Download presentation
Presentation is loading. Please wait.

2
Clinical Enzymology

3
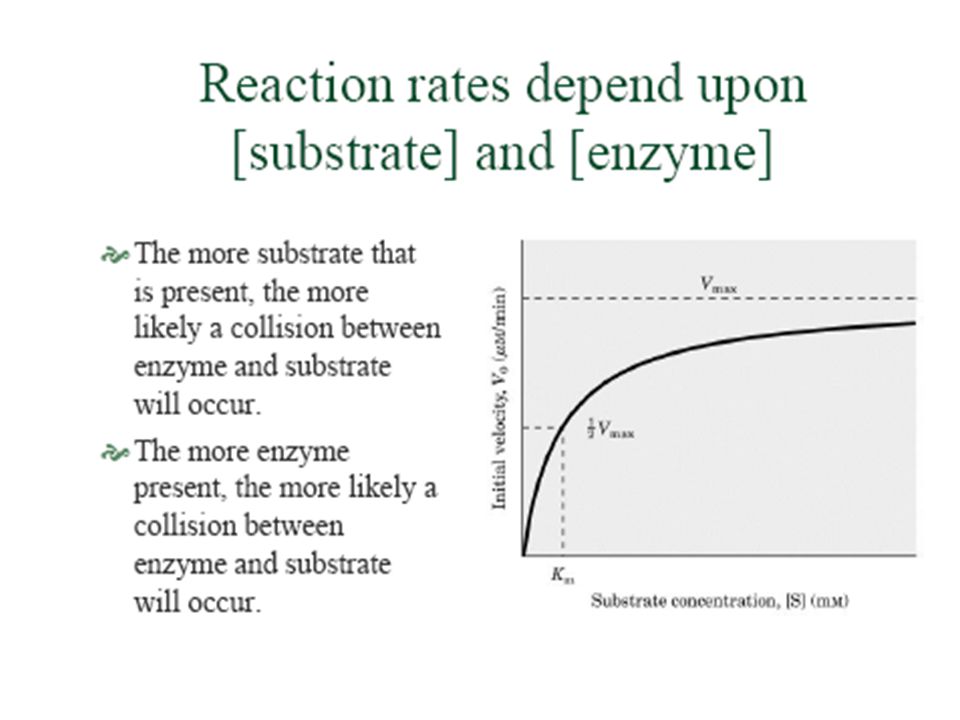
INTRODUCTION Enzymes are the protein catalysts that increase the rate of specific chemical reaction in the body. Enzymes are found in small amounts mainly within cells ,clotting factors and digestive enzymes function naturally after secretion: Plasma specific – Thrombin Secreted - Lipase, Amylase Intracellular - transaminases, creatine kinase Injury or death of tissues can cause the release of tissue-specific enzymes into the bloodstream. Elevated enzyme levels are often indicators of tissue problems, and are used in the diagnosis of diseases. Enzyme activities in the body fluids are altered by pathological processes so, its measurement is used for disease investigation.

4
Chemical Nature of Enzymes
All known enzymes are proteins. They are high molecular weight compounds made up principally of chains of amino acids linked together by peptide bonds. Enzymes can be denatured and precipitated with salts, solvents and other reagents. They have molecular weights ranging from 10,000 to 2,000,000. Many enzymes require the presence of other compounds - cofactors - before their catalytic activity can be exerted. This entire active complex is referred to as the HOLOENZYME; i.e., APOENZYME (protein portion) plus the COFACTOR (coenzyme, prosthetic group or metal-ion-activator) .
 plus the COFACTOR (coenzyme, prosthetic group or metal-ion-activator) .")
5
Apoenzyme + Cofactor = Holoenzyme
Chemical Nature of Enzymes ……contd. Apoenzyme + Cofactor = Holoenzyme The Cofactor may be: 1 • A coenzyme - a non-protein organic substance which is dialyzable, thermostable and loosely attached to the protein part. 2 • A prosthetic group - an organic substance which is dialyzable and thermostable which is firmly attached to the protein or apoenzyme portion. 3 • A metal-ion-activator - these include K+, Fe++, Fe+++, Cu++, Co++, Zn++, Mn++, Mg++, Ca++, and Mo+++.

7
Classification of Enzymes :
Enzymes can be classified by the kind of chemical reaction catalyzed. A. Addition or removal of water : 1. Hydrolases - these include esterases, carbohydrases, nucleases, deaminases, amidases, and proteases 2. Hydrases such as fumarase, enolase, aconitase and carbonic anhydrase B. Transfer of electrons : 1. Oxidases 2. Dehydrogenases

8
Classification of Enzymes …… contd.
C. Transfer of a radical: Transglycosidases - of monosaccharides Transphosphorylases and phosphomutases - of a phosphate group Transaminases - of amino group Transmethylases - of a methyl group Transacetylases - of an acetyl group D. Splitting or forming a C-C bond: Desmolases Changing geometry or structure of a molecule 3. Isomerases E. Joining two molecules through hydrolysis of pyrophosphate bond in ATP or other tri-phosphate 1. Ligases

9
Specificity of Enzymes :
One of the properties of enzymes that makes them so important as diagnostic and research tools is the specificity they exhibit relative to the reactions they catalyze. Greater specificity is achieved in three ways: Interpreting investigations in the light of clinical features Test pattern recognition Isoenzyme determination: AST may be due to MI or Hepatitis so, it makes confusion in diagnosis to be confirmed by LDH levels. - ALP in Cholestasis & bone diseases : - Differentiated by bilirubin & transaminase levels in Cholestasis . - Confirmed by GGT in Cholestasis.

