Download presentation
Presentation is loading. Please wait.

1
Treatments for Anxiety
Stacy Shaw Welch, PhD Anxiety and Stress Reduction Center (ASRC) of Seattle June 2, 2010 FCAP Seminar Series / Partners for our Children What anxiety is: how to identify anxiety, distinguishing between “normal” or situational anxiety and a persisting anxiety disorder Specific anxiety disorders seen in children, adolescents and adults The latest research on treatment on treatments for anxiety disorders across development Ways to use “modular” treatment approaches for anxiety to help, from simple to very complex presentations
 of Seattle. June 2, FCAP Seminar Series / Partners for our Children. What anxiety is: how to identify anxiety, distinguishing between normal or situational anxiety and a persisting anxiety disorder. Specific anxiety disorders seen in children, adolescents and adults. The latest research on treatment on treatments for anxiety disorders across development. Ways to use modular treatment approaches for anxiety to help, from simple to very complex presentations.")
2
Overview Part 1 – Understanding anxiety
Part 2 – Treating anxiety: First line treatment approaches for anxiety Part 3 – Concepts of Modular Treatment (moving from Evidence Based Treatment to Evidence Based Practice) Part 4 - Introduction to Modules for Anxiety Treatment
 Part 4 - Introduction to Modules for Anxiety Treatment.")
3
Fear, Anxiety, and Anxiety Disorders

4
What is anxiety? Fear: focused response to a known or definite threat
Fight or flight response Necessary for survival Anxiety: fear response in the absence of clear danger (anticipation or possibility) Universal experience / wide range of normal Can be useful/ functional
 Universal experience / wide range of normal. Can be useful/ functional.")
5
What is an anxiety disorder?
Persistent anxiety over time around situations that are not objectively dangerous / anxiety not appropriate to developmental level Causes Marked distress Impairment in functioning Note: this can be obvious or more subtle in children (e.g., family system is organized around child’s anxiety)
")
6
Anxiety vs. Anxiety Disorder
More a matter of degrees Example of separation anxiety: Normal / functional at specific developmental stages Some children show increased S.A. as a result of traumatic conditioning Some children show increased S.A. with no traumatic conditioning Some children would have such severe or longlasting symptoms that it would meet criteria for a disorder

7
Anxiety disorders Separation anxiety disorder Specific phobia
Social phobia Panic disorder/agoraphobia Generalized anxiety disorder (GAD) Posttraumatic stress disorder (PTSD)/ Acute stress disorder (ASD) Obsessive compulsive disorder (OCD)
 Posttraumatic stress disorder (PTSD)/ Acute stress disorder (ASD) Obsessive compulsive disorder (OCD)")
8
Development of Anxiety
Biology + learning Genetics, temperament clearly influence who becomes anxious Environment powerful source of learning and continued “wiring” of the brain to either anticipate lack of control and danger or safety and resources to cope Transaction between the two continues over the lifespan –this is the tragedy and great hope

9
Development of Anxiety
Another important transaction: the interaction of anxious behaviors and the environment Anxiety “pulls” for certain behaviors from the environment These environmental responses can further reinforce anxiety and prevent corrective learning experiences

10
Treating Anxiety: Brief Review of Research

11
Treatment Two main treatment approaches for children, teens and adults
CBT – by far most well researched and effective treatment for anxiety. Should be first-line intervention, combined with meds for moderate or severe disorder. Medication – SSRIs first, then augmentation strategies

12
What is CBT? -Skills based, problem-solving, very practical approach to emotionally driven problems/behaviors -Patients learn to take “bite-sized” small steps towards health -Biopsychosocial model as opposed to purely biomedical model Should include at least 4 elements: education/monitoring, tools to calm physiology, cognitive restructuring, exposure Note that we’ll review all of these later WSPA 2008 / asrcseattle.com

