Download presentation
Presentation is loading. Please wait.

1
The Physician Market, Part 2 Professor Vivian Ho Health Economics Fall 2007 These slides draw from material in Santerre & Neun, Health Economics, Theories, Insights and Industry Studies, Thomson Press 2007

2
Advantages of capitation for physicians Increased clinical autonomy uPhysician financially responsible for cost overruns èEliminates need for external review Increased income uPhysician compensated by risk pools created from withholds if can reduce utilization of hospital, outpatient, diagnostics, other ancillary services

3
MCOs and Physician Conduct l HMOs combine the insurance and production functions in health care. l They are different from traditional indemnity (FFS) plans, in that they attempt to control how health care is provided. l How do HMOs influence physicians?
 plans, in that they attempt to control how health care is provided. l How do HMOs influence physicians .")
4
Types of Managed Care Orgs

5
MCOs and Physician Conduct l Staff model HMOs pay physicians a salary. No incentive to over-provide care. l IPA HMOs usually pay physicians discounted FFS. Physicians have incentive to over-provide care. How can the HMO control costs?

6
MCOs and Physician Conduct l Caution: Distinctions between different types of HMOs are blurring over time. 28% of staff HMOs pay based on salary only ( Gold, 1996 ). 90% of PPOs use discounted FFS.
. 90% of PPOs use discounted FFS..")
7
Financial Risk Arrayed on a Spectrum from Full Risk for the Insurer to Full Risk for the Provider HBS Case Study 9-698-060, Note on Managed Care

8
Additional MCO Compensation Tools l Risk sharing - The insurer can make the physician bear some of the risk of insuring the patient, so that the physician will also feel the need to restrain medical costs. Capitation Withholdings Bonuses

9
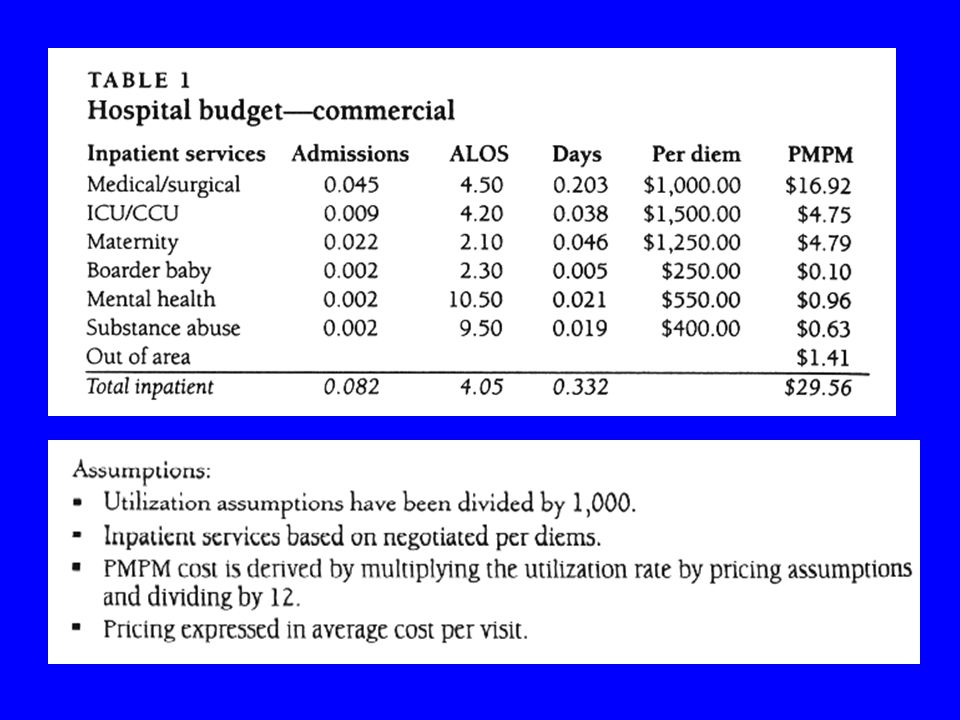
Additional MCO Compensation Tools l Capitation - Physician receives a fixed payment per person in return for providing medical services regardless of the quantity of medical care delivered. l e.g. A physician may receive $9 per member per month for each enrollee who chooses an HMO plan and elects him to be their primary care caregiver.

10
Additional MCO Compensation Tools l Capitation Physician has an incentive to restrict # of patient visits. Problem - Physician can reduce visits by referring patients to other providers in the same HMO plan. l e.g. If the patient has high blood pressure, refer her to a cardiologist. Solution - Withholding

11
Additional MCO Compensation Tools l Even if docs paid thru capitation, HMO responsible for costs of hospital services, outpatient diagnostic tests, physician referrals. l How can the HMO limit these costs? Withhold a portion of physician payment (PMPM) until end of fiscal year.
 until end of fiscal year..")
12
HMO Reimbursement Strategies l Assign these funds to specific expenditure categories (e.g. lab tests). l At end of year, return a portion of the withhold to physicians if surplus exists in that expenditure category. l Can even change next year’s withhold or capitation based on this year’s performance.
. l At end of year, return a portion of the withhold to physicians if surplus exists in that expenditure category. l Can even change next year’s withhold or capitation based on this year’s performance..")
13
Additional MCO Compensation Tools lBonuses - MCOs can give a portion of their profits at the end of the year to physicians who elect cost-effective behavior. e.g. Pay bonuses to primary caregivers who reported lower number of specialist referrals.

