Download presentation
Presentation is loading. Please wait.

1
Chronic Diarrhoea in infancy

2
Admission 1 CW admitted 29/11/2010 7 week old female
Brought by mother – 18 year old 6 day history diarrhoea No vomiting, tolerating feeds Dry cough, blocked nose No traditional or other medicines taken No TB contacts

3
Birth history: Caesarean section at 43 weeks for failed induction for post-dates Birthweight - 2.8kg Mother Rh positive, RPR negative, HIV negative Feeding: Breastmilk, supplementing with Nan, Pelargon Formula incorrectly mixed – too dilute, possibly not enough given 6 week vaccine up to date. Had weighed 3.2kg at clinic Stays with mother and maternal grandparents

4
Examination Ill-looking baby Weight – 2.7kg Blood sugar 5.3mmol/l
Oxygen saturation 90% on room air Afebrile Pink Capillary refill 3 seconds, dry mucous membranes, decreased skin turgor. Fontanelle not sunken Blocked nose Chest - acidotic breathing. Chest clear CVS - normal

5
Abdomen – soft, no masses felt Excoriated nappy rash
CNS – lethargic, but moving limbs equally Blood gas – metabolic acidosis with respiratory compensation pH – 7,166 Bicarb – 5.0mmol/l PaCO₂ – 14,3mmHg BE mmol/l Assessed as 7 week old infant with gastroenteritis complicated by >10% dehydration and acidosis. Possibly also septic.

6
FBC U&E CRP CSF CMP WCC Na 2.0 P Ca corrected Hb K L Mag MCV 92 Cl RBC 3 Phos Plts Co Prot Albumin Urea Glucose 3.8 Creat 63 Cl AG No bacteria Urine dipstick Uricult Nil abnormal No growth

7
Management Intravenous fluids Cefotaxime
Zinc sulphate orally and zinc topically to nappy rash Mother continued to breastfeed and also gave Isomil

8
Progress Stools gradually settled, still quite frequent
Post-intake ward round still looked quite lethargic, grey and mottled still acidotic Skin looked dry, and as if peeling superficially Profuse diarrhoea still noted Stools gradually settled, still quite frequent Blood sugars normal, afebrile Blood gases initially took time to improve U&E improved

9
Day 4 - looked hypothyroid
Dry skin Yellowish tinge Small umbilical hernia TSH – mIU/l FT₄ – 10.1 pmol/l Weight on discharge – 3.64kg (almost 1kg more than on admission) Approximately 25% dehydrated on admission Discharged after 6 days, on Eltroxin For follow up at Unit Follow-up clinic
 Approximately 25% dehydrated on admission. Discharged after 6 days, on Eltroxin. For follow up at Unit Follow-up clinic.")
10
Admission 2 23/12/2010 (18 days after discharge) Age 2 ½ months
3 day history of sleeping a lot Mother said no diarrhoea but loose stools noted in nappy No vomiting No cough Apparently still feeding well Now taking breastmilk and Lactogen (soy formula not available) Also started porridge
 Also started porridge.")
11
Examination Ill-looking Afebrile – actually hypothermic (35°c)
Blood sugar – 7.5mmol/l Heart rate 111/min Oxygen saturation 99% in room air Signs of severe dehydration Markedly decreased skin turgor Sunken eyes Capillary refill >3 seconds Dry mucous membranes Acidotic breathing lethargic

