Download presentation
Presentation is loading. Please wait.

1
HYPER-BILIRUNEMIA

2
History Earliest work on jaundice from Baumes-1785, and Hervieux-1847
Kernicterus was first described by Johannes Orth, 1875 He postulated that jaundice might have hematologic origins He noted that the brain in jaundiced adults wasn’t affected Christian Schmorl coined the term in 1904 Translated, Kernicterus means jaundice of the “kern” or nuclear region of the brain

3
Jaundice… Exaggerated Hyperbilirubinemia
Polycythemia Hemolysis Rh incompatibility ABO incompatibility Abnormal RBCs—G6PD, spherocytosis, thalassemia Birth Trauma—Bruising, Cephalohematoma Metabolic Abnormalities—Crigler Najjar, Gilbert Syndrome, Galactosemia Medications—Sulfonamides Displaces bilirubin from albumin; same binding site

4
Causes of Hyper-bilirubinemia in the newborns:

5
Jaundice

6
Zona 1: 4 a 7 mg/dl; Zona 2: 5 a 8,5 mg/dl; Zona 3: 6 a 11,5 mg/dl; Zona 4: 9 a 17 mg/dl; Zona 5: > de 15 mg/dl. Adaptado de Kramer: AJDC 1069;118:454 y Finn: Acta Obstet Gynecol Scand 1975; 54:329

8
Pathophysiology RBCs are broken down
Bilirubin is an end product of heme metabolism Bilirubin is conjugated in the liver Enzyme: UDP-Glucuronyl Transferase Conjugated bili is excreted via the GI tract Enzyme: Beta-Glucuronidase can unconjugate bili in the small intestine and bili is reabsorbed

9
Pathophysiology of Newborn Hyperbilirubinemia
Relatively high hematocrit; more cells to break down UDP-Glucuronyl Transferase is not fully functional until 3- 4 months of life Relative starvation state and slow transit time, especially in breastfeeders Breastmilk contains beta-glucuronidase; enterohepatic circulation is increased

10
Pathophysiology UCB is lipophilic and crosses the Blood-Brain Barrier
In vitro, free UCB will not precipitate out of solution unless in the presence of a polar lipid membrane In theory, only free UCB crosses, albumin-bound does not. BBB of infants is more permeable than adults, and acidosis causes it to be even more permeable.

11
Pathophysiology…cont
UCB has an affinity for the basal ganglia, hippocampus, cranial nerve nuclei Mechanism is widely studied, but still unknown UCB interrupts metabolism in glial cells and causes apoptosis of neurons Exact mechanisms are unknown, but definitely separate pathways. Age of the cell is inversely proportional to susceptibility

14
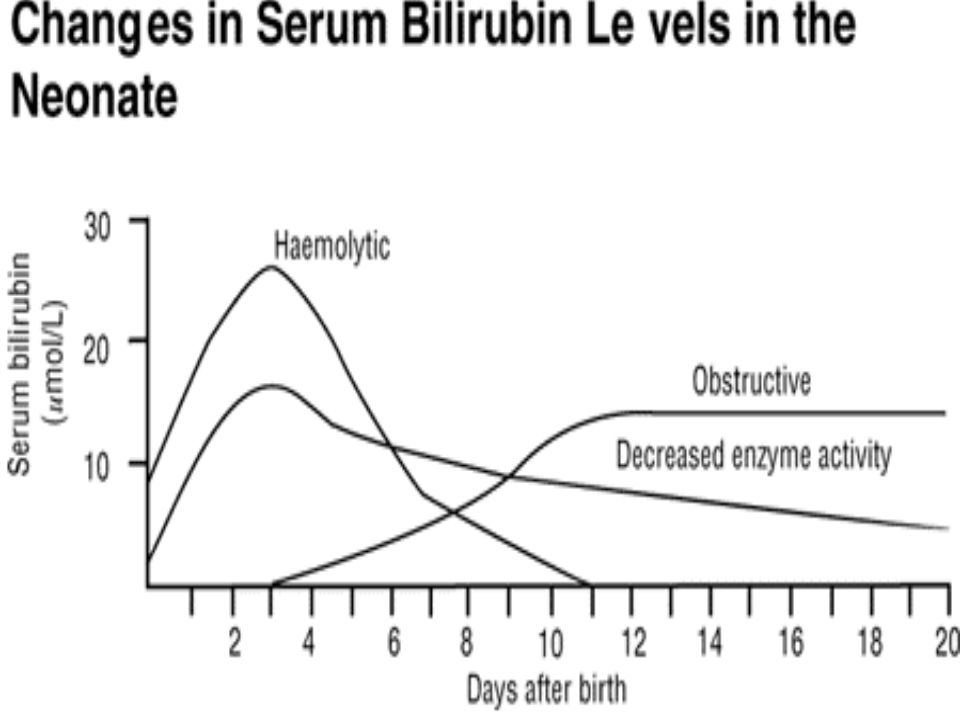
Phases of Physiological jaundice

15
In pre-term infant, bilirubin levels may peak as high as 10-12mg/dl at 4-5 days and decrease slowly over 2-4 weeks. Newborns produce twice as much bilirubin as do adults, because of:

16
Types of Un-conjugated Hyper-bilirubinemia

17
Physiological Jaundice
Immature hepatic function + increased bilirubin load from RBCs hemolysis..

18
Breast feeding associated jaundice-early
milk intake few calories Enterohepatic shunting In the intestine the enzyme (B- glucuronidase is able to convert conjugated bilirubin into unconjigated form reabsorbed by the intestinal mucosa transported to the liver

19
Hemolytic disease Breast-milk jaundice (late onset) Blood antigen incompatibility cause hemolytic or large numbers of RBCs where liver is unable to conjugate and excrete excess bilirubin from hemolysis. Caused by possible factors in the breast milk that prevent bilirubin conjugation, or less frequent stooling.