10
Specificity of Enzymes ………contd.
In general, there are four distinct types of specificity: Absolute specificity - the enzyme will catalyze only one reaction. Group specificity - the enzyme will act only on molecules that have specific functional groups, such as amino, phosphate and methyl groups. Linkage specificity - the enzyme will act on a particular type of chemical bond regardless of the rest of the molecular structure. Stereochemical specificity - the enzyme will act on a particular steric or optical isomer.

11
Factors affecting serum enzyme activity
Rate of synthesis Tissue damage Mass of enzyme Producing tissue Rate of entry into blood Inhibition Serum enzyme activity Rate of removal Inactivation Clearance

12
Factors affecting Serum enzyme activities-1
I- Rate of entry of enzymes into blood is affected by: a – Rate of synthesis of enzyme: - Biliary obstruction hepatobiliary tree enzymes - Drugs :Anticonvulsant drugs ( Phenobarbital & phenytoin) synthesis of enzymes by the hepatocytes b- Mass of enzyme producing cells as in: - alkaline phosphatase: ( in active growth , Paget’s disease. and in 3rd trimester pregnancy). - acid phosphatase ( in cancer prostate). c- Necrosis or Cell damage as in: - Hepatitis transaminases - Myocardial infarction CK - Stored blood LDH
 synthesis of enzymes by the hepatocytes. b- Mass of enzyme producing cells as in: - alkaline phosphatase: ( in active growth , Paget’s disease. and in 3rd trimester pregnancy). - acid phosphatase ( in cancer prostate). c- Necrosis or Cell damage as in: - Hepatitis transaminases. - Myocardial infarction CK. - Stored blood LDH.")
13
Factors affecting Serum enzyme activities-2
II- Enzyme inhibitors: - Little effect on enzyme values determined in the lab. - Organophosphorus poisoning irreversible inhibition of cholinesterase. III- Clearance of enzymes: - Breakdown by Proteases and removal by the reticuloendothelial system. - Renal excretion of small molecular enzymes e.g. Amylase

15
Schematic diagram showing the effect of temperature on rate of nonenzyme-catalyzed and enzyme catalyzed reactions.

16
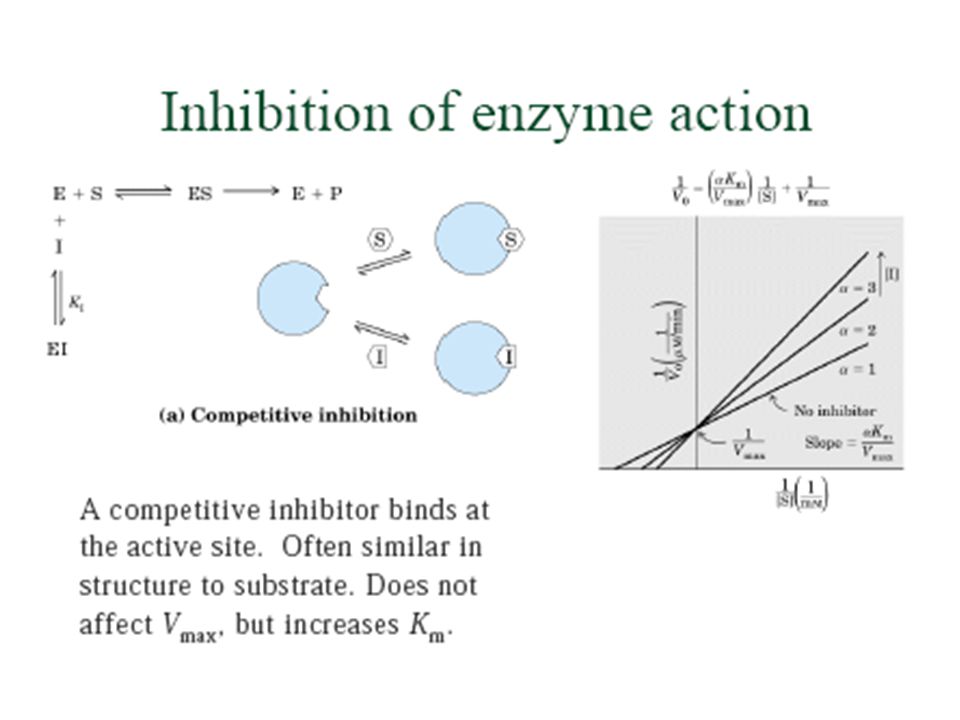
How does an enzyme work? Enzymes have an active site- a cleft into
which substrate molecules fit The active site contains amino acids that: - Attract the substrate - Assist in the chemical reactions that converts substrate to product