12
Management Required 3 fluid boluses
Slow rehydration ( ½ Darrow’s dextrose) Cefotaxime Metabolic screen considered Not kept NPO – continued breast and restarted Isomil Post intake ward round not dysmorphic sclerematous Slightly distended abdomen, soft, having ++ watery stools Scissoring of legs, brisk (3/4 reflexes) Blood culture positive already
 Cefotaxime. Metabolic screen considered. Not kept NPO – continued breast and restarted Isomil. Post intake ward round. not dysmorphic. sclerematous. Slightly distended abdomen, soft, having ++ watery stools. Scissoring of legs, brisk (3/4 reflexes) Blood culture positive already.")
13
Assessed as 2 ½ month old female HIV negative Recurrent admissions (2) for severe gastroenteritis complicated by acidosis Now with hyponatraemia, hypocalcaemia (on gas) Clinically septic with positive blood culture ??other metabolic condition
 Clinically septic with positive blood culture. other metabolic condition.")
14
Results Blood gas FBC CRP U&E CSF Stool red subst Urine red subst
pH WCC 22 Na P Neg (?) Neg* CO₂ Hb K L Bicarb 4 Plts Cl E BE CO₂ <5 Prot 1.65 Ca Urea Gluc 5.5 Lac Creat 72 Cl *on Isomil AG
 Neg* CO₂ Hb K 3.5. L 4. Bicarb 4. Plts 478. Cl 102. E 0. BE CO₂ <5. Prot Ca Urea 9.8. Gluc 5.5. Lac 2.4. Creat 72. Cl 131. *on Isomil. AG 15.")
15
TFT’S Blood cultures FT₄ <5.1 pmol/l 1) E. Coli sensitive to Ampicillin, Cefotaxime TSH mIU/l 2) Coag. neg Staph (43.9hrs) - contaminant Urine – no dipstick results, no Uricult done
 Coag. neg Staph (43.9hrs) - contaminant. Urine – no dipstick results, no Uricult done.")
16
Progress Acidosis improved over next 2 days
U&E improved (sodium increased without additional sodium replacement). Oral potassium given - corrected Blood sugars generally normal – no hypoglycaemia recorded, 2 hyperglycaemia’s noted on day of admission, also on blood gas Temperature improved, no spikes Passed frequent (up to 8) soft stools a day Weight improved to 3,52kg within a week Discharged 01/01/2011 (8 days after admission) T.T.O. - Eltroxin
. Oral potassium given - corrected. Blood sugars generally normal – no hypoglycaemia recorded, 2 hyperglycaemia’s noted on day of admission, also on blood gas. Temperature improved, no spikes. Passed frequent (up to 8) soft stools a day. Weight improved to 3,52kg within a week. Discharged 01/01/2011 (8 days after admission) T.T.O. - Eltroxin.")
17
Admission 3 Readmitted 15/01/2011 (2 weeks after d/c)
Now 3 months of age 3 day history fever, “face yellowish”, cough, diarrhoea, also vomiting Been drinking Lactogen at home. Mother had stopped breastfeeding on previous admission

18
Examination Appeared lethargic, pale, coughing Temperature below 35°c
Bullous lesion on chin, pustules in neck flexure, scalp Acidotic breathing Capillary refill 4 seconds (other signs of dehydration not mentioned) Chest - decreased air entry on right CVS - normal Abdomen – slightly distended
 Chest - decreased air entry on right. CVS - normal. Abdomen – slightly distended.")
19
CNS – increased tone, brisk reflexes
Umbilical hernia, blue-grey discolouration around it Nappy rash CNS – increased tone, brisk reflexes Fontanelle not bulging Assessed as a 3 month old female infant with Recurrent admissions for acute gastroenteritis Hypothyroidism Presenting with sepsis complicated by severe metabolic acidosis ?bronchopneumonia, ?meningitis

20
Management Fluid bolus x 2 Cefotaxime Initially kept nil per os
Nursed in incubator Blood gas Ph – PaCO₂ HCO₃ BE Lac – 1.7 Only results – FBC, CSF, Blood culture WCC – Hb – MCV – Plts - 125 CSF – NAD Blood culture – no growth after 7 days

21
Progress Despite fluids, gas no better. Bolus repeated
Post intake ward round Mild dysmorphism – small chin, low set ears, small upturned nose Chest – crackles bilaterally Assessed as sepsis, bronchopneumonia Cloxacillin added for ? Staph skin lesions

22
Stat dose calcium gluconate, MgSO₄ given
Urine U&E (18/01) Pyruvate LFT TFT CMP Metabolic screen Dipstick NAD Na 37 (N) Bili 2/1 FT₄ Ca Abn org acids Uricult no growth K Prot/ Alb 43/24 TSH 17.7 Mg 0.43 Abn amino acids Cl ALP 270 Po₄ 1.75 Low B₁₂ CO₂ 7 GGT <5 Urea 11 ALT 25 Creat 84 AST 52 Stat dose calcium gluconate, MgSO₄ given
 Pyruvate. LFT. TFT. CMP. Metabolic screen. Dipstick NAD. Na (N) Bili 2/1. FT₄ Ca Abn org acids. Uricult no growth. K 5.4. Prot/ Alb. 43/24. TSH Mg Abn amino acids. Cl 118. ALP 270. Po₄ Low B₁₂. CO₂ 7. GGT <5. Urea 11. ALT 25. Creat 84. AST 52. Stat dose calcium gluconate, MgSO₄ given.")
23
U&E 19/01 20/01 25/01 Na 141 144 K 4.7 5.6 5.7 Cl 120 110 CO₂ 12 13 23 Urea 7.9 5.0 3.5 Creat 26 47 19 AG 17 14

