurate method to predict surgical success Follow-up sleep study required
 Usually eliminates snoring 41% chance of achieving AHI < 20 No accurate method to predict surgical success Follow-up sleep study required")
51
Summary: Pediatric and Adult OSAS Dangerous Common ADHD symptoms in kids vs. sleepiness in adults Treatment: T&A in most kids vs. CPAP in most adults

52
Summary: Pediatric OSAS Not all kids with ADD or ADHD symptoms need OSAS evaluation Think about OSAS in kids with ADHD symptoms then ask about loud snoring, poor/disrupted sleep and look for adenotonsillar hypertrophy

Similar presentations






 286-7455 Fax: (703) 286-7462.>")






 in Children Bergen County School Nurses Association November 18, 2013 Lee D. Eisenberg M.D., M.P.H., F.A.C.S. ENT and.>")