13
What kinds of problems can it be used for?
Think behavior change, esp. emotionally driven behaviors Depression * Anxiety disorders** Unexplained medical illness / somatization Chronic pain management Eating disorders (bulimia and binge eating) Insomnia (primary and secondary) Addictions Non-adherence to medical recommendations Lifestyle / Behaviors linked to chronic disease care (physical activity, diet, social support, medications, etc.) Child internalizing and depressive disorders** Marital distress Anger status of cognitive-behavioral therapy: A review of meta-analyses. Author: Butler, Andrew C Source: Clinical Psychology Review Vol. 26, Iss. 1. In this review of 16 recent meta-analyses we sought to answer a multifaceted question: How effective is CBT, for which disorders, and compared to what, and how lasting are these effects? Collectively, the findings detailed in A.C. Butler et al. / Clinical Psychology Review 26 (2006) 17–31 27 this review suggest that CT is highly effective for adult unipolar depression, adolescent unipolar depression, generalized anxiety disorder, panic disorder with or without agoraphobia, social phobia, PTSD, and childhood depressive and anxiety disorders. The comparison-weighted grand mean effect size for these disorders when compared to no-treatment, wait list, or placebo controls is 0.95 (SD=0.08). CBT is associated with large improvements in symptoms for bulimia nervosa, and the associated effect sizes (M=1.27, SD=0.11) are significantly larger than those that have been found for pharmacotherapy. CBT also has shown promising results as an adjunct to pharmacotherapy in the treatment of schizophrenia. The average uncontrolled effect size of 1.23 for CBT compares favorably with an ES of 0.17 for schizophrenic patients receiving only routine care. Moderate effect sizes (M=0.62, SD=0.11) were obtained when CT was compared to controls for marital distress, anger, childhood somatic disorders, and several chronic pain variables (i.e., pain expression behavior, activity level, social role functioning and cognitive coping and appraisal). CT was somewhat superior to antidepressants in the treatment of adult unipolar depression (ES=0.38). CT was equally effective to behavior therapy in the treatment of adult depression (ES=0.05) as well as obsessive-compulsive disorder (ES=0.19). Trauma-focused CBT and EMDR were equally effective for PTSD. The efficacy of CT for sexual offending is relatively low (ES=0.35). However, along with hormonal treatments, it is the most effective treatment for reducing recidivism in this population. Finally, CT was found to be superior to supportive/nondirective therapy in the few occurrences when these two treatments were directly compared. This includes two comparisons for adolescent depression (ES=0.84) and two comparisons for generalized anxiety disorder (ES=0.71). We also aimed to provide answers regarding the degree to which the effects of CT persist following the termination of treatment. The meta-analyses reviewed strongly suggest that across many disorders the effects of CT are maintained for substantial periods beyond the cessation of treatment. More specifically, significant evidence for long-term effectiveness was found for depression, generalized anxiety, panic, social phobia, OCD, sexual offending, schizophrenia, and childhood internalizing disorders. In the cases of depression and panic, there appears to be robust and convergent meta-analytic evidence that CT produces vastly superior long-term persistence of effects, with relapse rates half those of pharmacotherapy. In addition, CT appears to show greater long-term effects in the treatment of generalized anxiety disorder as compared to applied relaxation. This review of existing meta-analyses adds to our knowledge of the effects of CT for a variety of disorders. However, future meta-analyses should (1) continue to evaluate the effects of CBT as applied to an even wider, more specific spectrum of disorders, (2) continue to evaluate the long-term effects of CBT, and (3) continue to evaluate the effects of CBT as compared to alternative treatments. For example, with respect to the former, Lam et al. (2003), in a randomized controlled trial of CBT for relapse prevention in Bipolar Disorder, found that patients treated with CBT experienced significantly better outcomes (e.g., fewer and shorter bipolar episodes, fewer hospital admissions, less variability in manic symptoms, etc.) at 1 year follow-up. However, because there are currently no meta-analytic findings on CBT for Bipolar Disorder, the WSPA 2008 / asrcseattle.com
 Insomnia (primary and secondary) Addictions. Non-adherence to medical recommendations. Lifestyle / Behaviors linked to chronic disease care (physical activity, diet, social support, medications, etc.) Child internalizing and depressive disorders** Marital distress. Anger. status of cognitive-behavioral therapy: A review of meta-analyses. Author: Butler, Andrew C Source: Clinical Psychology Review Vol. 26, Iss. 1. In this review of 16 recent meta-analyses we sought to answer a multifaceted question: How effective is CBT, for which disorders, and compared to what, and how lasting are these effects Collectively, the findings detailed in. A.C. Butler et al. / Clinical Psychology Review 26 (2006) 17– this review suggest that CT is highly effective for adult unipolar depression, adolescent unipolar depression, generalized anxiety disorder, panic disorder with or without agoraphobia, social phobia, PTSD, and childhood. depressive and anxiety disorders. The comparison-weighted grand mean effect size for these disorders when. compared to no-treatment, wait list, or placebo controls is 0.95 (SD=0.08). CBT is associated with large. improvements in symptoms for bulimia nervosa, and the associated effect sizes (M=1.27, SD=0.11) are significantly. larger than those that have been found for pharmacotherapy. CBT also has shown promising results as an. adjunct to pharmacotherapy in the treatment of schizophrenia. The average uncontrolled effect size of 1.23 for CBT. compares favorably with an ES of 0.17 for schizophrenic patients receiving only routine care. Moderate effect sizes. (M=0.62, SD=0.11) were obtained when CT was compared to controls for marital distress, anger, childhood. somatic disorders, and several chronic pain variables (i.e., pain expression behavior, activity level, social role. functioning and cognitive coping and appraisal). CT was somewhat superior to antidepressants in the treatment of. adult unipolar depression (ES=0.38). CT was equally effective to behavior therapy in the treatment of adult. depression (ES=0.05) as well as obsessive-compulsive disorder (ES=0.19). Trauma-focused CBT and EMDR were. equally effective for PTSD. The efficacy of CT for sexual offending is relatively low (ES=0.35). However, along. with hormonal treatments, it is the most effective treatment for reducing recidivism in this population. Finally, CT. was found to be superior to supportive/nondirective therapy in the few occurrences when these two treatments were. directly compared. This includes two comparisons for adolescent depression (ES=0.84) and two comparisons for. generalized anxiety disorder (ES=0.71). We also aimed to provide answers regarding the degree to which the effects of CT persist following the termination. of treatment. The meta-analyses reviewed strongly suggest that across many disorders the effects of CT are. maintained for substantial periods beyond the cessation of treatment. More specifically, significant evidence for. long-term effectiveness was found for depression, generalized anxiety, panic, social phobia, OCD, sexual offending, schizophrenia, and childhood internalizing disorders. In the cases of depression and panic, there appears to be robust. and convergent meta-analytic evidence that CT produces vastly superior long-term persistence of effects, with relapse. rates half those of pharmacotherapy. In addition, CT appears to show greater long-term effects in the treatment of. generalized anxiety disorder as compared to applied relaxation. This review of existing meta-analyses adds to our knowledge of the effects of CT for a variety of disorders. However, future meta-analyses should (1) continue to evaluate the effects of CBT as applied to an even wider, more. specific spectrum of disorders, (2) continue to evaluate the long-term effects of CBT, and (3) continue to evaluate the. effects of CBT as compared to alternative treatments. For example, with respect to the former, Lam et al. (2003), in a. randomized controlled trial of CBT for relapse prevention in Bipolar Disorder, found that patients treated with CBT. experienced significantly better outcomes (e.g., fewer and shorter bipolar episodes, fewer hospital admissions, less. variability in manic symptoms, etc.) at 1 year follow-up. However, because there are currently no meta-analytic. findings on CBT for Bipolar Disorder, the. WSPA 2008 / asrcseattle.com.")
14
Specific Approaches to Anxiety Treatment
Adults: a manual (or two, or three) for each anxiety disorder Children: Not much until 1980’s (DSM-III) Early approaches: adult techniques and theories with child-language Major studies / treatments to know: CBT for anxiety: “Coping Cat”, “Coping Koalla (Kendall, Barrett) Talking Back to OCD: ERP (March), POTS CAMS (meds plus CBT) TFCBT – Trauma – focused CBT Modular treatments emphasizing exposure (Chorpita) Print tomorrow.
 for each anxiety disorder. Children: Not much until 1980’s (DSM-III) Early approaches: adult techniques and theories with child-language. Major studies / treatments to know: CBT for anxiety: Coping Cat , Coping Koalla (Kendall, Barrett) Talking Back to OCD: ERP (March), POTS. CAMS (meds plus CBT) TFCBT – Trauma – focused CBT. Modular treatments emphasizing exposure (Chorpita) Print tomorrow.")
15
Coping Cat (Kendall et al, 1994, 1997)
16-session CBT program for overanxious (GAD), separation, social anxiety, adjustment problems “Coping Cat” 7-14, “Cat” 14-18 50-64% no longer met anxiety disorder criteria Gains maintained at 1 year / 3 year follow up (5% waitlist) “F.E.A.R” plan takes children through elements of CBT including techniques to calm their bodies, cognitive restructuring, exposure, and rewards Just print for notes then delete
, separation, social anxiety, adjustment problems. Coping Cat 7-14, Cat % no longer met anxiety disorder criteria. Gains maintained at 1 year / 3 year follow up (5% waitlist) F.E.A.R plan takes children through elements of CBT including techniques to calm their bodies, cognitive restructuring, exposure, and rewards. Just print for notes then delete.")
16
CBT, Meds, and combination: what’s best?
CAMS study (Dec. 2008) 488 Children, ages 7 – 17 Primary diagnoses of SAD, GAD, social phobia Randomized to 14 sessions of CBT, up to 200 mg. of sertraline, combination therapy, or placebo Results: “much improved” or “very much improved” on CGI CBT alone: 59.7% Sertraline alone: 54.9% Placebo: 23.7% Combination: 80.7%
 488 Children, ages 7 – 17. Primary diagnoses of SAD, GAD, social phobia. Randomized to 14 sessions of CBT, up to 200 mg. of sertraline, combination therapy, or placebo. Results: much improved or very much improved on CGI. CBT alone: 59.7% Sertraline alone: 54.9% Placebo: 23.7% Combination: 80.7%")
17
Conceptual framework for Modular Treatment of Anxiety

