Download presentation
Presentation is loading. Please wait.

1
Oncology Patient-Centered Medical Home
Oncology Management Services, Inc Building the Business Case for Quality and Value John D. Sprandio, MD, FACP October 3, 2014

2
Patient-Centered Medical Home
1967 Standards of Child Health Care American Academy of Pediatrics 2007 Joint Principles of the PCMH American Medical Association American Association of Family Practitioners American Academy of Pediatrics American College of Physicians American Osteopathic Association

3
Joint Principles of PCMH
Personal physician coordinates comprehensive care. Physician directed medical team. Whole person orientation for all stages of life (acute, chronic, preventive, and end-of-life care). Coordinated and integrated care across all aspects of the health care system utilizing information technology. Quality and safety with continuous quality improvement and recognition by a non-governmental body. Enhanced access through open scheduling and new communication tools. Appropriate payment recognizing the added value with the model.
. Coordinated and integrated care across all aspects of the health care system utilizing information technology. Quality and safety with continuous quality improvement and recognition by a non-governmental body. Enhanced access through open scheduling and new communication tools. Appropriate payment recognizing the added value with the model.")
4
NCQA Primary Care Recognition
Six Standards (validated, tested elements & features) Enhanced Access and Continuity Identify and Manage Populations Plan and Manage Care Provide Self-care Support and Community Resources Track and Coordinate Care Measure and Improve Performance
 Enhanced Access and Continuity. Identify and Manage Populations. Plan and Manage Care. Provide Self-care Support and Community Resources. Track and Coordinate Care. Measure and Improve Performance.")
5
Medical Neighborhood American College of Physicians
Council of Subspecialty Societies (CSS), Policy Paper 2010 Addressed relationship between primary care PCMH model and specialty/subspecialty practices Highlights: Established definition of Patient Centered Medical Home Neighbor Approved a framework to categorize interactions between PCMH and PCMH - N Approved guiding principles of the development of care-coordination agreements between PCMH and PCMH-N Neil Kirschner, Ph.D. American College of Physicians, Senior Associate Regulatory and Insurer Affairs
, Policy Paper Addressed relationship between primary care PCMH model and specialty/subspecialty practices. Highlights: Established definition of Patient Centered Medical Home Neighbor. Approved a framework to categorize interactions between PCMH and PCMH - N. Approved guiding principles of the development of care-coordination agreements between PCMH and PCMH-N. Neil Kirschner, Ph.D. American College of Physicians, Senior Associate. Regulatory and Insurer Affairs.")
6
Quality and Cost are Completely Intertwined
“The degree to which health services increase the likelihood of desired health outcomes and are consistent with current professional knowledge” (IOM 1997) Cost: Resource utilization related to delivery of care Value: “The degree to which health services increase the likelihood of desired health outcomes, are consistent with current professional knowledge AND are delivered with the proper allocation of resources” The utilization of unnecessary resources IS poor quality of care
 Cost: Resource utilization related to delivery of care. Value: The degree to which health services increase the likelihood of desired health outcomes, are consistent with current professional knowledge AND are delivered with the proper allocation of resources The utilization of unnecessary resources IS poor quality of care.")
7
Q V= C Value in Cancer Care Evidence based care Desired outcomes
NCCN guidelines COC program certification ASCO QOPI certification IOM reports Q C V= Desired outcomes Treatment Guideline adherence Appropriate therapy rendered Rational & Informed care at EOL

8
Care Team engagement essential in driving quality
Doing Well by Doing Good: Improving the Business Case for Quality Gosfield, Reinertsen, et al *2010 Update Care Team engagement essential in driving quality Centrality of the care team-patient relationship: Clinical team provides 1-on-1 interaction that defines healthcare Explanation, prediction, plan of care Physicians and advanced practitioners have the broadest scope of professional jurisdiction Drive provision of all goods and services The Care team is the portal to the rest of the system Referrals, education, interpretation of insurance benefits Care Team members face barriers on their way to becoming accountable for the quality and consistency of care they deliver

9
Barriers to quality = Care Team “time stealers”
Doing Well by Doing Good: Improving the Business Case for Quality Gosfield, Reinertsen, et al *2010 Update Barriers to quality = Care Team “time stealers” EMR, work-flow, niche competitors, documentation & communication hurdles. Variable: data collection, data presentation, decision support, outcome measures. Absence of real-time performance measurement, efficiency tools, and payer support. Care Team work environment redesign Standardize Simplify Make clinically relevant Engage patients Fix accountability at the locus of control