24
Titralac, oral PO₄ enema, Vit D commenced
FBC (19/01) CRP FBC (20/01) FBC (22/01) CMP (20/01) CMP (22/01) CMP (31/01) WCC 14 9 WCC 20 WCC 24 Ca Ca Ca Hb Hb Hb Mg Mg Plts 31 Plts 29 Plts PO₄ 1.13 PO₄ 1.28 PO₄ 1.38 Titralac, oral PO₄ enema, Vit D commenced Started Fluconazole. No growth on blood cultures Stool MC&S (28/01) Yellow, soft, yeast, N flora, no parasites
 CRP. FBC (20/01) FBC (22/01) CMP (20/01) CMP (22/01) CMP (31/01) WCC WCC 20. WCC 24. Ca Ca Ca Hb 7.8. Hb 7.7. Hb 8.8. Mg Mg Plts 31. Plts 29. Plts 54. PO₄ PO₄ PO₄ Titralac, oral PO₄ enema, Vit D commenced. Started Fluconazole. No growth on blood cultures. Stool MC&S (28/01) Yellow, soft, yeast, N flora, no parasites.")
25
Cytogenetic studies (FISH) FOR 22q11 deletion
Negative - no deletion detected Chromosome analysis 46, XX

26
During admission Weaned off oxygen by day 2
Only 1 temp spike whilst in incubator (day 2) Blood sugars normal (2 high on admission) Only 2 stools whilst NPO Restarted feeds day 2-3 Stools charted as normal, on Isomil Nan given (?accidentally) – profuse watery diarrhoea followed Loose stools persisted on Isomil, changed to Alfare after 8 days Fewer stools charted, but loose stools persisted Zinc sulphate given
 Blood sugars normal (2 high on admission) Only 2 stools whilst NPO. Restarted feeds day 2-3. Stools charted as normal, on Isomil. Nan given ( accidentally) – profuse watery diarrhoea followed. Loose stools persisted on Isomil, changed to Alfare after 8 days. Fewer stools charted, but loose stools persisted. Zinc sulphate given.")
27
Cholestyramine, Reuteri drops started whilst on Alfare as loose stools persisting. Not much improvement ??Phosphate enema orally exacerbating diarrhoea – stopped Clinically remained stable, did not require intravenous fluids despite loose stools Took Sorol after loose stools. Always drank very eagerly! Weight unchanged for 2 weeks. Slowly improved to 3.9kg by discharge Discharged 08/02/2011 (3 weeks after admission), on Alfare, Vit D, Titralac, Zinc, Eltroxin
, on Alfare, Vit D, Titralac, Zinc, Eltroxin.")
28
Admission 4 Came to Unit follow-up clinic 21/ (2 weeks after d/c) 4 ½ months of age Mother said had been coughing for a few days Feeding Alfare, correctly mixed, 100ml 3 hourly. Feeding well apparently No vomiting 8 normal stools per day

29
Examination Weight 3.6kg – lost 300 g since discharge
Looked tachypnoeic and lethargic Afebrile (in ward 17 – 38.8°C) Oxygen saturation 90% in room air Heart rate 125/min 5% dehydrated For first time noticed white area on left iris Systems not remarkable, chest clear
 Oxygen saturation 90% in room air. Heart rate 125/min. 5% dehydrated. For first time noticed white area on left iris. Systems not remarkable, chest clear.")
30
Decided to admit Course in ward IV fluids
To monitor condition, avoid antibiotics so sweat test could be done Step down to Isomil, monitor response CXR Course in ward numerous loose stools on Isomil Became very dehydrated within hours Rehydrated, changed back to Alfare Required Ampicillin for bronchopneumonia Responded well to above management Rebooked sweat test

31
Blood cultures Coag neg staph (57 hours) U&E 21/02 22/02 24/02 FBC
TFT’s CMP Na 153 146 142 WCC FT₄ <5.1 FT₄ Ca 2.04 K 3.4 5.4 Hb TSH TSH Mg 0.99 Cl 134 126 112 MCV Po₄ 0.95 CO₂ 9 12 23 Plts Urea 14.8 9.7 2.5 Creat 69 55 25 AG 13 11 Blood cultures Coag neg staph (57 hours)
")
32
Amylase Ammonia LFT Vit D PTH 13 84 TP/Alb 57/37 Not processed 109.9 ALP GGT ALT AST

33
Given Vit B₁₂ IM, zinc sulphate in ward
Discharged after 1 week Weight on discharge – 4.06kg Vit D, Eltroxin, Alfare Called back for weight check 10/03 Weight 4.3kg Still having intermittent loose stools Looking well! For sweat test 18/03/2011

34
Lymphocyte subset analysis (11/03)
WCC 6.08 Lymphocytes 2.81 (N – ) CD3 2012 CD4 1299 CD8 606 IgA, IgM, IgG levels Normal
 CD CD CD IgA, IgM, IgG levels. Normal.")
35
Diarrhoea in infancy & childhood
Frequent passage of loose stools or passage of an increased volume of stool water >200ml/m²/day or > g/m²/day Difficult to measure in children Increase in stool frequency + change to loose/watery stools NB breastfed infants pass frequent stools normally Some say >3 loose stools/day Acute diarrhoea - <2weeks’ duration Chronic diarrhoea - >2 weeks’ duration Persistent diarrhoea - >2 weeks’ duration with dehydration Protracted diarrhoea – severe enough to require nutritional support (parenteral alimentation)
")
36
Mechanism of diarrhoea
Normally stool output dictated by balance between absorption and secretion by intestinal lining – absorption usually > secretion Proportion of water absorption coupled with absorption of nutrients, electrolytes Requires adequate digestion of nutrients Prevent unabsorbable, osmotically active substrates in lumen Diarrhoea occurs if net secretion of water due to ↓ absorption from lumen or ↑secretion/ water loss