18
Modular treatment Addressing what happens when you try to apply evidence based treatment in community settings with Complex clients Complex situations Logistical challenges (e.g., time)
")
19
Evidence-based treatments vs. practice
“interventions or techniques that have produced therapeutic change in controlled trials” (Kazdin, 2008) Evidence-based practice “clinical practice that is informed by evidence about interventions, clinical expertise, and patient needs, values, and preferences and their integration in decision making about individual care” (Kazdin, 2008) When it comes to anxiety disorders it really is time to mvoe from ebt that have produced t.c. in a controlled trial to e.b.p.
 Evidence-based practice. clinical practice that is informed by evidence about interventions, clinical expertise, and patient needs, values, and preferences and their integration in decision making about individual care (Kazdin, 2008) When it comes to anxiety disorders it really is time to mvoe from ebt that have produced t.c. in a controlled trial to e.b.p.")
20
Protocol-based treatment
Strong trend over the last 25 years toward the development of standardized, protocol-based treatments (i.e., treatment manuals) Protocol characteristics: Disorder specific Step-by-step list of interventions Same set of procedures across clients Dissemination and training is generally needed for each protocol MAYBE GET A PICTURE OF ALL THE MANUALS
 Protocol characteristics: Disorder specific. Step-by-step list of interventions. Same set of procedures across clients. Dissemination and training is generally needed for each protocol. MAYBE GET A PICTURE OF ALL THE MANUALS.")
21
Pros and cons Pros Significant advances in the scientific study of psychotherapy (treatments are replicable) Improved treatment outcomes Greater consistency and quality of care Cons Problems with dissemination Overlap and redundancy across protocols Multiple protocols for the same disorder Don’t address co-morbidity Decreased flexibility in treatment Encourage disorder-specific thinking

22
Modular-based treatment
Emerging trend in recent years toward more modular, flexible approaches to treatment Modular approaches provide a set of overarching principles and a set of evidence-based interventions (“modules”) Not all modules are necessarily used with each client and the order of modules may vary from client to client Decisions about which modules to use and in what order are based on the unique symptom patterns of each client
 Not all modules are necessarily used with each client and the order of modules may vary from client to client. Decisions about which modules to use and in what order are based on the unique symptom patterns of each client.")
23
Modular treatment and anxiety
Anxiety disorders lend themselves well to a modular treatment approach because… They share many of the same features and symptoms A CBT conceptualization of anxiety can be applied across the disorders There is considerable overlap in the interventions that comprise the treatment protocols for the various disorders Modular approaches have been developed for treating anxiety in children/adolescents (Chorpita, 2006) and somewhat with adults (Barlow et al., 2004; Sullivan et al., 2007)
 and somewhat with adults (Barlow et al., 2004; Sullivan et al., 2007)")
24
Basic CBT model of anxiety
Physical sensations (physiological arousal) Anxiety Thoughts (perception of threat) Behaviors (avoidance, safety behaviors)
 Anxiety. Thoughts. (perception of threat) Behaviors. (avoidance, safety behaviors)")
25
Safety behaviors Anxious people often engage in a range of behaviors to make themselves feel safer when they cannot avoid anxious situations These behaviors are attempts to neutralize feelings of anxiety Although these behaviors can facilitate functioning, they also prevent recovery Examples Reassurance seeking Over-preparation Behavioral rituals Safety cues/objects