19
Sequence of events in enzyme catalyzed reaction
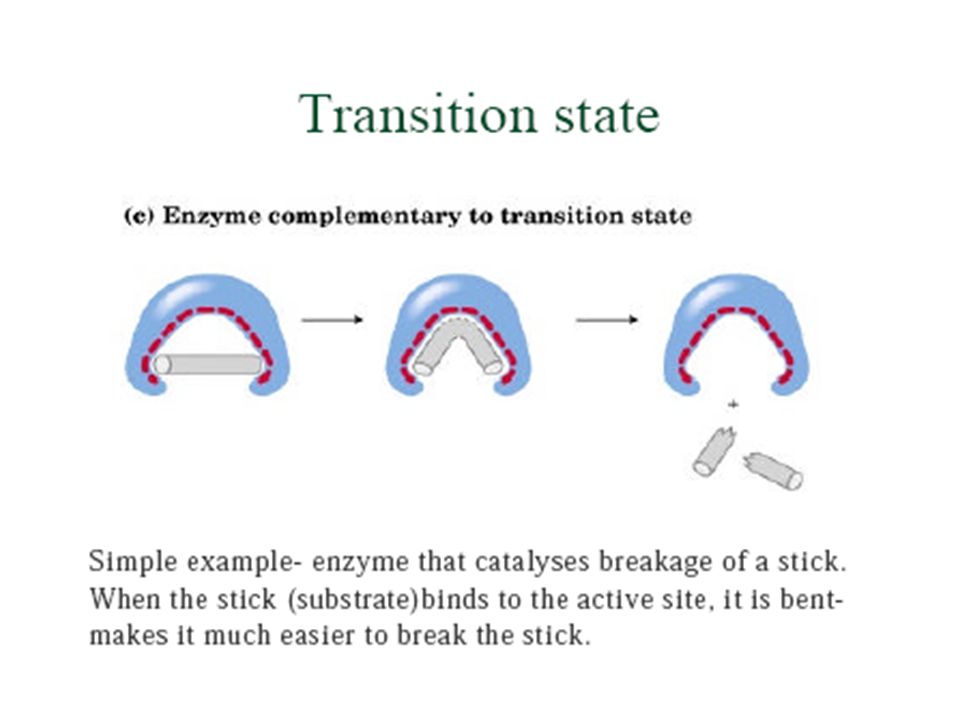
1) E + S ® ES. Enzyme and Substrate collide. Substrate binds to active site of enzyme. A transition state forms where the structure of the substrate is altered. 2) ES ® EP. Enzyme catalyses the conversion of substrate to Product. Both substrate and product remain in active site. 3) EP ® E + P. Product is released from active site.
 E + S ® ES. Enzyme and Substrate collide. Substrate binds to active site of enzyme. A transition state forms where the structure of the substrate is altered. 2) ES ® EP. Enzyme catalyses the conversion of substrate to Product. Both substrate and product remain in active site. 3) EP ® E + P. Product is released from active site.")
21
ISOENZYMES Catalyze the same reaction Two or more polypeptide chains
Different polypeptide chains are products of different genes Differ in AA sequence and physical properties May be separable on the basis of charge Are tissue specific

22
Isoenzymes and multiple forms
Aminotransferases: ALT AST GGT ALT and AST : 1. Pyridoxal dependent 2. Indicates Hepatitis, Myocardial infarction: - Elevations take > 4 hours to develop, last 4 days - ALT elevation lasts longer than AST - AST elevations are higher than ALT - Elevations occur in most definite infarctions 3. Skeletal muscle damage 4. Hemolysis 5. Pancreatitis

23
Isoenzymes and multiple forms
GGT Hepatobiliary enzyme - highly inducible in 75% of the population Highest increases in intra or posthepatic biliary obstruction Higher and more persistent increases than AlP (Alkaline Phosphatase)
")
24
Diagram illustrating the origin of Isoenzymes

25
Transaminase activities in human tissues, relative to serum as unity
AST ALT Heart 7800 450 Liver 7100 2850 Skeletal Muscle 5000 300 Kidney 4500 1200 Pancreas 1400 130 Spleen 700 80 Lung 500 45 Erythrocytes 15 7 Serum 1