20
Diagnostic evaluation
Dx: serum level of bilirubin. Normal values: Unconjugated bilirubin= 0.2 to 1.4 mg/dl. Clinical dx depends on: TSB (Total serum bilirubin level) time on onset for the S&S GA at birth age in days post delivery. Family Hx and mother’s Rh factor evidence of hemolysis feeding method Infant physiological status
 time on onset for the S&S. GA at birth. age in days post delivery. Family Hx and mother’s Rh factor. evidence of hemolysis. feeding method. Infant physiological status.")
21
Laboratory Measures There is currently no lab value that correlates well with the development of kernicterus; there seem to be many factors that lead to its development Guidelines for initiating therapy for hyperbilirubinemia currently include the variables of UCB and age of baby. There are no good guidelines for preterm infants An unconjugated bilirubin level of 25 or less in TERM, HEALTHY babies has not been correlated with kernicterus Pediatrics 1995; Case reports of Term, Healthy, Breastfed babies—UCB levels associated with clinical Kernicterus were 39-50 It has been hypothesized that measuring UNBOUND UCB can be correlated, but not well supported as of yet

22
Pathological Jaundice
Appearance of jaundice within 24 hours of birth. Persistent jaundice after 1 week in full-terms babies, and more than 2 weeks for pre- term neonates. TSB > 12mg/dl. Increase in serum bilirubin 5mg/dl/day Direct bilirubin > 1.5 mg/dl.

23
Jaundice

24
Complications… Kernicterus (Bilirubin encephalopathy)
Def: is a syndrome of sever brain damage resulting from the deposition of unconjugated bilirubin In brain cells. The damage occurs when the serum concentration reaches toxic levels and crosses the BBB.

26
The yellow staining in the brain of a neonate is known as kernicterus.
There is a coronal section of medulla on the left and cerebral hemisphere on the right demonstrating kernicterus in deep grey matter of hemisphere and brain stem. Kernicterus is more likely to occur with prematurity, low birth weight, and increased bilirubin levels.

27
Complications…….cont Serum bilirubin level can’t predict the risk for brain injury alone, other factors put the newborn at high risk for encephalo-pathy are: Metabolic acidosis low serum albumin levels Intracranial infection as meningitis increased blood pressure any conditions that may increase metabolic demands for oxygen or glucose, (e.g. fetal distress, hypoxia, hypthermia, hypoglycemia). S&S: CNS depression or excitation, Lethargy and decreased activity, Irritability, Hypotonia and seizures…. May progress to defness, cerebral palsy, or mental retardation.
. S&S: CNS depression or excitation, Lethargy and decreased activity, Irritability, Hypotonia and seizures…. May progress to defness, cerebral palsy, or mental retardation.")
28
Therapeutic Management

29
Prevention: Treatment of Hyperbilirubinemia
Phototherapy Initiate based on UCB level and baby’s age Isomerizes UCB to Lumirubin, soluble in water and excreted via the kidney Exchange transfusion Initiate if phototherapy fails, repeat as needed Incidence of kernicterus has dropped since the advent Sn-Mesoporphyrin Inhibits Heme-oxygenase, which is the rate-limiting enzyme in heme catabolism. Only case reports thus far, where exchange transfusion was refused

30
Jaundice

32
Phototherapy ………( blue fluorescent light)
Bilirubin by photoisomerization soluble lumirubin (best in 1st 24-48hrs) What are the major nursing intervention at this stage? Pharmacological action of phenobarbital are: Increase bilirubin conjugation &hepatic clearance of the pigment in the bile 2. Increase albumin level thus increasing binding sites Feeding ( intestinal motility, establish N.Flora, ) hepatic shunting.
 What are the major nursing. intervention at this stage Pharmacological action of phenobarbital are: Increase bilirubin conjugation. &hepatic clearance of the pigment in the bile. 2. Increase albumin level thus increasing binding sites. Feeding ( intestinal motility, establish N.Flora, ) hepatic shunting.")
33
Some infants may also benefit from a fiberoptic pad underneath them, especially in the breastfed infant who is encouraged to feed 8-12 times in 24 hours. Serum bilirubin levels above 25 mg/dL or higher at any time is a medical emergency and the infant should be evaluated immediately for exchange transfusion

35
Jaundice

36
Jaundice

37
Phototherapy at home

38
When drwing blood samples, turn the light off, cover the sample

39
Jaundice mask Def: an excessive level of accumulated billirubin in the blood.

40
MRI of an infant who suffered from severe Erythroblastosis Fetalis

41
Sources Ahlfors, CE: Unbound Bilirubin Associated with Kernicterus: A Historical Approach. Journal of Pediatrics 2000; 137(4): Brodersen, R and L. Stern: Deposition of Bilirubin Acid in the CNS—A Hypothesis for the Development of Kernicterus: Acta Paediatr Scand 1990; 79: Hansen, TR: Pioneers in the Scientific Study of Neonatal Jaundice and Kernicterus. Pediatrics 2000; 106(2): e15. Kappas, A, et al: Sn-Mesoporphyrin Interdiction of Severe Hyperbilirubinemia in Jehovah’s Witness Newborns as an Alternative to Exchange Transfusion. Pediatrics 2001; 108(6):
: e15. Kappas, A, et al: Sn-Mesoporphyrin Interdiction of Severe Hyperbilirubinemia in Jehovah’s Witness Newborns as an Alternative to Exchange Transfusion. Pediatrics 2001; 108(6):")
Similar presentations









 Types of bilirubin: İndirect bilirubin=free bilirubin=unconjugated.>")












 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")