15
Advantages of capitation for physicians Improved cash flow uPhysician receives fixed payment per patient each month èReduces bad debt expenses Better budgeting uSteady cash flow - well-defined budgets uEasier to identify and correct sources of cost overruns

16
4 Components of a Capitated Contract 1) Covered Services Definitions such as “primary care services within the physician’s scope of practice” are too vague Examples of capitated primary services:
 Covered Services Definitions such as primary care services within the physician’s scope of practice are too vague Examples of capitated primary services:")
17
Examples of Current Procedure Terminology l 99201 Initial office visit for an out-of-town patient requiring topical refill (Dermatology) Initial office visit for a 65-year-old male for reassurance about an isolated seborrheic keratosis on upper back (Plastic surgery) Initial office visit for a 10-year old male, for limited subungual hematoma not requiring drainage (Internal Medicine)
 Initial office visit for a 65-year-old male for reassurance about an isolated seborrheic keratosis on upper back (Plastic surgery) Initial office visit for a 10-year old male, for limited subungual hematoma not requiring drainage (Internal Medicine)")
18
l Carve outs - specific services or patients singled out in the capitation contract for special consideration Usually for expensive, infrequent services e.g. HIV+ patients, mental health, organ transplants Can be paid on fee-for-service (FFS) basis, or separate providers may contract for carve outs
 basis, or separate providers may contract for carve outs.")
19
Components of a Capitated Contract Payment methods u Capitation rate/schedule - Managed care organizations employ actuaries who predict the cost of care as a function of population characteristics

24
lTiming of payments u Payment of carve out services u Payment withholds used to fund risk pools, and method for risk pool distribution u Methods for limiting risk (e.g. reinsurance, stop-loss) u Insurer may agree to assume treatment costs that exceed a predefined threshold amount
 u Insurer may agree to assume treatment costs that exceed a predefined threshold amount.")
25
List of other requirements u Quality assurance activities l May require reporting detailed patient data è More sophisticated, costly record keeping u Required office/call hours u Use of physician extenders u Copayment procedures u “most-favored-nation” clause u Additional professional liability insurance coverage

26
Process for termination u Provisions for termination without cause l Can be financially risky to physician u Provisions for termination with cause l Should specify specific conditions l e.g. failure to comply w/ quality assurance requirements u Contract should specify physician responsibilities if managed care organization insolvent l “Continuation of care” requirements l Usually must complete patient’s course of treatment until satisfactory arrangements made to secure treatment elsewhere

27
Evidence on Physicians & MCO Compensation l 57% of MCOs base pay on utilization or costs measures l Almost half of MCOs consider patient complaints and quality measures

28
Evidence on Physicians & MCO Compensation l MCOs paying physicians a salary had 13.1% fewer hospitalization days per 1,000 enrollees per yr. relative to FFS l Capitation led to 7.5% fewer hospitalization days l Physicians faced w/ withholds had 10.5% fewer visits per enrollee l Caution: The studies did not determine whether profits rose, or whether quality of patient care was affected

29
Physician Market Performance lPhysician expenditures have slowed in the 1990s, more in line with the growth of the overall economy. But they may be on the rise again

30
Physician Market Performance Revenue per Self-Employed Physician, ($1,000s) Increases in revenues are due to increases in expenses AND higher income for physicians
 Increases in revenues are due to increases in expenses AND higher income for physicians")
31
Physician salaries remain high l When managed care grows, salary growth for specialists slows, while pay for primary care docs rises l Physician groups getting large enough to want their own specialists l Female docs’ salaries exceed males in a dozen or so specialties

32
Employed vs. Independent Physicians l Employed physicians worked 5-7 fewer hours a week l Employed physicians’ median net income was $142,000 in 1996, vs. $198,000 for all private-practice physicians l Practice mgmt. Companies typically pay physicians $300,000-$400,000 per physician for practice assets (land, equipment) Tradeoff: 20% of practice’s net revenues
 Tradeoff: 20% of practice’s net revenues.")
33
Physician Practice Management (PPMs) l PPMs act as liaisons between insurers and doctors by acquiring physician practices l Advantages: Economies of scale in operational costs Improved risk assessment for managed care Finance new information systems Retain patient revenues by keeping referrals within the PPM network
 l PPMs act as liaisons between insurers and doctors by acquiring physician practices l Advantages: Economies of scale in operational costs Improved risk assessment for managed care Finance new information systems Retain patient revenues by keeping referrals within the PPM network")
34
Fortune Magazine, March 3, 1997

35
l MedPartners Provider Network acts as an intermediary, accepting capitated payments from HMOs & paying claims to the company’s network providers Patients buy insurance from PacifiCare Health Systems, Foundation Health Systems Inc., etc. Had up to 19,200 doctors in the PPM division in hundreds of physician clinics at one point

36
l MedPartners posted a net loss of $1.26b on revenues of $2.6b in 1998 l Loss of $821m on $2.4b in revenues in 1997

37
What Went Wrong l Failure to integrate its operations or provide systems to operate more efficiently than they had done independently Lacked actuarial expertise to predict medical costs California: Plan underestimated incurred-but- not-reported claims liability & could not estimate a dollar value for the large backlog of unprocessed claims Failed to invest in information systems, medical equipment, or expansion of medical services to boost a group’s internal growth

38
What Went Wrong l MedPartners bought new practices at a furious rate, often at hefty prices Industry buying spree boosted the prices of physician practices l Doctors didn’t react well to becoming employees of remote national companies Physicians who sold their practices didn’t feel the need to work as hard, younger doctors’ salaries lower due to cut taken by the PPM

39
MedPartners’ Reaction l MedPartners exited the PPM business and became Caremark, which is in the Pharmaceutical Benefits Management (PBM) market
 market")
40
The Future of PPMs l Doctors will continue to organize in larger groups to avoid hassles of office admin and managed-care contracting l Smaller single-specialty PPMs seem more committed to improving operations l # of publicly traded PPMs (~30) may shrink by 50%
 may shrink by 50%")
Similar presentations










 Sandy H. Yoo May 5, 2006.>")

>")