10
Creating Value Care Team Work Environment 2003
Addressing barriers to consistency and accountability Standardization of oncology processes Value Proposition Scalability Payer Response

11
Enhancing Value in Cancer Care
Addressing Care Team Barriers Streamline processes Standardize roles & responsibilities Minimize clinically irrelevant activity Improve patient/family engagement Fix accountability at locus of control Data systems tracking performance Continuously improve performance Q C V= Treatment Guideline adherence Appropriate therapy rendered Rational & Informed care at EOL Enhanced patient access Improved patient navigation, coordination & communication Reduced avoidable complications Reduced unnecessary utilization

12
Oncology Patient-Centered Medical Home®
NCQA level III, PCMH recognition April 2010 Integrated care delivery model for hematology & oncology PCMH principles: access, engagement, shared decisions, coordination, communication and accountability Medical oncology serves as the hub of coordination and accountability in meeting cancer care needs Integrates Primary PCMH, surgical, radiation oncology, inpatient, social, hospice services via information hub Value Proposition: Better cancer care, health, lower cost Payer recognition, integration with ACOs, Clinically Integrated Networks

13
Oncology PCMH Quality & Value Driver Diagram
Triple Aim Patient-,Payer-,and Provider-Centered Outcomes Primary Driver Care Team Environment Delivery Standards Services Secondary Drivers Process of Care Standards, Care Integration, Evidence Base Multi-disciplinary Guideline Concordance Engagement & Orientation Patient Responsibilities Practice Responsibilities Goals, Insurance Issues National Committee for Quality Assurance PCSP Recognition PCOC standards Patient & Family Experience of Care American College of Physicians PCMH-N Patient Navigation Multidisciplinary Input Scheduling & Tracking Palliation Symptom Management Focus on Performance Status (PS) Patient Advocacy NCCS, CSC, ACS Execution of Care Staging/Guideline Adherence Standardized Processes/Data Care Coordination Communication American College of Surgeons Commission on Cancer Data Collection NCDB Treatment & PC Standards Avoidable Resource Utilization ER/Hospitalizations Imaging & Lab NCCN Treatment Guidelines Survivorship Guidelines Symptom Management On Demand Access/Visits Performance data collection Track success of Palliation Survivorship Care Standardized Primary PCMH ASCO QOPI Standards Survivorship Guidelines Survivorship Care Standardized Care Plans Coordination Agreements End of Life Care Hospice Enrollment Place at Time of Death Resource Utilization Institute of Medicine National Quality Forum National Cancer Policy Forum Goals of Therapy Documented PS Driven Discussions Shared Decision Making Payer Based Episode and “OMH” Programs CMS & Commercial Total Cost Of Care Medical, Surgical, Lab Radiation, Imaging Data Driven Improvement ©2014 Oncology Management Services, Ltd.
 Patient Advocacy NCCS, CSC, ACS. Execution of Care Staging/Guideline Adherence Standardized Processes/Data Care Coordination Communication. American College of Surgeons. Commission on Cancer Data Collection NCDB Treatment & PC Standards. Avoidable Resource Utilization ER/Hospitalizations Imaging & Lab. NCCN Treatment Guidelines Survivorship Guidelines. Symptom Management On Demand Access/Visits Performance data collection Track success of Palliation. Survivorship Care Standardized Primary PCMH. ASCO QOPI Standards Survivorship Guidelines. Survivorship Care Standardized Care Plans Coordination Agreements. End of Life Care Hospice Enrollment Place at Time of Death Resource Utilization. Institute of Medicine National Quality Forum National Cancer Policy Forum. Goals of Therapy Documented PS Driven Discussions Shared Decision Making. Payer Based Episode and OMH Programs CMS & Commercial. Total Cost Of Care Medical, Surgical, Lab Radiation, Imaging. Data Driven Improvement. ©2014 Oncology Management Services, Ltd.")
14
Creating Value Care Team Work Environment
Standardization of oncology care processes Value Proposition Scalability Payer Response

15
Standardization of Oncology PCMH Processes
Consistent approach by the care team Patient Engagement & Orientation Patient Navigation Shared Decision-Making Execution of Care Care coordination Symptom Management Survivorship Care Goals of therapy