37
Normal small intestinal villous architecture

38
↓ functional absorptive area
↓ absorption of water and electrolytes ↑ secretion/ loss of water and electrolytes into lumen ↓ functional absorptive area Decreased intraluminal digestion ↓enterocyte cellular absorptive function ↓intestinal transit ↑ in secretory cells Stimulation of secretory pathways Enterotoxins activate intracellular signal transduction – Cl⁻ secretion ‘Leaky ‘ epithelium Osmotic shift into lumen Effects on enteric nervous system

39
Chronic diarrhoea in infants
Symptom not disease Various underlying causes Previously – term ‘Intractable Diarrhoea of Infancy’ applied to chronic unexplained diarrhoea in children Out of favour – not a discrete disease entity; defined disorders have recently been characterised TPN - better survival of these children Causes of chronic diarrhoea in children can be divided into Diseases having normal villus-crypt architecture Diseases having villus atrophy

40
Normal villus-crypt morphology
Transport defects Chloride-bicarbonate exchanger – Chloride-losing diarrhoea Sodium-hydrogen exchanger – Congenital sodium diarrhoea Ileal bile-salt receptor deficiency Sodium-glucose co-transporter – glucose-galactose malabsorption Abetalipoproteinaemia – fat and fat-soluble vitamin malabsorption Acrodermatitis enteropathica – defect in zinc transport Enzyme defects Enterokinase deficiency – protein malabsorption Primary lactase deficiency – congenital form very rare Pancreatic malabsorption – cystic fibrosis, Shwachman Diamond Syndrome

41
May even be history of polyhydramnios during pregnancy
Surgical congenital/acquired short bowel Malrotation with bacterial overgrowth Dysmotility causing pseudo-obstruction and bacterial overgrowth Blind-loop syndrome with bacterial overgrowth Transport defects and enzyme deficiencies may cause diarrhoea in early neonatal period May even be history of polyhydramnios during pregnancy If consider diagnosis – send stool electrolyte concentrations

42
Villus atrophy Primary epithelial causes
Microvillus inclusion disease neonatal Tufting enteropathy enteropathies Associated with immune system abnormalities Autoimmune enteropathy IPEX syndrome Primary immune deficiencies – SCID, thymic hypoplasia, CD40 ligand deficiency chronic pathogen infection, propensity to autoimmunity Acquired immunodeficiency Recurrent episodes of infection Intestinal lymphangiectasia – PLE, dilated lacteals, decreased circulating lymphocytes

43
Food-sensitive enteropathy
Post-enteritis enteropathy – lactase, sucrase deficiency Cow’s milk protein sensitivity Coeliac disease – after introduction of gluten into diet, PLE Infective enteropathy Post-enteritis enteropathy EPEC Cryptosporidiosis Rotavirus – always associated with disturbed immune function Metabolic conditions Mitochondrial cytopathies (MELAS) Bacterial overgrowth syndrome
 Bacterial overgrowth syndrome.")
44
Inflammatory bowel disease
Very rare in infancy Cryptogenic Syndromatic intractable diarrhoea – dysmorphic features including hypertelorism, broad midface and nose, trichorrhexis nodosa, subtle immunodeficiency, occ cirrhosis

45
Microvillus inclusion disease
Severe enteropathy Watery diarrhoea from day 1 of life Stools even mistaken for urine Faecal sodium and chloride concentrations similar to plasma Volume of stool loss greater than cholera Secretory diarrhoea 2nd most common cause of severe protracted diarrhoea starting during 1st week of life (after infection) Genetic aetiology Intractable diarrhoea, requires parenteral nutrition Fatal without TPN/ intestinal transplant
 Genetic aetiology. Intractable diarrhoea, requires parenteral nutrition. Fatal without TPN/ intestinal transplant.")
46
Histology Villus atrophy Intracytoplasmic microvillus inclusions
Inclusions thought to be due to a genetic defect in trafficking of membrane proteins to apical surface

47
Histopathologic features of classic microvillus inclusion disease
Histopathologic features of classic microvillus inclusion disease. A: Low magnification view of a jejunal biopsy showing total villus atrophy and relatively short crypts. B: Higher magnification of surface enterocytes with vacuolated apical cytoplasm and focal piling-up of cells.