26
Diagnostic Enzyme Analysis
Cellular/Plasma specific activities of various enzymes: Tissue AST ALT LDH CK (GOT) (GPT) Heart Liver <10 Skeletal Muscle RBC <1
 (GPT) Heart Liver <10. Skeletal. Muscle RBC <1.")
28
LDH-Lactate Dehydrogenase in MI
LDH is a tetramer of two non-identical subunits (LDH5(M4), LDH4(M3H), LDH3(M2H2), LDH2(MH3), LDH1(H4)
, LDH4(M3H), LDH3(M2H2), LDH2(MH3), LDH1(H4)")
29
ENZYMES OF CLINICAL INTEREST
Acid phosphatase (ACP) Amylase (AMS) Alanine aminotransferase (ALT) Alkaline phosphatase (ALP) Aspartate aminotransferase (AST) Creatine kinase (CK) Gamma-glutamyltransferase (GGT) Glucose 6-phosphate dehydrogenase (G6PD) Lactate dehydrogenase (LDH or LD) Lipase (LPS) Plasma cholinesterase
 Amylase (AMS) Alanine aminotransferase (ALT) Alkaline phosphatase (ALP) Aspartate aminotransferase (AST) Creatine kinase (CK) Gamma-glutamyltransferase (GGT) Glucose 6-phosphate dehydrogenase (G6PD) Lactate dehydrogenase (LDH or LD) Lipase (LPS) Plasma cholinesterase.")
30
Diagnostically Important Enzymes 1/3
Principle Clinical Applications Principal Sources Enzyme Carcinoma of prostate Prostate, erythrocytes Acid Phosphatase (ACP) Hepatic parenchymal disease Liver, Skeletal muscle, Heart Alanine aminotransferase(ALT) Muscle disease Skeletal muscle, heart Aldolase Bone diseases, hepatobiliary diseases Liver, bone, intestinal mucosa, placenta, kidney Alkaline Phosphatase (ALP) Pancreatic diseases Salivary glands, pancreas, ovaries Amylase (AMS) Myocardial infarction, hepatic parenchymal disease, muscle disease Liver, skeletal muscle, heart, kidney, erythrocytes Aspartate aminotransferase(AST)
 Hepatic parenchymal disease. Liver, Skeletal muscle, Heart. Alanine aminotransferase(ALT) Muscle disease. Skeletal muscle, heart. Aldolase. Bone diseases, hepatobiliary diseases. Liver, bone, intestinal mucosa, placenta, kidney. Alkaline. Phosphatase (ALP) Pancreatic diseases. Salivary glands, pancreas, ovaries. Amylase (AMS) Myocardial infarction, hepatic parenchymal disease, muscle disease. Liver, skeletal muscle, heart, kidney, erythrocytes. Aspartate aminotransferase(AST)")
31
Diagnostically Important Enzymes 2/3
Principle Clinical Applications Principal Sources Enzyme Organophosphorus insecticide poisoning, suxamethonium sensitivity, hepatic parenchymal diseases Liver Cholinesterase Myocardial infarction, muscle diseases Skeletal muscle, brain, heart, smooth muscle Creatine kinase (CK) Hepatic parenchymal disease Glutamate dehydrogenase Hepatobiliary disease, alcoholism Liver, kidney gamma-GT (GGT)
 Hepatic parenchymal disease. Glutamate dehydrogenase. Hepatobiliary disease, alcoholism. Liver, kidney. gamma-GT (GGT)")
32
Diagnostically Important Enzymes 3/3
Principle Clinical Applications Principal Sources Enzyme Myocardial infarction, hemolysis, hepatic parenchymal disease Heart, liver, skeletal muscle, erythrocytes, platelets, lymph nodes Lactate dehydrogenase(LDH) Hepatobiliary disease Hepatobiliary tract 5’ Nucleosidase Parenchymal hepatic disease Liver Sorbitol dehydrogenase Pancreatic diseases Pancreas Trypsin(ogen)
 Hepatobiliary disease. Hepatobiliary tract. 5’ Nucleosidase. Parenchymal hepatic disease. Liver. Sorbitol dehydrogenase. Pancreatic diseases. Pancreas. Trypsin(ogen)")
33
Acid phosphatase (ACP)
Found in prostate, bone, liver, spleen, kidney, RBCs and platelets Primarily used to diagnose prostate cancer . In other prostatic conditions e.g. prostatitis, benign prostatic hypertrophy. In other non prostatic conditions e.g. hemolysis, Paget’s disease, metastatic carcinoma of the breast & Gaucher’s disease. Prostate- Specific Antigen(PSA): an enzyme occurs in prostatic tissue and in cases of metastatic carcinoma Tartarate inhibits the prostatic ACP enzyme while Formaldehyde inhibits ACP from other sources
: an enzyme occurs in prostatic tissue and in cases of metastatic carcinoma. Tartarate inhibits the prostatic ACP enzyme while Formaldehyde inhibits ACP from other sources.")
34
Alanine aminotransferase (ALT)
Widely distributed, although the largest amounts found in the liver. Smaller amounts occur in the heart but usually remains normal after MI . Congestive cardiac failure release from the liver More specific for liver disease than AST.

35
Alkaline phosphatase (ALP)
Widely distributed, high concentrations in intestines, liver, bone, spleen, placenta and kidney. The main sources of serum ALP are the hepatobiliary tree and bone disorders. Elevated levels during healing of fractures , active growth and during the 3rd trimester of pregnancy. serum ALP activity in liver disease is mainly due to Cholestasis. Decreased levels are found in the inherited condition “ Hypophosphatasia” which is caused by defective bone calcification

36
Alkaline phosphatase (ALP)
Causes of increased serum alkaline phosphatase enzyme activity: Physiological : Bone disease: Hepatobiliary disease: Others: - Infancy - Puberty - Pregnancy - Intestinal isoenzymes - Hyperparathyroidism - Osteomalacia, rickets - Paget’s disease of bone - Osteomyelitis - Hepatitis - Cholestasis - Cirrhosis Carcinoma of the bronchus

37
Alkaline Phosphatase Bone Alkaline Phosphatase 4 8 12 16 20 (Years)
Males Females Alk. Phos.units (Years)
")
38
Amylase (AMS) Hydrolases that split complex Polysaccharides.
- alpha-amylases (1-4 alpha links attacked at random) - MW 40,000 - filtered by kidney - Ca+2 requiring metalloenzyme Sources : 1. Pancreas (p-type) 2. Salivary glands (s-type) 3. Intestinal malignancy
 - MW 40,000 - filtered by kidney. - Ca+2 requiring metalloenzyme. Sources : 1. Pancreas (p-type) 2. Salivary glands (s-type) 3. Intestinal malignancy")
39
Amylase (AMS) Clinical Significance : Diagnosis and monitoring of pancreatitis 1. Acute: - transient increase in activity within hours - returns to normal in days 2. Extent of increase (typically fold) related to probability of acute pancreatitis. 3. Serum amylase activity may be falsely normal in presence of severe dyslipidaemia - check urinary amylase. 4. Serum amylase may be raised in biliary duct obstruction. 5. Serum amylase activity may be normal in chronic pancreatitis. 6. Amylase may be raised in pleural effusions and pseudocystic fluids secondary to pancreatitis. 7. Salivary gland diseases or trauma may raise serum amylase activity.
 related to probability of acute pancreatitis. 3. Serum amylase activity may be falsely normal in presence of severe dyslipidaemia - check urinary amylase. 4. Serum amylase may be raised in biliary duct obstruction. 5. Serum amylase activity may be normal in chronic pancreatitis. 6. Amylase may be raised in pleural effusions and pseudocystic fluids secondary to pancreatitis. 7. Salivary gland diseases or trauma may raise serum amylase activity.")
40
Salivary Enzymes in Normal Function and Abnormal Pathology
α-Amylase—normally present in saliva—important in digestion ______________________________________________ Lysozyme Hyaluronidase Chondrosulfatase Aryl Sulfatase Neutral Protease Collagenases Specific activities are increased in gingivitis and periodontal disease