26
Integrated CBT Model of Anxiety Disorders
Fear Stimulus (trigger or cue) Misinterpretation of Threat Pre-existing Beliefs Anxiety Environmental Factors Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 Misinterpretation. of Threat. Pre-existing. Beliefs. Anxiety. Environmental. Factors. Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
27
Components of the model
Fear stimulus/trigger Anxiety is almost always cued Misinterpretation of threat Primary cognitive distortions in anxiety (1) Overestimating the likelihood of negative outcomes (2) Catastrophizing Avoidant coping Primary avoidance – avoiding triggers altogether Secondary avoidance – engaging in safety behaviors when complete avoidance is not possible Absence of corrective learning New learning does not occur and the fear is maintained (and often strengthened) JUST PRINT THIS
 Overestimating the likelihood of negative outcomes (2) Catastrophizing. Avoidant coping. Primary avoidance – avoiding triggers altogether. Secondary avoidance – engaging in safety behaviors when complete avoidance is not possible. Absence of corrective learning. New learning does not occur and the fear is maintained (and often strengthened) JUST PRINT THIS.")
28
Separation anxiety disorder
Fear Stimulus (trigger or cue) - Separating from parent at school. - Going to a friend’s house for a sleep-over. - My mom/dad might die. - Something bad might happen to my mom/dad. Misinterpretation of Threat Anxiety - Panic symptoms, crying Primary avoidance: Refuse to leave house/car; call home to be picked up Secondary avoidance: Separates but only if can call parent repeatedly to seek reassurance that he/she is okay; has to carry cell phone at all times Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 - Separating from parent at school. - Going to a friend’s house for a sleep-over. - My mom/dad might die. - Something bad might happen to my mom/dad. Misinterpretation. of Threat. Anxiety. - Panic symptoms, crying. Primary avoidance: Refuse to leave house/car; call home to be picked up. Secondary avoidance: Separates but only if can. call parent repeatedly to seek reassurance that. he/she is okay; has to carry cell phone at all times. Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
29
Specific phobia (flying)
Fear Stimulus (trigger or cue) Needing to fly for a business trip. Needing to fly for a family vacation. Something will go wrong with the plane. The plan will crash and I will die. Misinterpretation of Threat Anxiety - Increased heart rate, shallow breathing Primary avoidance: Avoid going on the trip; get someone else to attend the business meeting; family drives to vacation spot instead of flying Secondary avoidance: Sit next to “safe” person; distract self for entire flight; seek reassurance from others about airline safety; drink alcohol or take Xanax before/during the flight (adults) Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 Needing to fly for a business trip. Needing to fly for a family vacation. Something will go wrong with the plane. The plan will crash and I will die. Misinterpretation. of Threat. Anxiety. - Increased heart rate, shallow breathing. Primary avoidance: Avoid going on the trip; get. someone else to attend the business meeting; family drives to vacation spot instead of flying. Secondary avoidance: Sit next to safe person; distract self for entire flight; seek reassurance. from others about airline safety; drink alcohol or. take Xanax before/during the flight (adults) Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
30
(primary and secondary) Experience and Learning
Social phobia Fear Stimulus (trigger or cue) Having to give a presentation in front of the class. - Needing to ask a question in a store. I will sound stupid. My mind will go blank. I will be an inconvenience. He will be annoyed. Misinterpretation of Threat Anxiety - Increased heart rate, sweating, lightheaded Primary avoidance: Skip class; avoid asking the question Secondary avoidance: Look down at notes during the entire presentation; talk quickly; over-prepare for presentation; overly apologetic when asking Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 Having to give a presentation in front of the class. - Needing to ask a question in a store. I will sound stupid. My mind will go blank. I will be an inconvenience. He will be annoyed. Misinterpretation. of Threat. Anxiety. - Increased heart rate, sweating, lightheaded. Primary avoidance: Skip class; avoid asking the. question. Secondary avoidance: Look down at notes during. the entire presentation; talk quickly; over-prepare. for presentation; overly apologetic when asking. Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
31
(primary and secondary) Experience and Learning
Panic disorder Fear Stimulus (trigger or cue) Exercising and heart rate starts to increase. I am going to have a heart attack. I am going to pass out. Misinterpretation of Threat Panic symptoms (increased heart rate, shallow breathing, sweating, dizziness) Anxiety Primary avoidance: Stop exercising; leave the gym Secondary avoidance: Repeatedly check heart rate; call doctor office; go to urgent care center; seek reassurance from friend; carry water and cell phone at all times at gym Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 Exercising and heart rate starts to increase. I am going to have a heart attack. I am going to pass out. Misinterpretation. of Threat. Panic symptoms (increased heart rate, shallow. breathing, sweating, dizziness) Anxiety. Primary avoidance: Stop exercising; leave the gym. Secondary avoidance: Repeatedly check heart. rate; call doctor office; go to urgent care center; seek reassurance from friend; carry water and cell. phone at all times at gym. Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
32
(primary and secondary) Experience and Learning
GAD Fear Stimulus (trigger or cue) Trying to call spouse and he/she is not answering. Something must have happened. He/she was in an accident. Misinterpretation of Threat Restlessness, muscle tension, increased heart rate Anxiety Primary avoidance: N/A Secondary avoidance: Repeatedly calling spouse at multiple numbers (work, cell phone) until reaching him/her; keep busy and try to distract self until spouse is home Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 Trying to call spouse and he/she is not answering. Something must have happened. He/she was in an accident. Misinterpretation. of Threat. Restlessness, muscle tension, increased heart. rate. Anxiety. Primary avoidance: N/A. Secondary avoidance: Repeatedly calling spouse. at multiple numbers (work, cell phone) until. reaching him/her; keep busy and try to distract self. until spouse is home. Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
33
(primary and secondary) Experience and Learning
PTSD (sexual assault) Fear Stimulus (trigger or cue) Walking home from bus stop after work at dusk. I am not safe. - Someone could assault/rape me on the way home. Misinterpretation of Threat Increased heart rate, shallow breathing, upset stomach Anxiety Primary avoidance: Avoid taking the bus; drive to and from work; call someone for a ride Secondary avoidance: Have someone walk with him/her between bus stop and home; talk on cell phone during entire walk home; walk quickly; carry pepper spray in hand during walk Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 Fear Stimulus. (trigger or cue) Walking home from bus stop after work at dusk. I am not safe. - Someone could assault/rape me on the way home. Misinterpretation. of Threat. Increased heart rate, shallow breathing, upset stomach. Anxiety. Primary avoidance: Avoid taking the bus; drive to. and from work; call someone for a ride. Secondary avoidance: Have someone walk with. him/her between bus stop and home; talk on cell. phone during entire walk home; walk quickly; carry. pepper spray in hand during walk. Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
34
(primary and secondary) Experience and Learning
OCD (checking) Fear Stimulus (trigger or cue) Turning off the stove after cooking breakfast. What if I left the stove on? It could burn down the house. Misinterpretation of Threat Increased heart rate Anxiety Primary avoidance: Avoid eating breakfast foods that require using the stove Secondary avoidance: Repeatedly check the stove before leaving the house; drive back home mid- day from work to check the stove; call neighbor to check on the house; mentally review memory of turning off the stove throughout the day Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 Fear Stimulus. (trigger or cue) Turning off the stove after cooking breakfast. What if I left the stove on It could burn down the house. Misinterpretation. of Threat. Increased heart rate. Anxiety. Primary avoidance: Avoid eating breakfast foods. that require using the stove. Secondary avoidance: Repeatedly check the stove. before leaving the house; drive back home mid- day from work to check the stove; call neighbor to. check on the house; mentally review memory of. turning off the stove throughout the day. Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
35
Shared processes to target
There are a set of anxiety processes that are important to target regardless of which anxiety disorder is being treated Maladaptive thoughts that contribute to perceptions of threat in safe situations Physiological reactivity in response to fear triggers Avoidance behaviors that prevent the habituation of fear Safety behaviors that prevent new learning Problematic reinforcement of anxiety by the environment

36
Good news… We have very effective CBT interventions for the processes common to the anxiety disorders! Process/problem Intervention Misperception of threat Cognitive restructuring Physiological reactivity Relaxation skills Avoidance behaviors Exposure** Safety behaviors Response prevention Reinforcement of anxiety by environment Contingency management

37
Modular treatment for anxiety
A modular CBT approach to treating anxiety involves… Assessing which anxiety processes are most prominent for each client Selecting the evidence-based interventions (“modules”) that are effective for treating these processes Sequencing these modules to address the unique characteristics of each client and his/her environment
 that are effective for treating these processes. Sequencing these modules to address the unique characteristics of each client and his/her environment.")
38
CBT “modules” for anxiety
Psychoeducation Self-monitoring Relaxation skills Cognitive restructuring Response prevention Exposure* Parenting techniques Changing environmental contingencies/responses Relapse prevention Others: social skills, emotion regulation, behavioral activation, motivational interviewing…. Flexible modules HERE OR RIGHT BEFORE THIS SLIDE COULD SHOW THE CHORPITA SLIDES IN OTHER TALK AS EXAMPLES OF WHAT A MORE FULLY FLESHED OUT MODULAR TREATMENT WOULD LOOK LIKE. THEN MAYBE MOVE TO ADULT LITERATURE BEING A BIT LESS FULLY FLESHED OUT WHEN IT COMES TO INTERWEAVING OF COMPLEX ISSUES THAT OFTEN CO-OCCUR LIKE SUBSTANCE USE, PAIN, ETC. ESP. IN SETTINGS LIKE PRIMARY CARE. BUT, THESE ARE THE BASIC ISSUES, ETC. ETC.