16
Standardization of Oncology PCMH Processes
Patient Engagement & Orientation Define role of nurse and patient navigators, physicians, etc Modes of enhanced access & coordination defined Financial counseling – details of insurance coverage Patient reporting & practice responsibilities Practice as “Point of First Triage” Symptom and disease management strategies (nurse triage) Patient Portal education Patient Navigation Shared Decision-Making Execution of Care Care coordination Symptom Management Survivorship Care Goals of therapy
 Patient Portal education. Patient Navigation. Shared Decision-Making. Execution of Care. Care coordination. Symptom Management. Survivorship Care. Goals of therapy.")
17
Standardization of Oncology PCMH Processes
Patient Engagement & Orientation Patient Navigation Lay Navigators Scheduling of all imaging, laboratory testing Precertification of necessary imaging Scheduling all external provider appointments Oncologic and non-oncologic Tracking test results and consultation reports to completion Re-scheduling when necessary Interface/scanning of reports Shared Decision-Making Execution of Care Care coordination Symptom Management Survivorship Care Goals of therapy

18
Standardization of Oncology PCMH Processes
Standardized Engagement & Orientation Patient Navigation Shared Decision-Making Explanation – specific TNM & molecular staging Prediction – natural history, impact on performance status Treatment options – consensus based guidelines Financial counseling – patient OOP expenses Patient Preferences – life goals, family responsibilities, hobbies Plan of Care – discussed and mutually agreed upon Goals of therapy defined – curative or palliative Written or electronic plan shared with patient/stakeholders Execution of Care Care coordination Symptom Management Survivorship Care Goals of therapy

19
Standardization of Oncology PCMH Processes
Patient Engagement & Orientation Patient Navigation Shared Decision-Making Execution of Care Standardized outpatient processes and work flow Patient self assessment questionnaire (PSAQ) Data collection and presentation drives decisions Adherence to multidisciplinary and chemotherapy guidelines Navigation, communication & coordination of all aspects of care Provider team accessibility Performance metrics monitored Care coordination Symptom Management Survivorship Care Goals of therapy
 Data collection and presentation drives decisions. Adherence to multidisciplinary and chemotherapy guidelines. Navigation, communication & coordination of all aspects of care. Provider team accessibility. Performance metrics monitored. Care coordination. Symptom Management. Survivorship Care. Goals of therapy.")
20
Standardization of Oncology PCMH Processes
Patient Engagement & Orientation Patient Navigation Shared Decision-Making Execution of Care Care coordination Multidisciplinary input – Primary, Surgery, Radiation, Medical Oncology Timeline of intervention discussed and scheduled Standardized communication among primary care & oncology teams Coordination of care between oncologist, primary and other specialists Coordination of care arrangements define responsibilities (PCMH-N) Transitions of care OP to ER or Admission, admission to OP Symptom Management Survivorship Care Goals of therapy
 Transitions of care OP to ER or Admission, admission to OP. Symptom Management. Survivorship Care. Goals of therapy.")
21
Standardization of Oncology PCMH Processes
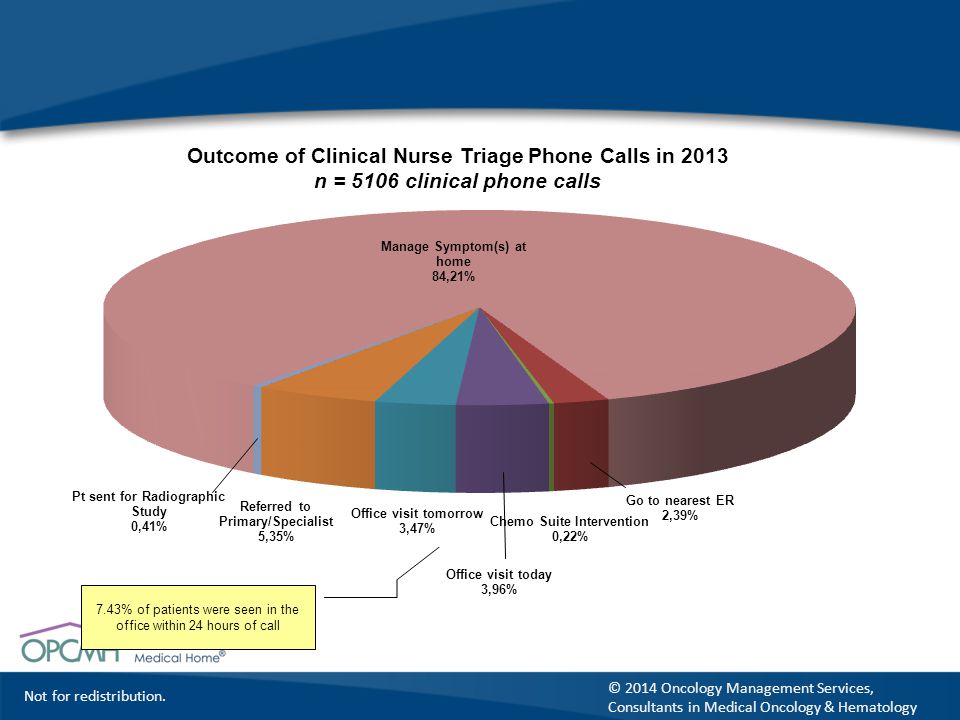
Patient Engagement & Orientation Patient Navigation Shared Decision-Making Execution of Care Care coordination Symptom management – during and between OP visits Standardized symptom data collection, grading & documentation Auto-populated fields in documentation driving physician response Longitudinal view of success of symptom management Documentation of specific recommendations shared with patient Telephone triage 24/7 - standardized algorithms Documentation of type and disposition of every call Survivorship Care Goals of therapy