41
Causes of Hyperamylasemia and Hyperamylasuria
1. Pancreatic disease (P-type): Pancreatitis: - Acute - Chronic - Complications: Pseudocyst Ascites and pleural effusion Abcess Pancreatic Trauma, including investigative maneuvers Pancreatic carcinoma
: Pancreatitis: - Acute. - Chronic. - Complications: Pseudocyst. Ascites and pleural effusion. Abcess. Pancreatic Trauma, including investigative maneuvers. Pancreatic carcinoma.")
42
Causes of Hyperamylasemia and Hyperamylasuria
2. Disorders of non-pancreatic origin (mechanism unknown) : a- Renal insufficiency (mixed) b- Neoplastic hyperamylasemia - usually bronchogenic or ovarian (usually S-type) c- Salivary gland lesions, e.g. mumps, calculus disease (S-type) d- Macroamylasemia (predominantly S-type)
 : a- Renal insufficiency (mixed) b- Neoplastic hyperamylasemia - usually bronchogenic. or ovarian (usually S-type) c- Salivary gland lesions, e.g. mumps, calculus disease. (S-type) d- Macroamylasemia (predominantly S-type)")
43
Causes of Hyperamylasemia and Hyperamylasuria
3. Disorders of complex origin (mechanism unknown or uncertain) Biliary tract disease Intra-abdominal disease (other than pancreatic diseases): Perforated peptic ulcer (P-type) Intestinal obstruction (P-type) Mesenteric infarction (P-type) Peritonitis (mixed; depends on cause) Acute appendicitis Ruptured ectopic pregnancy (S-type) Aortic aneurysm with dissection Cerebral trauma (type depends on other organ damage) Burns and traumatic shock Postoperative hyperamylasemia (usually S-type) Diabetic ketoacidosis (mixed) Renal transplantation (S-type) Acute alcoholism (mixed) Drugs: - Medicinal opiates (P-type) - Heroin addiction (S-type)
 Biliary tract disease. Intra-abdominal disease (other than pancreatic diseases): Perforated peptic ulcer (P-type) Intestinal obstruction (P-type) Mesenteric infarction (P-type) Peritonitis (mixed; depends on cause) Acute appendicitis. Ruptured ectopic pregnancy (S-type) Aortic aneurysm with dissection. Cerebral trauma (type depends on other organ damage) Burns and traumatic shock. Postoperative hyperamylasemia (usually S-type) Diabetic ketoacidosis (mixed) Renal transplantation (S-type) Acute alcoholism (mixed) Drugs: - Medicinal opiates (P-type) - Heroin addiction (S-type)")
44
Aspartate aminotransferase (AST)
This enzyme is widely distributed in the body. Main sources: Heart, liver, skeletal muscle, and kidney. Useful in the diagnosis of MI, liver disorders and muscle damage. Causes of serum AST levels: Physiological : Neonates. Liver diseases: Hepatitis, hepatic necrosis , cholestasis Cardiac disease: Myocardial Infarction. Diseases of skeletal muscle: Crush injury,trauma,myopathy From Erythrocytes: Hemolysis

45
Creatine kinase (CK) Creatine kinase is associated with ATP regeneration in muscle and nervous tissue. Elevated blood levels of CK are used as indicators of MI, muscular dystrophy, and stroke. CK occurs as a dimer of 2 different subunits, M and B. - CK-BB: Brain type. - CK-MB: Hybrid type. - CK-MM: Muscle type. These can be separated by electrophoresis. CK-MB is released from cardiac muscle cells after MI.

46
Creatine kinase (CK) BB % MB % MM %
A dimer - M and B protein strands which are the products of different genes - true isoenzymes. 5% cutoff by general agreement 2 of 3 - history, ECG, enzymes BB % MB % MM % < 1 <20 > 80 MM - skeletal muscle > 40 > 60 MB - cardiac muscle > 95 < 3 BB - brain

47
Gamma-glutamyltransferase (GGT)
A microsomal enzyme its synthesis induced by ethanol and anticonvulsant drugs. Found mainly in the kidney and significant amounts in liver, brain, prostate, and pancreas. Used primarily for diagnosis of hepatobiliary problems. ALT, AST and GGT are the main liver function tests. Marked elevation of serum GGT level is seen in alcoholic liver disease. serum GGT activity sometimes following MI or congestive cardiac failure.