39
Flowchart for a standard manualized CBT protocol
Fear Ladder Learning about Anxiety Relaxation Cognitive Restructuring Exposure Rewards / Practice Maintenance Finish

40
Modular CBT protocol – (Just get to Exposure)
Fear Ladder Interference Learning about Anxiety child ready to practice? no yes in vivo possible? yes no yes In Vivo Exposure Imaginal Exposure more items to practice? Maintenancee Finish no

41
Modular flowchart for treatment planning
Fear Ladder moderate disruptive behavior? parents rewarding avoidance? low motivation? other mild disruptive Behavior? negative beliefs or depression? social skills deficits? troubleshoot Learning about Anxiety Rewards Time-Out Social Skills: Meeting People bright, verbal, or older? yes child ready to practice? Active Ignoring no Cognitive Restructuring: Probability Social Skills: Nonverbal no yes in vivo possible? Cognitive Restructuring: STOP Cognitive Restructuring: Catastrophic yes no yes In Vivo Exposure Imaginal Exposure more items to practice? Maintenance Finish no

42
Modular flowchart for treatment planning
Fear Ladder moderate disruptive behavior? parents rewarding avoidance? slow motivation? other mild disruptive Behavior? negative beliefs or depression? social skills deficits? troubleshoot Learning about Anxiety Rewards Time-Out Social Skills: Meeting People bright, verbal, or older? yes child ready to practice? Active Ignoring no Cognitive Restructuring: Probability Social Skills: Nonverbal no yes in vivo possible? Cognitive Restructuring: STOP Cognitive Restructuring: Catastrophic yes no yes In Vivo Exposure Imaginal Exposure more items to practice? Maintenance Finish no

43
CBT “modules” for anxiety
Psychoeducation Self-monitoring Relaxation skills Cognitive restructuring Response prevention Exposure* Parenting techniques Changing environmental contingencies/responses Relapse prevention Others: social skills, emotion regulation, behavioral activation, motivational interviewing…. Flexible modules HERE OR RIGHT BEFORE THIS SLIDE COULD SHOW THE CHORPITA SLIDES IN OTHER TALK AS EXAMPLES OF WHAT A MORE FULLY FLESHED OUT MODULAR TREATMENT WOULD LOOK LIKE. THEN MAYBE MOVE TO ADULT LITERATURE BEING A BIT LESS FULLY FLESHED OUT WHEN IT COMES TO INTERWEAVING OF COMPLEX ISSUES THAT OFTEN CO-OCCUR LIKE SUBSTANCE USE, PAIN, ETC. ESP. IN SETTINGS LIKE PRIMARY CARE. BUT, THESE ARE THE BASIC ISSUES, ETC. ETC.

44
Psychoeducation Key to helping clients understand their symptoms and the treatment model Psychoeducation should include both: Disorder specific information Review of the integrated CBT model of anxiety Helpful to fill out the model with the client using examples from his/her life Kids- maps, posters, etc. Could be used for anxiety disorder or “normal” anxiety (will be validating if not anxiety reducing) Could be used for parents dealing with anxiety, even without anxiety disorder
 Could be used for parents dealing with anxiety, even without anxiety disorder.")
45
Integrated Model of Anxiety -
Client Handout Fear Stimulus (trigger or cue) Misinterpretation of Threat Pre-existing Beliefs Anxiety Environmental Factors Avoidant Coping (primary and secondary) Absence of Corrective Experience and Learning
 Misinterpretation. of Threat. Pre-existing. Beliefs. Anxiety. Environmental. Factors. Avoidant Coping. (primary and secondary) Absence of Corrective. Experience and Learning.")
46
Self-monitoring Critical part of problem/ symptom assessment
Helps client recognize the different components of their anxious reactions (“anxiety is not a lump”) Helps clients identify patterns in responses Elements of self-monitoring for anxiety include: Triggers/cues for anxiety Intensity ratings for anxiety (SUDS) Physical sensations Anxious thoughts Anxious behaviors (avoidance, safety behaviors) Young kids would do with caretaker
 Helps clients identify patterns in responses. Elements of self-monitoring for anxiety include: Triggers/cues for anxiety. Intensity ratings for anxiety (SUDS) Physical sensations. Anxious thoughts. Anxious behaviors (avoidance, safety behaviors) Young kids would do with caretaker.")
47
Self-monitoring example – social phobia
Situation/trigger Boss asked me a question in a meeting Intensity of anxiety (0-10) 5 Physical sensations/ other symptoms Sweating, lightheaded, upset stomach Anxious thoughts (words or images) “I am going to freeze up,” “I will sound like an idiot” Anxious behaviors (e.g., avoidance, safety behaviors, rituals) Gave a short answer; avoided eye contact; took a drink of water; mental retracing after
 5. Physical sensations/ other symptoms. Sweating, lightheaded, upset stomach. Anxious thoughts. (words or images) I am going to freeze up, I will sound like an idiot Anxious behaviors. (e.g., avoidance, safety behaviors, rituals) Gave a short answer; avoided eye contact; took a drink of water; mental retracing after.")
48
Self-monitoring example - panic
Situation/trigger Standing in line at a store Intensity of anxiety (0-10) 7 Physical sensations/ other symptoms Increased heart rate, shallow breathing, sweating Anxious thoughts (words or images) “I am going to have a panic attack,” “I won’t be able to get out of here in time” Anxious behaviors (e.g., avoidance, safety behaviors, rituals) Put my merchandise down and left the store; went to sit on a bench to calm down; took a Xanax MAYBE ADD A COMMENT ABOUT HOW IF YOU DO SELF-MONITORING ALL THE TIME
 7. Physical sensations/ other symptoms. Increased heart rate, shallow breathing, sweating. Anxious thoughts. (words or images) I am going to have a panic attack, I won’t be able to get out of here in time Anxious behaviors. (e.g., avoidance, safety behaviors, rituals) Put my merchandise down and left the store; went to sit on a bench to calm down; took a Xanax. MAYBE ADD A COMMENT ABOUT HOW IF YOU DO SELF-MONITORING ALL THE TIME.")
49
Self-monitoring example - OCD
Situation/trigger Hitting a bump in the road while driving Intensity of anxiety (0-10) 9 Physical sensations/ other symptoms Increased heart rate Anxious thoughts (words or images) “What if I hit someone with my car?” Anxious behaviors (e.g., avoidance, safety behaviors, rituals) Drove around the block 4 times to check for injured pedestrians; mental retracing
 9. Physical sensations/ other symptoms. Increased heart rate. Anxious thoughts. (words or images) What if I hit someone with my car Anxious behaviors. (e.g., avoidance, safety behaviors, rituals) Drove around the block 4 times to check for injured pedestrians; mental retracing.")
50
Relaxation Relaxation skills target physiological reactivity associated with anxiety and worry Two main skills are Diaphragmatic breathing – targets acute panic/anxiety reactions Progressive muscle relaxation – targets chronic muscle tension associated with ongoing anxiety/worry Important to be realistic about how effective these skills are in reducing anxiety Could be taught for anxiety disorder or “normal” anxiety Creative ways to teach children (bubbles, snake, tire)
")
51
Relaxation Disorder specific recommendations General recommendations
Breathing re-training is a standard part of treatment for panic disorder PMR is a standard part of treatment for GAD Neither tends to work that well for OCD General recommendations Consider using with children and adolescents regardless of disorder Consider using with adults regardless of disorder when physiological symptoms are prominent and/or interfere with treatment Coach clients not to use relaxation skills during exposure exercises