48
Tufting enteropathy Similar to MVID but initially less aggressive
Presents in first few months life Chronic watery diarrhoea Impaired growth Prognosis variable Molecular basis unknown – thought to be due to genetic defect Characteristic feature presence of focal epithelial tufts – closely packed enterocytes, rounding of apical plasma membrane

49
Stained sections from a child with tufting enteropathy showing severe villus atrophy and moderate crypt hyperplasia without a marked inflammatory cell component in the lamina propria

50
Autoimmune enteropathy
Protracted diarrhoea – unresponsive to all dietary exclusions, often requiring TPN Often initially misdiagnosed as post-enteritis/ food- sensitive enteropathy in early stages First few months of life – often only after first 8 weeks, may be perinatal Usually period of good growth prior to onset of symptoms Frequently associated with extra-intestinal manifestations of auto-immunity Most commonly renal disease, polyendocrinopathy (esp. pancreas) Rarely family history of unexplained infant diarrhoea Clinical response to potent immunosuppression
 Rarely family history of unexplained infant diarrhoea. Clinical response to potent immunosuppression.")
51
Males > females (often X-linked)
Consanguinity Can have aggressive or insidious onset May be unmasked by enteric pathogens – often consider infective gastroenteritis/ post-enteritis syndrome/ cow’s milk sensitive enteropathy first Initial management – milk exclusion – lactose-free/ oligoallergenic formula May induce slight improvement because often 2°lactase deficiency Loose stools, weight loss tend to continue

52
Histopathologic features of autoimmune enteropathy
Histopathologic features of autoimmune enteropathy. Jejunal biopsy obtained from a child with autoimmune enteropathy showing total villus atrophy, crypt hyperplasia and a marked mononuclear cell inflammatory infiltrate in the lamina propria.

53
Pathogenesis – circulating systemic antibodies against enterocytes
Similar to Coeliac disease but no history of gluten ingestion prior to onset Pathogenesis – circulating systemic antibodies against enterocytes Levels decline/ disappear on immunosuppressive treatment Titre not proportional to volume of stool losses Pathological findings due to uncontrolled activation of T cells within intestinal mucosa Associated B cell response – enterocyte auto- antibodies Outcome poor Death due to complications of TPN, involvement of other organs by AI process, complications of immunosuppressive treatment

54
IPEX syndrome

55
Only described in males
Usually lethal in infancy/ childhood Growth retardation and cachexia prominent feature May even begin prenatally Not simply due to diarrhoea, malnutrition Possibly also due to excessive cytokines/ TNF Hypocalcamia can occur – in presence of high PTH, possibly due to PTH resistance Also prone to sepsis Enterococcus, staphylococcus Immune dysregulation, drugs, autoimmune neutropenia, loss of skin and gut integrity, malnutrition

56
Pathogenesis Mutation in Foxp3 gene
Foxp3 encodes transcription factor – Scurfin Scurfin involved in T cell signalling, proliferation of CD₄⁺ T cells State of immune hyperreactivity – organ destruction, eczema, lymphadenopathy, cachexia Lack of functional regulatory T cells Many intestinal manifestations similar to AI enteropathy Villus atrophy, marked infiltrate in lamina propria of activated T cells

57
Management of neonatal enteropathies
Nutritional support, adequate hydration most important for growth, development Severe cases – parenteral nutrition early Await nutritional rehabilitation prior to diagnosing exact aetiology Less severe cases – elemental/ low carbohydrate- containing formulae Improve enteral delivery of calories, nutrients Avoid complications associated with TPN

58
Medication Antisecretory agents (somatostatin analogues) variable
Trophic factors (GH, ?colostrum) success Autoimmune enteropathy, IPEX Corticosteroids, cyclosporine, tacrolimus, infliximab, cyclophosphamide Allogeneic bone marrow transplant Microvillus inclusion disease, Tufting enteropathy – poor prognoses Small bowel transplantation, with/ without concomitant liver transplant has been successful
 success. Autoimmune enteropathy, IPEX. Corticosteroids, cyclosporine, tacrolimus, infliximab, cyclophosphamide. Allogeneic bone marrow transplant. Microvillus inclusion disease, Tufting enteropathy – poor prognoses. Small bowel transplantation, with/ without concomitant liver transplant has been successful.")
59
Post-enteritis syndrome
Clinicopathological condition in which small intestinal mucosal damage persists following acute gastroenteritis Sensitization to food antigens classically considered Secondary disaccharidase deficiency to be responsible Both above actually occur to much lesser extent than previously thought Another mechanism thought to be infection/ re-infection with enteric pathogen Pathophysiology remains to be fully clarified