48
Glucose 6-phosphate dehydrogenase (G6PD)
First (and control) enzyme for pentose phosphate pathway (P.P.P.). Important in production of NADPH + H+, especially in RBC. NADPH + H+ keeps glutathione reduced. Antimalarial drugs are oxidants, and adversely affect this system in RBCs. Some populations, especially African-Americans, have a high frequency of G6PD deficiency. If given antimalarial drugs, or fava beans, they develop hemolytic anemia.
 enzyme for pentose phosphate pathway (P.P.P.). Important in production of NADPH + H+, especially in RBC. NADPH + H+ keeps glutathione reduced. Antimalarial drugs are oxidants, and adversely affect this system in RBCs. Some populations, especially African-Americans, have a high frequency of G6PD deficiency. If given antimalarial drugs, or fava beans, they develop hemolytic anemia.")
49
Lactate dehydrogenase (LDH or LD)
Converts pyruvate to lactate (and vice versa) during and after anaerobic metabolism. LDH occurs as a tetramer of 2 different subunits: LD-1 (HHHH) from the heart: Elevated after MI. LD-2 (HHHM) from the kidney: Elevated after renal infarction. LD-3 (HHMM) from the lung, spleen and pancreas: Elevated in pulmonary embolism. LD-4 (HMMM) and LD-5 (MMMM), both from the liver and skeletal muscle: Elevated in injury to liver or skeletal muscle.
 during and after anaerobic metabolism. LDH occurs as a tetramer of 2 different subunits: LD-1 (HHHH) from the heart: Elevated after MI. LD-2 (HHHM) from the kidney: Elevated after renal infarction. LD-3 (HHMM) from the lung, spleen and pancreas: Elevated in pulmonary embolism. LD-4 (HMMM) and LD-5 (MMMM), both from the liver and skeletal muscle: Elevated in injury to liver or skeletal muscle.")
50
Control LDH Isoenzymes

51
Lipase (LPS) Pancreatic lipases :
Breaks down fat into monoacylglycerol and free fatty acids. Primarily from the pancreas. Used to diagnose acute pancreatitis. Pancreatic lipases : - A group of enzymes that hydrolyze glycerol esters of long chain fatty acids. - Some substrate specificity e.g. LPL (Lipoprotein Lipase). - Bile salts are necessary for activity. -Almost exclusively used clinically in the investigation of pancreatitis. - Increase within hours of acute attack. - May remain elevated for many days . - More specific to acute pancreatitis than amylase. - Less sensitive to acute exacerbations in chronic pancreatitis.
. - Bile salts are necessary for activity. -Almost exclusively used clinically in the investigation of pancreatitis. - Increase within hours of acute attack. - May remain elevated for many days . - More specific to acute pancreatitis than amylase. - Less sensitive to acute exacerbations in chronic pancreatitis.")
52
Plasma cholinesterase
Similar to cholinesterase in nervous system, degrades acetylcholine (neurotransmitter and hormone). Elevated in hepatitis and cirrhosis. Also elevated in organophosphate (pesticide) poisoning. Degrades succinylcholine, a muscle relaxant given during general anesthesia in surgery. Some people are deficient in plasma cholinesterase, so the normal dose of succinylcholine would kill them Therefore, a determination of plasma cholinesterase is made prior to major surgery.
. Elevated in hepatitis and cirrhosis. Also elevated in organophosphate (pesticide) poisoning. Degrades succinylcholine, a muscle relaxant given. during general anesthesia in surgery. Some people are deficient in plasma cholinesterase, so. the normal dose of succinylcholine would kill them. Therefore, a determination of plasma cholinesterase is. made prior to major surgery.")
53
Low Plasma Cholinesterase
Examples Category of cause Infancy, 3rd Trimester of pregnancy Physiological reasons Scoline sensitivity (ChE variants) Inherited abnormality Acquired abnormality: Impaired protein synthesis A) Liver disease Organophosphorus insecticides B) Industrial poisoning Oral contraceptives, MAO inhibitors, Cytotoxic drugs C) Drug effects
 Inherited abnormality. Acquired abnormality: Impaired protein synthesis. A) Liver disease. Organophosphorus insecticides. B) Industrial poisoning. Oral contraceptives, MAO inhibitors, Cytotoxic drugs. C) Drug effects.")
54
Pancreatic Trypsin A Serine Protease (hydrolyses peptide bonds formed by the carboxyl groups of lysine/arginine). Inactive Zymogens secreted (Type 1 and 2) under the influence of vagus nerve . alpha1-antitrypsin and alpha2-macroglobulin protect serum proteins (consider alpha-1 AT deficiency). Little clinical application in modern practice.
 under the influence of vagus nerve . alpha1-antitrypsin and alpha2-macroglobulin protect serum proteins (consider alpha-1 AT deficiency). Little clinical application in modern practice.")
55
Serum Enzymes in Disease