52
(assuming that fear is not really dangerous)
Exposure Exposure is staying present with the feared stimulus long enough for new learning to occur (assuming that fear is not really dangerous)
")
53
Habituation and anxiety
Time

54
Exposure Three golden rules of exposure:
1. Fears are faced gradually, moving from least to most difficult 2. The client must stay in the feared situation long enough to learn that the bad things s/he fears will not happen. If withdrawal occurs to quickly-fear can increase 3. Practice and repetition are the keys to success

55
Exposure Process of exposure is similar across the anxiety disorders, what varies is the fear trigger Separation anxiety – separation from caregiver Specific phobia – feared object/ situation Social phobia – social/performance situations Panic/agoraphobia – physical sensations of panic/avoided activities and situations GAD – worry scenarios/images and worry triggers PTSD – trauma memories and triggers OCD – triggers for obsessions and obsessive thoughts themselves

56
Exposure: Build a Hierarchy
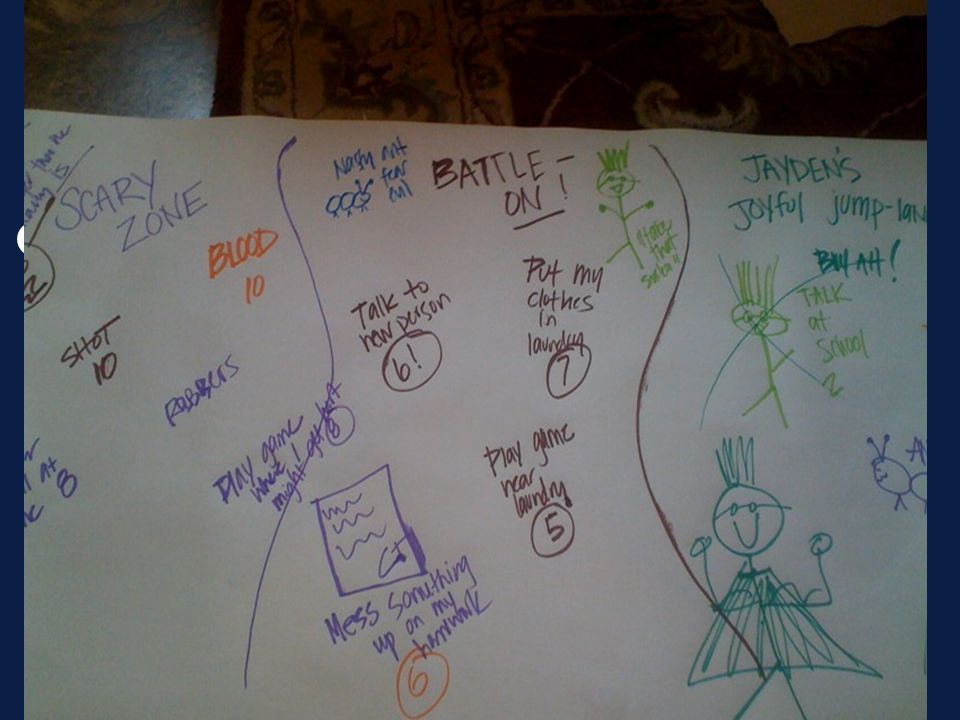
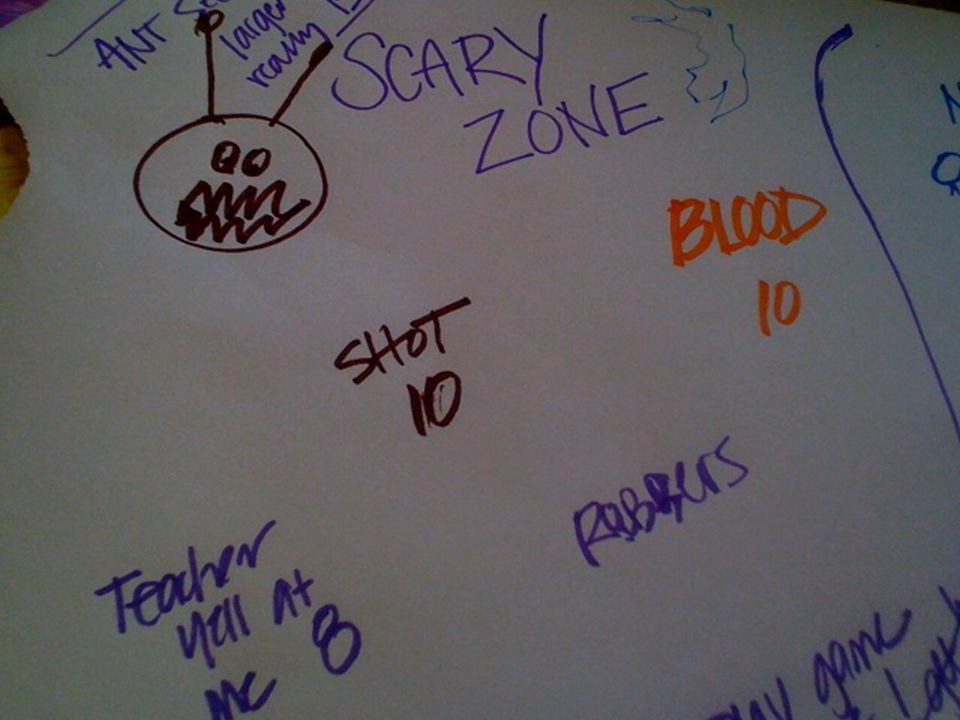
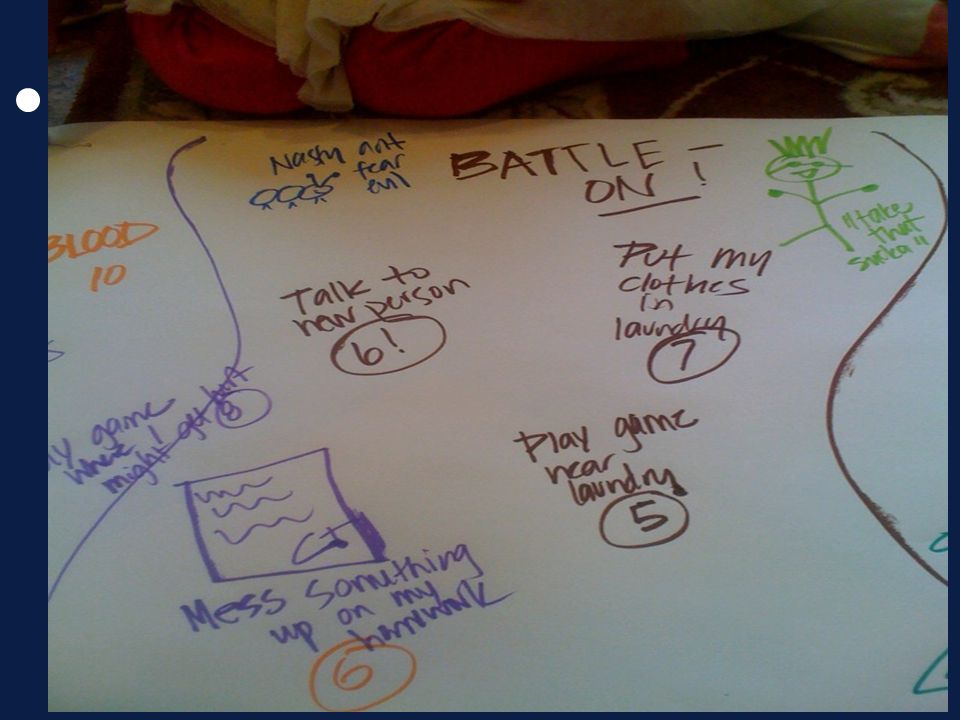
First, externalize anxiety Teach children how to identify and rate anxiety Fear thermometer / worry scale Anxiety list, “bravery ladder”, map Case example: “Jayden”, 9 year old boy with GAD, mild OCD Very significant worries in a wide range of areas – academic, medical, social, getting hurt, making any mistake Adopted at age 4 out of foster care system, very early abuse/neglect Significant risk and protective factors