22
Standardization of Oncology PCMH Processes
Patient Engagement & Orientation Patient Navigation Shared Decision-Making Execution of Care Care coordination Symptom Management Survivorship Care Consistent & Coordinated Care Plans Progress note templates integrated into software overlay “Assessment & Survivorship Care Plan” Coordination agreements with primary care team (ACP PCMH-N) Dissemination of information to all involved providers Enhanced patient interaction with community support services Goals of therapy
 Dissemination of information to all involved providers. Enhanced patient interaction with community support services. Goals of therapy.")
23
Standardization of Oncology PCMH Processes
Standardized Engagement & Orientation Patient Navigation Shared Decision-Making Execution of Care Care coordination Symptom Management Survivorship Care Goals of therapy Performance Status driven decision making in non-curative setting Standardized PS measurement Documentation of ongoing goals dialogue based on PS changes Goals of therapy updated via replay of: Explanation, Prediction, Options, Patient Preference, Plan of Care Hospice utilization monitored

24
Creating Value Care Team Work Environment Process standardization
Value Proposition – demonstration of results Scalability Payer Response

26
USON/Milliman: Approximately 2 emergency room visits per chemotherapy patient per year
(14 million commercially insured; 104,473 cancer patients) Source: Milliman analysis of Medstat 2007, Milliman Health Cost Guidelines 2009 © 2014 Oncology Management Services, Consultants in Medical Oncology & Hematology
 Source: Milliman analysis of Medstat 2007, Milliman Health Cost Guidelines © 2014 Oncology Management Services, Consultants in Medical Oncology & Hematology.")
27
USON/Milliman: Approximately 1 hospital admission per chemotherapy patient per year (n=14 million commercially insured; 104,473 cancer patients) Source: Milliman analysis of Medstat 2007, Milliman Health Cost Guidelines 2009

28
Multimodality Guidelines
NCCN multimodality care plans Consensus based recommendations Physician selects care plan within EMR Selection shared with billing, nursing staff NCCN Chemotherapy Guideline Compliance Adjuvant and first line metastatic Adherence > 95% – 2013 (CMOH) Practice and individual physician performance
 Practice and individual physician performance.")
29
Oncology PCMH Palliative Care
Concurrent delivery of palliative care Comprehensive health assessment each visit Symptoms: patient defined, RN/MA confirmed, physician accountable to respond NCI graded and longitudinally viewed Dynamic problem list of symptoms, co-morbid conditions Documentation of ongoing management Use of standardized approaches and instructions Patient view of documentation via portal