60
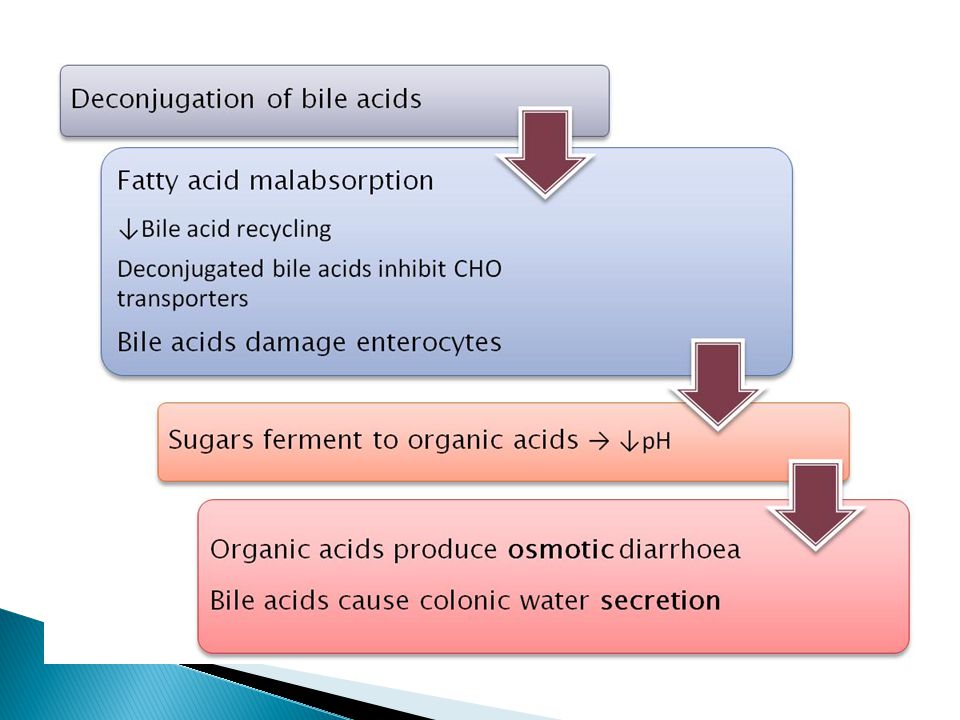
Bacterial overgrowth syndrome
Symptoms occurring due to increased number bacteria stomach, duodenum, jejunum, proximal ileum stem from increased bacterial burden on normal functions of upper GIT Occurs when normal mechanisms which keep numbers low disrupted Structural abnormalities of GIT (congenital/ post-surgery) Decreased acidity Decreased peristalsis Mucosal damage/ atrophy Immunodeficiency Disruption of normal flora
 Decreased acidity. Decreased peristalsis. Mucosal damage/ atrophy. Immunodeficiency. Disruption of normal flora.")
61
Normally Gram positive organisms, anaerobes, aerobes, fungi in colon > ileum > duodenum, jejunum BOS – increased numbers anaerobes, normal flora Vicious cycle follows (pics) Risk factors Malnutrition in neonates/ infants Immunocompromise Intestinal surgery/ congenital GI abnormalities Hypothyroidism - ↓motility Clinically – signs & symptoms of malabsorption Anaemia, steatorrhoea, Vit A deficiency, dermatitis, weight loss/ FTT
 Risk factors. Malnutrition in neonates/ infants. Immunocompromise. Intestinal surgery/ congenital GI abnormalities. Hypothyroidism - ↓motility. Clinically – signs & symptoms of malabsorption. Anaemia, steatorrhoea, Vit A deficiency, dermatitis, weight loss/ FTT.")
64
Try to prevent total eradication of protective organisms
Treatment Antibiotics rebalance enteric florae Try to prevent total eradication of protective organisms Broad spectrum antibiotics (aerobes, anaerobes, particularly Bacteroides fragilis) Augmentin, Clindamycin, Metronidazole Gentamicin – significant improvement <1yr olds Cholestyramine, Flagyl/ Gentamicin been shown to reduce diarrhoea within 4-5 days, infants with idiopathic chronic diarrhoea ?length of treatment
 Augmentin, Clindamycin, Metronidazole. Gentamicin – significant improvement <1yr olds. Cholestyramine, Flagyl/ Gentamicin been shown to reduce diarrhoea within 4-5 days, infants with idiopathic chronic diarrhoea. length of treatment.")
65
Nutrient/ vitamin replacement
Especially important in population who are already deficient Zinc – NB in immunity, wound healing ↓incidence, frequency, severity, persistence of diarrhoea Vit A – NB for maintenance of epithelium Address underlying conditions Infectious diarrhoea Malnutrition Hypothroidism Immunodeficiency

