Download presentation
Presentation is loading. Please wait.

1
بنام خداوند جان وخرد

2
ORTHOPAEDIC EMERGENCIES DR.Hossein Saremi Orthopaedic surgeon Hand&shoulder fellowship Hamedan University of medical sciences

3
A musculoskeletal injury or condition that, if missed, could result in additional complications, significant impairment, or death and needs immediate management Orthopaedic Emergencies

4
Definition “ missed” = Lawsuit“ missed” = Lawsuit “additional complications” = Lawsuit“additional complications” = Lawsuit “impairments” = Lawsuit“impairments” = Lawsuit Delaied management=LawsuitDelaied management=Lawsuit “death” = Lawsuit“death” = Lawsuit

5
Emergent orthopaedic conditions Open FXOpen FX DislocationDislocation Compartement syndromCompartement syndrom Any FX with associated vascular injuryAny FX with associated vascular injury

6
Open FX the skin overlying a fracture is broken, allowing communication between the fracture and the external environmentthe skin overlying a fracture is broken, allowing communication between the fracture and the external environment Inside-outInside-out Outside-inOutside-in

7
Open FX complications Soft tissue infectionSoft tissue infection OsteomyelitisOsteomyelitis Gas gangreneGas gangrene TetanusTetanus Crush syndromeCrush syndrome Skin lossSkin loss Non-unionNon-union

8
Open Fx Management DOs: Control the bleedingControl the bleeding Cover with sterile dressingCover with sterile dressing SplintSplint IV antibioticsIV antibiotics Tetanus prophylaxisTetanus prophylaxis DON’Ts: Scream and pass out Replace protruding bone Explore wound Clamp vessels

9
Debridement Conservativedebridement

10
Debridement Pasteur : It is the environment not the bacteria that determines whether a wound becomes infectedPasteur : It is the environment not the bacteria that determines whether a wound becomes infected

11
Open Joint Any open wound over or near a joint should be assumed to extend to the joint until proven otherwise Any open wound over or near a joint should be assumed to extend to the joint until proven otherwise

12
Dislocation Displacement of bones at a joint from their normal positionDisplacement of bones at a joint from their normal position May be associated with neurovascularMay be associated with neurovascular injury injury Cartilage damageCartilage damage

13
Dislocation-Knee Anterior (31%)Anterior (31%) –Caused by hyperextension –Often ACL and PCL both torn –MCL and/or LCL usually injured –Popliteal artery- intimal tear Posterior (25%)Posterior (25%) –ACL and PCL torn –Possible tear of extensor mechanism –Avulsion or disruption of popliteal artery Lateral (13%)Lateral (13%) Medial (3%)Medial (3%) Rotary (4%)- usually posterolateralRotary (4%)- usually posterolateral
Anterior (31%) –Caused by hyperextension –Often ACL and PCL both torn –MCL and/or LCL usually injured –Popliteal artery- intimal tear Posterior (25%)Posterior (25%) –ACL and PCL torn –Possible tear of extensor mechanism –Avulsion or disruption of popliteal artery Lateral (13%)Lateral (13%) Medial (3%)Medial (3%) Rotary (4%)- usually posterolateralRotary (4%)- usually posterolateral")
14
Dislocation-Knee

15
Dislocation-Hip Usually high-energy traumaUsually high-energy trauma More frequent in young patientsMore frequent in young patients Anterior- hip in external rotationAnterior- hip in external rotation Posterior- hip in internal rotationPosterior- hip in internal rotation Central acetabular fracture dislocationCentral acetabular fracture dislocation May result in avascular necrosisMay result in avascular necrosis Sciatic nerve injury in 10-35%Sciatic nerve injury in 10-35%