30
Oncology PCMH End of Life Care
Performance Status Driven Decision-Making PS: patient defined, RN/MA documentation, physicians accountable to respond PSAQ, ECOG grading (fixed), physician prompt PS longitudinally viewed by patient and physician Physician accountability Systems that monitor for changes in PS (ECOG 3) Documentation of rationale for continuation of therapy Transparency of discussion of goals Patient visibility of documentation via portal
, physician prompt. PS longitudinally viewed by patient and physician. Physician accountability. Systems that monitor for changes in PS (ECOG 3) Documentation of rationale for continuation of therapy. Transparency of discussion of goals. Patient visibility of documentation via portal.")
31
Oncology PCMH Survivorship Care
Care team: NP/PA + physician collaboration Survivorship care plan templates (ASCO) Clinical summary (toxicities, co-morbidities) Documentation of management of residual symptoms Treatment summary, genetic testing, family history Surveillance and screening activities, immunizations Community resource utilization Coordination of care arrangements in survivorship Responsibility matrix defined Primary PCMH, Oncology PCMH, Radiation and Surgical teams
 Clinical summary (toxicities, co-morbidities) Documentation of management of residual symptoms. Treatment summary, genetic testing, family history. Surveillance and screening activities, immunizations. Community resource utilization. Coordination of care arrangements in survivorship. Responsibility matrix defined. Primary PCMH, Oncology PCMH, Radiation and Surgical teams.")
32
Oncology PCMH Transitions of Care
Transition responsibility: facilitating hand-offs Symptomatic patients with an apparent new malignancy from ER, Primary PCMH or specialist office Oncology team drives efficiency, shortening timeline to diagnosis, symptom control and treatment Symptom control = reduced unnecessary ER visits, admission From oncology office to ER or inpatient admission Transfer of information to accepting parties Notification to Primary PCMH team From acute care to outpatient or skilled care Scheduling of all testing, consultation and follow-up visits

33
Creating Value Care Team Work Environment Process standardization
Value Proposition Scalability Payer Response

34
Scalability of Model Address care team barriers (Readiness Assessment)
Process and technology framework: merging work-flow, data collection/presentation, documentation, communication Standards, elements and features of care processes Oncology specific (NCQA, COC, TJC) Internal feedback of relevant practice performance data Knowledge driven continuous improvement Payer Response Alternate Payment Methods
 Internal feedback of relevant practice performance data. Knowledge driven continuous improvement. Payer Response. Alternate Payment Methods.")
35
PCORI-NCQA-ASCO-OMS PCORI funded Oncology Project (SEPA)
NCQA, OMS, ASCO, RAND, NCCS, IBC PCSP Recognition PCOC Recognition

36
Patient-Centered Specialty Practice (PCSP)
Track & Coordinate Referrals Referral Process and Agreements (MP) Referral Content Referral Response (MP) Provide Access & Communication Access Electronic Access Specialty Practice Responsibilities Culturally and Linguistically Appropriate Services The Practice Team (MP) Identify & Coordinate Patient Populations Patient Information Clinical Data D. Coordinate Patient Populations Plan & Manage Care Care Planning and Support Self-Care Medication Management (MP) Use Electronic Prescribing 5. Track & Coordinate Care Test Tracking and Follow-Up Referral Tracking and Follow-Up Coordinate Care Transitions 6. Measure & Improve Performance Measure Performance Measure Patient/Family Experience Implement and Demonstrate Continuous Quality Improvement (MP) Report Performance Use Certified EHR Technology
 Referral Content. Referral Response (MP) Provide Access & Communication. Access. Electronic Access. Specialty Practice Responsibilities. Culturally and Linguistically Appropriate Services. The Practice Team (MP) Identify & Coordinate Patient Populations. Patient Information. Clinical Data. D. Coordinate Patient Populations. Plan & Manage Care. Care Planning and Support Self-Care. Medication Management (MP) Use Electronic Prescribing. 5. Track & Coordinate Care. Test Tracking and Follow-Up. Referral Tracking and Follow-Up. Coordinate Care Transitions. 6. Measure & Improve Performance. Measure Performance. Measure Patient/Family Experience. Implement and Demonstrate Continuous Quality Improvement (MP) Report Performance. Use Certified EHR Technology.")
37
Patient-Centered Oncology Care (PCOC)
Track & Coordinate Referrals Referral Process and Agreements (L) Referral Content (L) Referral Response (M) Provide Access & Communication Access (H) Electronic Access (L) Specialty Practice Responsibilities (M) Culturally and Linguistically Appropriate Services (CLAS) (L) The Practice Team (H) Identify & Coordinate Patient Populations Patient Information (M) Clinical Data (L) C. Comprehensive Health Assessment (H) D. Coordinate Patient Populations (L) E. Evidence-based Decision Support (H) Plan & Manage Care Care Planning and Support Self-Care (H) Medication Management (H) Use Electronic Prescribing (L) 5. Track & Coordinate Care Test Tracking and Follow-Up (L) Referral Tracking and Follow-Up (M) Coordinate Care Transitions (H) Measure & Improve Performance Measure Performance (L) Measure Patient/Family Experience (L) Implement and Demonstrate Continuous Quality Improvement (M) Report Performance (L) Use Certified EHR Technology (L) Element Priority: Low (L); Medium (M); High (H)
 Referral Content (L) Referral Response (M) Provide Access & Communication. Access (H) Electronic Access (L) Specialty Practice Responsibilities (M) Culturally and Linguistically Appropriate Services (CLAS) (L) The Practice Team (H) Identify & Coordinate Patient Populations. Patient Information (M) Clinical Data (L) C. Comprehensive Health Assessment (H) D. Coordinate Patient Populations (L) E. Evidence-based Decision Support (H) Plan & Manage Care. Care Planning and Support Self-Care (H) Medication Management (H) Use Electronic Prescribing (L) 5. Track & Coordinate Care. Test Tracking and Follow-Up (L) Referral Tracking and Follow-Up (M) Coordinate Care Transitions (H) Measure & Improve Performance. Measure Performance (L) Measure Patient/Family Experience (L) Implement and Demonstrate Continuous Quality Improvement (M) Report Performance (L) Use Certified EHR Technology (L) Element Priority: Low (L); Medium (M); High (H)")
38
Creating Value Care Team Work Environment Process standardization
Value Proposition Scalability Payer Response