66
Investigation of chronic/ persistent diarrhoea
History Age of onset ?Preceded by episode of acute gastroenteritis Diet – foods which exacerbate diarrhoea Gender (IPEX, AI enteropathy) Drugs, toxins – thyroid hormone Previous bowel surgery Underlying immunodeficiency Other conditions – diabetes, hypothyroidism Family history – males on mother’s side
 Drugs, toxins – thyroid hormone. Previous bowel surgery. Underlying immunodeficiency. Other conditions – diabetes, hypothyroidism. Family history – males on mother’s side.")
67
Look at it – watery, bulky, pasty, oily, blood/mucus
Stool examination Look at it – watery, bulky, pasty, oily, blood/mucus Look at perineum – excoriation suggest acidic stools Reducing substances need liquid component nappies very absorptive may need to repeat must be on lactose-containing diet >1% abnormal Also check stool pH Not useful beyond infancy Stool electrolytes – intractable diarrhoeas

68
Faecal elastase – pancreatic exocrine function
Faecal α₁ Antitrypsin – protein-losing enteropathy Endogenous protein, not secreted, absorbed, digested by GIT Leucocytes, occult blood, lactoferrin – suggestive of infectious diarrhoea Chromatography – identifies malabsorbed sugar Microbiology & microscopy (fresh stool) Fat globules Leucocytes, blood - colitis Should repeat several times Culture for bacterial pathogens Cysts, ova, parasites (cryptosporidia) Viruses Giardia lamblia – duodenal juice, can do faecal antigen test
 Fat globules. Leucocytes, blood - colitis. Should repeat several times. Culture for bacterial pathogens. Cysts, ova, parasites (cryptosporidia) Viruses. Giardia lamblia – duodenal juice, can do faecal antigen test.")
69
Sweat test – sodium test, exclude CF
ΔF508 – commonest mutation, DNA analysis Must be well-hydrated, off antibiotics Sugar hydrogen breath test – bacterial overgrowth Use of different sugars can help distinguish between CHO malabsorptions Stool reducing substances more useful in infants Exclusion diets NPO – if diarrhoea continues – secretory Restrict carbohydrates (lactose) – if improves, likely disaccharidase deficiency Eliminate cow’s milk protein – if improves , possible food- sensitive enteropathy
 – if improves, likely disaccharidase deficiency. Eliminate cow’s milk protein – if improves , possible food- sensitive enteropathy.")
70
Immunological studies
Immune deficiency predisposes to chronic diarrhoea T cell subsets, immunoglobulins, IgG subsets Anti-tissue transglutaminase-IgA , serum IgA – coeliac disease Radiological studies Barium studies – malrotation, blind loops, strictures Small intestinal biopsy Endoscopically usually NB in diarrhoea in children Only way to diagnose coeliac disease

71
CW has genetics clinic appointment 25/03/2011
Isoelectric focussing of transferrin – congenital disorders of glycosylation Rare, rapidly expanding group of clinically heterogeneous disorders Most assoc with psychomotor retardation, dysmorphism CDG type 1b – normal neurodevelopment, predominant symptom diarrhoea CW has genetics clinic appointment 25/03/2011

72
Other investigations Look for complications of diarrhoea, malabsorption May point to aetiology also FBC Anaemia, WCC, platelets U&E Inflammatory markers Albumin Serum iron, ferritin, B12, folate Vit D, calcium, ALP INR

73
Treatment of persistent diarrhoea
1) General supportive measures Early fluid, electrolyte replacement Oral rehydration therapy superior to IV – safer, more efficacious Additional amino acids/ substitution of rice gruel/ cereal for glucose been proposed Increase caloric intake
 General supportive measures. Early fluid, electrolyte replacement. Oral rehydration therapy superior to IV – safer, more efficacious. Additional amino acids/ substitution of rice gruel/ cereal for glucose been proposed. Increase caloric intake.")
74
Though disaccharide deficiency not thought to be major cause of persistent diarrhoea, hypolactasia often 2° to intestinal damage, malnutrition Lactose-free diet recommended (part of WHO treatment algorithm) Lactose replaced by maltodextrins/ other CHO May need sucrose-free formula also Exclusion diets instituted to overcome food intolerance which may be cause or effect of diarrhoea Cow’s milk hydrolysate If not tolerated, amino acid-based formula
 Lactose replaced by maltodextrins/ other CHO. May need sucrose-free formula also. Exclusion diets instituted to overcome food intolerance which may be cause or effect of diarrhoea. Cow’s milk hydrolysate. If not tolerated, amino acid-based formula.")
75
Continuous enteral nutrition beneficial for ↓absorptive function
Rationale - ↑time:absorptive surface ratio → increase daily nutrient absorption Parenteral nutrition may be necessary (early) 2) Nutritional rehabilitation Micronutrient, vitamin supplementation
 2) Nutritional rehabilitation. Micronutrient, vitamin supplementation.")
76
3) Drugs Antibiotics/ probiotics Modification of intestinal microflra
Antibiotics – BOS, bacterial diarrhoea ‘Bowel cocktail’ – Metronidazole, Cholestyramine, Oral Gentamicin Proposed for severe, protracted diarrhoea of suspected infectious aetiology Lacking conclusive proof of efficacy Specific therapy Immunosuppressives for AI enteropathy