56
Myocardial Infarction

57
Myocardial Infarction ( MI )
Necrosis of the myocardium, but not angina pectoris release of CK, AST and LDH (HBD) into the circulation. CK is the first to rise (activity within 6 h of MI ). Total CK reaches a peak at h. In uncomplicated cases, CK returns to normal within 3 days. Serum AST more slowly ( maximum activity within 48 h) and returns to normal in 4-5 days. No significant elevation in HBD seen for the 1st 24 h (reaches maximum at about 3 days & remain for up to 8 days). It is important to consider the timing of sample when interpreting test results. CK & HBD are useful as early and late indicators of MI, and more specific than AST.
 into the circulation. CK is the first to rise (activity within 6 h of MI ). Total CK reaches a peak at h. In uncomplicated cases, CK returns to normal within 3 days. Serum AST more slowly ( maximum activity within 48 h) and returns to normal in 4-5 days. No significant elevation in HBD seen for the 1st 24 h (reaches maximum at about 3 days & remain for up to 8 days). It is important to consider the timing of sample when interpreting test results. CK & HBD are useful as early and late indicators of MI, and more specific than AST.")
58
Myocardial Infarction ( MI )
CK from skeletal muscle may be following intramuscular injection, chest compression for resuscitation or electrical defibrillator. CK specificity is by measuring CK-MB. HBD activity may be due to non cardiac factors (hemolysis). Cardiac enzyme measurements are very sensitive indicators of MI because it is in over 95% of cases. They are of particular value in the following conditions: Atypical clinical presentation (absence of chest pain) If the patient presents some time after a suspected event. Difficulty in interpreting ECG (Arrhythmia or previous MI). If further MI is suspected few days of a previous one.
. Cardiac enzyme measurements are very sensitive indicators of MI because it is in over 95% of cases. They are of particular value in the following conditions: Atypical clinical presentation (absence of chest pain) If the patient presents some time after a suspected event. Difficulty in interpreting ECG (Arrhythmia or previous MI). If further MI is suspected few days of a previous one.")
59
CK-2 & CK-3 in normal subject and in patient
24 hrs after Myocardial Infarction Creatine Kinase isoenzymes in blood

60
Plasma levels following myocardial infarction
CPK---Creatine Kinase LDH---Lactate Dehydrogenase HBDH—α-Hydroxybutyrate dehydrogenase

62
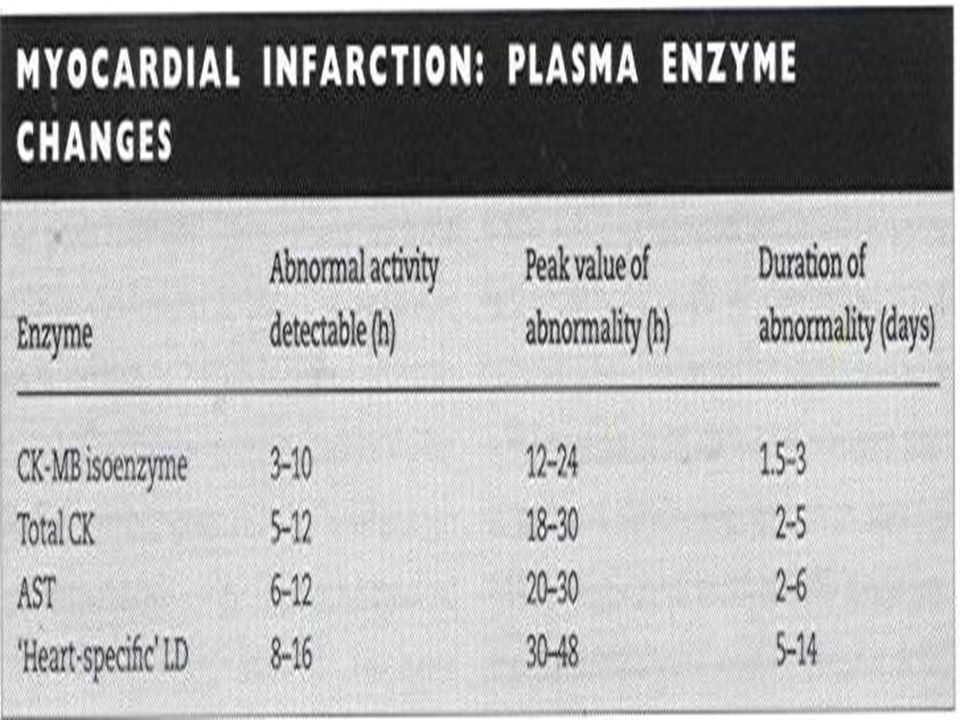
Myocardial Infarction : Plasma Enzymes Changes
Duration of abnormality (days) Peak value of abnormality(h) Abnormal activity detectable(h) Enzyme 3 - 10 CK-MB isoenzyme 2 - 5 5 - 12 Total CK 2 - 6 6 - 12 AST 5 - 14 8 - 16 Heart-specific’ LD
 Peak value of abnormality(h) Abnormal activity detectable(h) Enzyme CK-MB isoenzyme Total CK AST Heart-specific’ LD.")
63
Myocardial Infarction : Plasma enzymes vs ECG
Specificity % Sensitivity % 100 70 ECG 90 95 Plasma Enzymes

64
Troponin Troponins are a complex of I, T and C subunits uniquely present in striated muscle and regulate the calcium mediated interaction of actin and myosin. Troponin-I has three isoforms: sTnI (for fast twitch muscle); TnI (for slow twitch muscle) and cTnI (for cardiac muscle). cTnI levels are elevated in plasma within 4 hr after infarction. Better test than LDH and CKMB.
; TnI (for slow twitch muscle) and. cTnI (for cardiac muscle). cTnI levels are elevated in plasma within 4 hr after infarction. Better test than LDH and CKMB.")
65
Malignant Hyperpyrexia
Muscle Diseases Muscular Dystrophy Toxic Myopathy Malignant Hyperpyrexia Traumatic Myopathy