39
Payment Reform PCORI funded Oncology Project (SEPA) NCQA, OMS, ASCO, RAND, NCCS, IBC CMS Oncology Payment Reform TEP MITRE, Brookings, RAND, CMS, CMMI Oncology Bundled Payment Consortium CAP, CMS, CMMI, multiple payers ASCO Payment Reform Initiatives OMS CMOH Alternate Payment Methods in SEPA IBC, Keystone First, (48% of patients)
 NCQA, OMS, ASCO, RAND, NCCS, IBC CMS Oncology Payment Reform TEP MITRE, Brookings, RAND, CMS, CMMI Oncology Bundled Payment Consortium CAP, CMS, CMMI, multiple payers ASCO Payment Reform Initiatives OMS CMOH Alternate Payment Methods in SEPA IBC, Keystone First, (48% of patients)")
40
Provider Ability & Accountability Payment Reform for cancer care
Episode or Budgeted Payment model FFS Pathways OPCMH

41
CMS Oncology Care Model (OCM)
Combined features of CMS Oncology Payment Reform TEP + CAP Bundled Payment Consortium Medical oncology treatment episodes - broadly applied PCMH Practice Transformation Patient Navigators Enhanced Coordination Structured Care Plan (IOM) 24/7 access to clinician with records Adherence to nationally recognized treatment guidelines Oncology specific EHR, stage 2 MU by end of year three Data driven quality improvement program
 24/7 access to clinician with records. Adherence to nationally recognized treatment guidelines. Oncology specific EHR, stage 2 MU by end of year three. Data driven quality improvement program.")
42
CMS Oncology Care Model (OCM)
Performance Metrics – reported quarterly Driven by Care Team execution of PCMH processes ER visits/Hospital admissions (episode + 6 months & EOL) CAHPS (oncology version) Comprehensive health assessment, including PS Psychological screening (once/episode) Palliative care (concurrently or via formal consultation) Transition coordination and follow-up testing/OP visits Medication reconciliation Pain management Hospice Utilization Resource Utilization (Drugs, radiation therapy, imaging, laboratory) Results of data driven quality improvement efforts
 CAHPS (oncology version) Comprehensive health assessment, including PS. Psychological screening (once/episode) Palliative care (concurrently or via formal consultation) Transition coordination and follow-up testing/OP visits. Medication reconciliation. Pain management. Hospice Utilization. Resource Utilization (Drugs, radiation therapy, imaging, laboratory) Results of data driven quality improvement efforts.")
43
Principles of PCMH-N Applied to Cancer Care
PCMH standards + supportive technology applied to primary and specialty care enables a neighborhood of practices that deliver what Don Berwick called for in 2012: “…. an electronic line-of-sight contact with each other all day long, weaving a net of help and partnership with patients and families.”

Similar presentations