58
Example: Jayden, GAD Situation Worry Scale High Getting a shot
Teacher yelling at me Making mistakes on tests Falling and getting hurt at school Forgetting my homework Seeing blood Thinking about robbers Getting a bad grade Going to a new place 10 9 8 Medium Being late for school Forgetting a library book Making a mistake on homework Meeting new people Laundry machine 7 5 Low Chatting at school Playdates 4 3

63
Exposure hierarchy example – separation anxiety
SUDs Trigger 10 Going to an overnight camp 9 Spending the night at a friend’s house 8 Staying with grandma – both parents out of town overnight 7 One parent out of town overnight 5 2 hour play-date (no parents present) 3 1 hour play date (no parents present) 1 Playing alone in room (parents outside in yard)
 3. 1 hour play date (no parents present) 1. Playing alone in room (parents outside in yard)")
64
Exposure hierarchy example – PTSD (car accident)
SUDs Trigger 10 Driving on freeway where accident happened 8 Talking about the memory of the accident 7 Watching a car accident in a movie/TV show 5 Driving on a busy road at rush hour 4 Driving on a busy road not at rush hour 3 Driving in a busy parking lot 2 Driving around the block 1 Sitting in driver’s seat of car in driveway

65
Exposure hierarchy example – GAD
SUDs Trigger 10 Imagining spouse dying in car accident 9 Reading article about cancer 8 Imagining being fired from job 6 Imagining son failing out of college 5 Watching evening news Imagining being poor in retirement 4 Reading article about bankruptcy 3 Making a decision and not reversing it

66
Exposure hierarchy example – panic (interoceptive exposure)
SUDs Trigger 10 Running in place for 5 minutes (heart rate) 9 Spinning in chair for 1 minute (dizziness) 7 Straw breathing for 1 minute (not enough air) 6 Over-breathing for 1 minute (hyperventilating) 5 Walking up 1 flight of stairs (heart rate) 4 Sitting in heated car for 3 minutes (heat) 3 Standing up quickly (dizziness)
 9. Spinning in chair for 1 minute (dizziness) 7. Straw breathing for 1 minute (not enough air) 6. Over-breathing for 1 minute (hyperventilating) 5. Walking up 1 flight of stairs (heart rate) 4. Sitting in heated car for 3 minutes (heat) 3. Standing up quickly (dizziness)")
67
Tips when doing Exposure
If in doubt, start low Conduct first exposure in session, if possible Research on therapist – assisted exposure in OCD Schedule adequate time Prep and orient, but don’t drag out Be aware of your style Confident Lots of praise esp. following exposure Coach Balance distraction/coping with focus on anxiety sensations Debrief afterwards to promote learning

68
Case Example Case example – Jayden
Taught breathing and relaxation to entire family Started exposure with a low anxiety / high probability of success item (talking to a new person at our office), then extended to saying hello to baristas at coffee shops , then moved to saying hello to more people at school Gradually reduced reassurance seeking (cut by 50% as directed by child, with reward system). Worked with Mom to decrease overprotective behaviors and increase reinforcement for “brave” behaviors
, then extended to saying hello to baristas at coffee shops , then moved to saying hello to more people at school. Gradually reduced reassurance seeking (cut by 50% as directed by child, with reward system). Worked with Mom to decrease overprotective behaviors and increase reinforcement for brave behaviors.")
69
Exposure, cont. Eventually did “silly” things (say hi in a foreign language, wear our shirts inside out downtown) Moved up hierarchy with parents gradually coaching more at home during exposures (e.g., laundry). Laundry: play reward game near laundry, then sitting on machine, then put clothes in laundry, then imagine being sucked in laundry with therapist
. Laundry: play reward game near laundry, then sitting on machine, then put clothes in laundry, then imagine being sucked in laundry with therapist.")
71
What about traumatized kids / “normal” anxiety?
Exposure to actual danger makes fear increase Exposure when situation is not dangerous will create decreased fear over time Consider adding safety cues to help lower anxiety level Talk it through, focus their attention externally, validate fear Add safety cues (reassurance, praise) If needed use distraction If anxiety can’t be tolerated – avoid and try to come back later Examples: Dentist / therapy dog Little Bear – “the clam”
 If needed use distraction. If anxiety can’t be tolerated – avoid and try to come back later. Examples: Dentist / therapy dog. Little Bear – the clam")
72
Cognitive restructuring
Clients learn to: Identity anxious thoughts Evaluate / challenge unhelpful or maladaptive thoughts Generate more balanced, accurate thoughts Coping thoughts must be believable and not just “positive thinking” Rehearsal Before anxious situations During anxious situations With practice, balanced thoughts come more automatically

73
Cognitive distortions in anxiety
General Overestimating the likelihood of negative outcomes (“jumping to conclusions”) Catastrophizing (“worst case”)
 Catastrophizing ( worst case )")
74
Cognitive restructuring strategies
Overestimating likelihood of negative outcomes: Identify all other possible outcomes to help determine the “real odds” of the feared outcome Catastrophizing: Generate a list of ways to cope with the worst case scenario

75
Cognitive restructuring
Tread carefully and use validation Think developmentally Focus on helpfulness vs. accuracy If thoughts are resistant to change, back off and try again in another way or at another time

76
Cognitive restructuring example – separation anxiety
Anxious thought: If my mom goes to work (at a college campus) she will get shot and killed. Cognitive restructuring: Evidence for: There have been several shootings at colleges recently Evidence against: There has never been a shooting at her campus; she has been to work hundreds of time and has always come home safely; she’s never been injured at work at all Coping thoughts: My mom will likely be okay at work. Her campus seems to be pretty safe.
 she will get shot and killed. Cognitive restructuring: Evidence for: There have been several shootings at colleges recently. Evidence against: There has never been a shooting at her campus; she has been to work hundreds of time and has always come home safely; she’s never been injured at work at all. Coping thoughts: My mom will likely be okay at work. Her campus seems to be pretty safe.")
77
Cognitive restructuring example – social anxiety
Anxious thought: If I go to happy hour with my co-workers I won’t be able to come up with anything to say and I will look weird. Cognitive restructuring: Other possible outcomes: I am able to say something; I listen to others and just ask questions; I sit quietly and nobody notices; other people are quiet too. Real odds: Low. Coping with worst case: I could excuse myself to the bathroom and try to think of some things to talk about; I could think of ideas now before I go Coping thoughts: I will probably feel anxious but I can come up with at least 1 thing to say. I am not responsible for 100% of the conversation.