66
Muscular Dystrophy Genetically determined degenerative disorders.
Duchenne muscular dystrophy is an X-linked recessive disorder caused by an abnormal dystrophin gene (progressive weakness of muscles). CK activities before the onset of clinical symptoms (values >10 times the normal upper level). Serum CK is in 75 % of female carriers. Becker’s muscular dystrophy is a benign form of Duchenne MD. CK elevated pattern similar to that of Duchenne MD.
. CK activities before the onset of clinical symptoms (values >10 times the normal upper level). Serum CK is in 75 % of female carriers. Becker’s muscular dystrophy is a benign form of Duchenne MD. CK elevated pattern similar to that of Duchenne MD.")
67
Malignant Hyperpyrexia
Toxic Myopathy Causes: - Drugs & chemicals (Alcohol, D-penicillamine, ..etc) generalized myopathy - IM injections ( Trauma & Chemical irritation) CK activity by narcotic analgesics given in MI. Rapid in body temp, shock& convulsions.(in general Anesthesia Serum CK activity during attacks . Pre-operative CK should be measured in patients with a family history of malignant hyperpyrexia. Malignant Hyperpyrexia
 generalized myopathy. - IM injections ( Trauma & Chemical irritation) CK activity by narcotic analgesics given in MI. Rapid in body temp, shock& convulsions.(in general Anesthesia. Serum CK activity during attacks . Pre-operative CK should be measured in patients with a family history of malignant hyperpyrexia. Malignant Hyperpyrexia.")
68
Traumatic Myopathies Muscle trauma (surgery, I.M. injection, etc..) release of enzymes High serum CK values occurs post-operatively . If MI suspected, CK-MB should be measured. Serum CK usually return to normal within 48 h of a single intramuscular injection. Vigorous exercise of short duration and prolonged moderate exercise serum CK

69
Liver Diseases Hepatic Necrosis Hepatitis Cholestasis Jaundice
Hepatocellular Damage

70
Liver Enzymes ( ALT, AST, GGT, ALP, LDH)
Measurement of serum enzyme activities for : a - Differential Diagnosis of Jaundice. b - Monitoring of drug toxicity. ALT is more specific than AST. Hepatocellular disease has only modest effect on ALP & GGT (up to 3 times the upper limit of normal) In Cholestasis, Higher values of ALP & GGT due to synthesis ( the values are 5-10 times the upper normal level) .
 In Cholestasis, Higher values of ALP & GGT due to synthesis ( the values are 5-10 times the upper normal level) .")
71
Bone Diseases - Osteoporosis - Osteomalacia - Tumors - Paget’s Disease

72
Bone Enzymes - ( Alkaline Phosphatase) ALP
ALP enzyme is usually normal in Osteoporosis as osteoblastic activity is not increased Modest of ALP in Osteomalacia and Rickets Healing fractures Transient of ALP 1ry & 2ry Hyperparathyroidism of ALP In Paget’s disease of bone of ALP (10 times) 1ry & 2ry bone tumors of ALP (5 times normal)
 1ry & 2ry bone tumors of ALP (5 times normal)")
73
Enzymes in Urine Enzymes appear in Urine from 2 sources:
- Filtration of plasma - Leaking from cells lining the urinary tract Amylase is normally detected in urine (small size). Indicators of tubular damage: - Alkaline phosphatase - N-acetyl--glucosaminindase (NAG)
. Indicators of tubular damage: - Alkaline phosphatase. - N-acetyl--glucosaminindase (NAG)")
74
Enzymes in Hematological Disorders
Inherited or acquired diseases - Hemolytic diseases - Spherocytosis - Methemoglobinemia G-6-PD deficiency Hemolysis on exposure to oxidant drugs as antimalarial drugs (Primaquine) or ingestion of fava beans Pyruvate kinase , Glutathione synthetase, Hexokinase Defects Hemolysis
 or ingestion of fava beans. Pyruvate kinase , Glutathione synthetase, Hexokinase Defects Hemolysis.")
75
شكرًا لحسن المتابعة

76
Thank you

78
Enzymes Proteins. Increase reaction rates by lowering activation
energy. Increase rates by Allow reactions to occur under much milder conditions (low temperature, atmospheric pressure, around neutral pH). Enzymes do not affect the thermodynamic properties of a reaction- they do not alter DG.
. Enzymes do not affect the thermodynamic. properties of a reaction- they do not alter DG.")
90
Some other Enzymes of Diagnostic Value
Plasma AST in: Liver Disease Acute Renal Disease Acute Pancreatitis Alkaline Phosphatase Liver isoenzyme in: Liver cancer and fatty liver Bone isoenzyme in: Osteoblastic bone tumors Maternal plasma AP up in the third trimester of pregnancy

92
Factors affecting serum enzyme concentrations
1. Rate of entry - tissue damage enzyme synthesis - extent of tissue damage - concentration gradient - rate of production 2. Rate of clearance - breakdown by proteases - removal by reticuloendothelial system - renal excretion only for amylase (small molecular weight) 3. Induction 4. Proliferation
 3. Induction. 4. Proliferation.")
94
Functions of Released Enzymes
Components of bone—Collagen, Hyaluronic acid, Sulfated glycoproteins, Hydroxyapatite Hyaluronic Acid NAG + Glucuronic Acid HU Sulfated Glycoproteins NAG sulfate + Glucuronic AS, CS Acid Acids produced breakdown the hydroxyapatite crystal lattice

95
Bone Resorption Bone Collagen type I Abnormal Hydroxyapatite Crystal
lattice Collagenase type I ¾ and ¼ Chains Neutral Proteinase Amino acids and peptides

Similar presentations


















 are enzymes that differ in amino acid sequence but catalyze the same.>")




 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")






>")