77
Drugs to decrease fluid loss
Abnormal ion channels – enkephalinase inhibitor – racecadotril - ↓breakdown of endogenous opiates Somatostatin/ octreotide – severe secretory diarrhoea Loperamide – side effects unacceptable in children Trophic factors (increase cell growth) Growth hormone – used in short gut syndrome Inhibits chloride secretion, improves sodium absorption
 Growth hormone – used in short gut syndrome. Inhibits chloride secretion, improves sodium absorption.")
78
Probiotics Mono- or mixed cultures which must be live organisms
be of human origin be non-pathogenic be viable in delivery vehicles be stable in acid and bile adhere to target epithelial cells persist within GIT produce antimicrobial substances modulate the immune system influence metabolic activities – bile acids, nutrients

79
Beneficially affect host by
Improving properties of indigenous microflora Hampering growth of diarrhoeal pathogens Boost cellular and humoral immunity Evidence for benefit in viral and antibiotic- associated diarrhoea (↓severity, duration) Lactobacillus rhamnosus, L acidophilus, Bifidobacterium bifidum, yeast Saccharomyces boulardi (not human origin) May also help in food-allergies – partial hydrolysis of antigens Prebiotics – fructan, galactan – ferment in bowel → promote growth of beneficial bacteria Given together, enhance efficacy of probiotics Problem – many ‘wannabe’ products – doubtful effectiveness
 Lactobacillus rhamnosus, L acidophilus, Bifidobacterium bifidum, yeast Saccharomyces boulardi (not human origin) May also help in food-allergies – partial hydrolysis of antigens. Prebiotics – fructan, galactan – ferment in bowel → promote growth of beneficial bacteria. Given together, enhance efficacy of probiotics. Problem – many ‘wannabe’ products – doubtful effectiveness.")
80
Questions Is the hypothyroidism related to the cause of the diarrhoea?
Unlikely 2° to diarrhoea already had hypothyroidism on 1st admission Monovalent ions absorbed easily in GIT Hypothyroidism can cause diarrhoea due to ↓motility, BOS but ?should have settled on thyroxin replacement Excessive exogenous thyroxin could cause diarrhoea, but diarrhoea came first….. Recurrent infections Pneumonia, E. coli sepsis, skin lesions and ? Fungal sepsis – never proven HIV negative, lymphocytes slightly low (?significant) Considered CATCH 22 as dysmorphic, recurrent infections, hypocalcaemic, but FISH negative, PTH high, heart normal…..
 Considered CATCH 22 as dysmorphic, recurrent infections, hypocalcaemic, but FISH negative, PTH high, heart normal…..")
81
Hypocalcaemia, ↑PTH level, ?Vit D level, but responded to Vit D
Infections possibly due to immunocompromise 2° to malnutrition, decreased gut mucosal integrity Hypocalcaemia, ↑PTH level, ?Vit D level, but responded to Vit D Why would Vit D have been low? Was on formula and breast, not prem, didn’t look clinically like fat malabsorption Did the diarrhoea just interfere with Ca²⁺ absorption?

82
Summary CW had persistent diarrhoea
Began late neonatal period (7 weeks) Was not ‘intractable’ Female infant ?dysmorphic Hypothyroid Hypocalcaemia – possibly effect of malabsorption No protein losing enteropathy Recurrent infections, no eczema UNLIKELY transport defect, epithelial enteropathies
 Was not ‘intractable’ Female infant. dysmorphic. Hypothyroid. Hypocalcaemia – possibly effect of malabsorption. No protein losing enteropathy. Recurrent infections, no eczema. UNLIKELY transport defect, epithelial enteropathies.")
83
?sucrase-isomaltase deficiency ?CDG
Patient seems to have finally turned the corner and stabilised on Alfare (semi-elemental formula) Could be due to post-enteritis enteropathy, disaccharidase deficiency and/or cow’s milk protein intolerance Maybe just needed longer for bowel to recover Problem – accessing formula. When to step down? If relapses again, for SB biopsy ?AI enteropathy ?sucrase-isomaltase deficiency ?CDG ?Cystic fibrosis – but stools seemed watery, not typical – sweat test => negative
 Could be due to post-enteritis enteropathy, disaccharidase deficiency and/or cow’s milk protein intolerance. Maybe just needed longer for bowel to recover. Problem – accessing formula. When to step down If relapses again, for SB biopsy. AI enteropathy. sucrase-isomaltase deficiency. CDG. Cystic fibrosis – but stools seemed watery, not typical – sweat test => negative.")
84
Resolution can take a long time…
Mucosal atrophy can result in an 80% reduction of intestinal surface area in infants Once the offending agent is removed, repair of the small bowel progresses slowly After 2 months, the villi surface area is 63% normal but the microvillous surface area is only 38% normal.

Similar presentations