78
Cognitive restructuring example – panic
Anxious thought: I feel lightheaded. I am going to pass out and make a scene. Cognitive restructuring: Other possible outcomes: I might not faint – I never have before; I feel lightheaded because I am anxious; the feeling will probably pass after a while. Real odds: Low. Coping with worst case: If I fainted other people around would probably help me; I would feel embarrassed but that would pass too – I could tell people that I have a medical condition Coping thoughts: I been lightheaded many times and have never fainted. I am not likely to faint but if I do other people will help me and I won’t feel embarrassed forever. You don’t die from fainting!

79
A caveat about OCD Cognitive restructuring can be problematic when treating OCD Core feature of OCD is a difficulty tolerating doubt and uncertainty Cognitive restructuring can play right into this difficulty and often does not “stick” due to lingering doubts Can use the strategies to focus on beliefs about thoughts vs. the content of the thoughts themselves

80
Cognitive restructuring example - OCD
Anxious thought: If I have a bad thought something bad will happen to someone I love (example of thought action fusion) Cognitive restructuring: Socratic questioning about whether thoughts can impact events in the world Behavioral experiments to test this out – think about something falling from the sky and see if it does; think about a bug dying and see if it dies; work up to more difficult experiments about others being harmed by client’s thoughts
 Cognitive restructuring: Socratic questioning about whether thoughts can impact events in the world. Behavioral experiments to test this out – think about something falling from the sky and see if it does; think about a bug dying and see if it dies; work up to more difficult experiments about others being harmed by client’s thoughts.")
81
Response prevention Drawn from OCD treatment, but can be used broadly across anxiety disorders Response prevention can be thought of as the process of blocking any behaviors that are an attempt to neutralize anxiety (i.e., safety behaviors) Exposure less effective without RP, so its good to start before starting exposure if possible Often overlooked
 Exposure less effective without RP, so its good to start before starting exposure if possible. Often overlooked.")
82
Response prevention - steps
Identify safety behaviors Develop a plan to reduce and eliminate them (this can be put on your exposure hierarchy) Goal is to work toward full response prevention whenever possible (i.e., elimination of all safety behaviors) For severe anxiety, esp. health anxiety or OCD, might have to start with response prevention
 Goal is to work toward full response prevention whenever possible (i.e., elimination of all safety behaviors) For severe anxiety, esp. health anxiety or OCD, might have to start with response prevention.")
83
Response prevention example – driving phobia
Safety behavior Response prevention plan Listen to talk radio as a distraction Lower volume of radio over time until radio is off altogether Carry full bottle of water in front seat of car whenever driving Switch to half empty bottle, then mostly empty bottle, and then no bottle Always drive in the slow lane on freeway Switch from slow lane to center lane and then to fast lane

84
Response prevention example – OCD (child)
Ritual/compulsion Response prevention plan 30 minute checking sequence before bed Decrease checking in steps, eliminating 1 or more components each week Change clothes after coming in from outside Decrease number of articles of clothing being changed in steps Confess to others when done something “bad” Decrease total number of confessions for the day in steps

85
Response prevention example – GAD
Safety behavior Response prevention plan Call spouse repeatedly until reach him/her Call once and then do not call again if don’t reach him/her Check stock market updates online 15 times per day Check stock market information once per day Weigh pros and cons for lengthy period of time before making a minor decision Make minor decisions within specified time frame (e.g., a few minutes) and don’t undo them
 and don’t undo them.")
86
Changing environmental contingencies/responses
Assess carefully for: Reinforcement of anxious behaviors Lack of reinforcement for non-anxious behaviors Key people in client’s life should be involved in treatment during this module (if not already) Important to keep client in driver’s seat as much as possible
 Important to keep client in driver’s seat as much as possible.")
87
Changing the environment – child client (OCD)
Problem: Anxious child with OCD whose parents participate in many of the child’s rituals to help decrease her anxiety Solution: Educate the parents about the role that their behaviors play in perpetuating the child’s anxiety Provide a clear rationale for why these behaviors need to change for the child to get better Teach parents how to reinforce non-anxious behaviors Provide a road map for when parents should stop participating in various rituals Assist parents as needed in tolerating their own anxiety about their child’s discomfort

88
Changing the environment – adult client (panic/agoraphobia)
Problem: Anxious adult with panic disorder and agoraphobia who cannot go out in public without spouse (i.e., the spouse is a primary safety cue) Solution: Educate the spouse about the role that his/her behaviors play in perpetuating the client’s anxiety Provide a clear rationale for why these behaviors need to change for the client to get better Provide a road map for when the spouse should stop going various places with the client Teach spouse how to reinforce non-anxious behaviors Assist the couple in adjusting to new roles as the client becomes more independent
 Solution: Educate the spouse about the role that his/her behaviors play in perpetuating the client’s anxiety. Provide a clear rationale for why these behaviors need to change for the client to get better. Provide a road map for when the spouse should stop going various places with the client. Teach spouse how to reinforce non-anxious behaviors. Assist the couple in adjusting to new roles as the client becomes more independent.")
89
Relapse prevention Important to develop a relapse prevention plan with all clients prior to ending treatment Typical elements of this plan include: List of possible triggers that could lead to relapse of anxiety or other symptoms Plan for how to use skills learned in treatment to cope with these triggers Plan for how to identify and respond to new triggers and/or symptoms List of supports to enlist for help as needed Guidelines for when to return for booster sessions or a new course of treatment

90
Summary Modular treatment approaches use evidence based principles and interventions in a flexible way that allows for individualized treatment planning Approaching the treatment of anxiety in a modular way can highlight the commonalities among these disorders and how they are treated Focus is on doing what is likely to work for the unique symptom presentation of each client, within a framework of evidence-based practice If you know one CBT treatment for anxiety well, a lot of your knowledge will transfer to treating other anxiety disorders!

Similar presentations









 What is it? Extremely worried about things like health, money, family/friend problems even when.>")





 Thorbjorg Sveinsdottir MSc Psychology Barnahus 31. mai.>")