16
Reduction

17
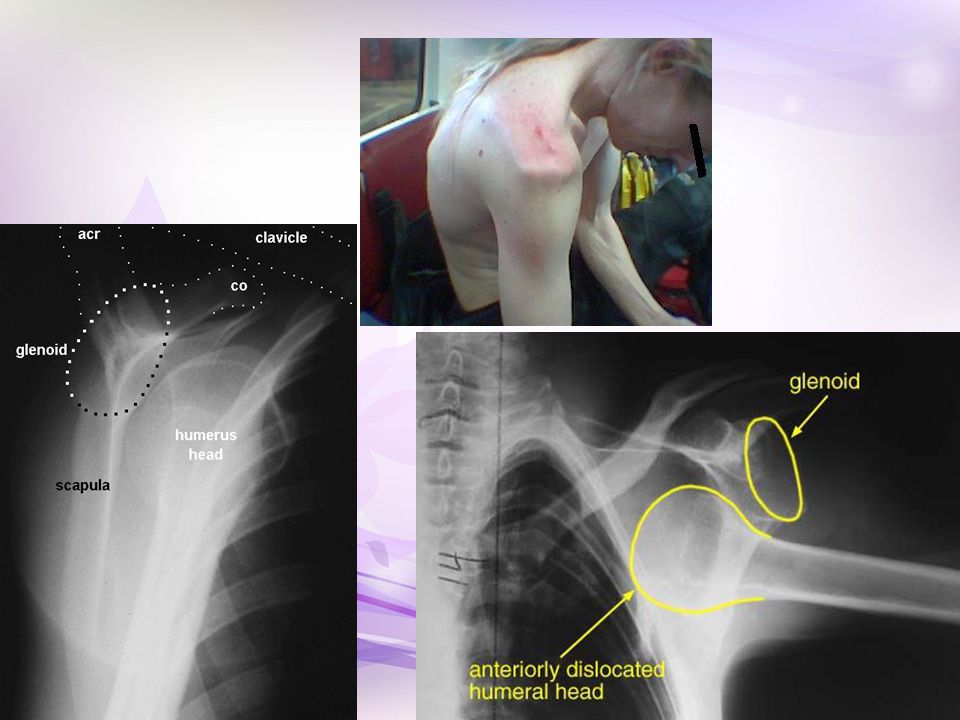
Dislocation-Shoulder Most common major joint dislocationMost common major joint dislocation May be associated with:May be associated with: –Bankart lesion –Fracture dislocation –Hill sachs lesion –SLAP lesion –Rotator cuff tear –Nerve injury- axillary, posterior cord, musculocutaneous musculocutaneous

18
Dislocation-Shoulder Anterior (95%)Anterior (95%) –Arm abducted and externally rotated Posterior (2-4%)Posterior (2-4%) –Arm adducted and internally rotated –Electrocution, seizure Inferior (1%)Inferior (1%) –Hyperabduction –Usually associated with significant trauma
Anterior (95%) –Arm abducted and externally rotated Posterior (2-4%)Posterior (2-4%) –Arm adducted and internally rotated –Electrocution, seizure Inferior (1%)Inferior (1%) –Hyperabduction –Usually associated with significant trauma")
20
Dislocation-shoulder Reduction (ant disloc)Reduction (ant disloc) Stimson (hanging weight technique)Stimson (hanging weight technique) Scapular ManipulationScapular Manipulation Leidelmeyer (external rotation)Leidelmeyer (external rotation) MilchMilch Traction-CountertractionTraction-Countertraction Reduction (post disloc)Reduction (post disloc) Traction on internally rotated and adducted arm with pressure on humeral headTraction on internally rotated and adducted arm with pressure on humeral head
Reduction (ant disloc) Stimson (hanging weight technique)Stimson (hanging weight technique) Scapular ManipulationScapular Manipulation Leidelmeyer (external rotation)Leidelmeyer (external rotation) MilchMilch Traction-CountertractionTraction-Countertraction Reduction (post disloc)Reduction (post disloc) Traction on internally rotated and adducted arm with pressure on humeral headTraction on internally rotated and adducted arm with pressure on humeral head")
21
Simple Reduction manuvere

22
Post-reduction neurovascular exam Axillary nerve Radial pulse Post-reduction x-raysPost-reduction x-rays ReductionReduction FracturesFractures

23
Follow up

24
Dislocation-Elbow Second most common major joint dislocationSecond most common major joint dislocation Usually closed and posteriorUsually closed and posterior Fall on extended elbowFall on extended elbow Posterior, posterolateral, posteromedial, lateral,Posterior, posterolateral, posteromedial, lateral, medial, or divergent Complex- dislocation with fracture (35-40%)Complex- dislocation with fracture (35-40%) –Radial head fracture most common Simple- dislocation without fractureSimple- dislocation without fracture –Rupture of capsule, rupture of MCL and lateral ligaments, rupture of flexor pronator mass, possible injury to brachialis muscle and rupture of brachial artery
Complex- dislocation with fracture (35-40%) –Radial head fracture most common Simple- dislocation without fractureSimple- dislocation without fracture –Rupture of capsule, rupture of MCL and lateral ligaments, rupture of flexor pronator mass, possible injury to brachialis muscle and rupture of brachial artery")
26
Elbow DX

27
Dislocation-Elbow Nerve inuryNerve inury Neuropraxia involving median or ulnar nerve in 20% of elbow dislocationsNeuropraxia involving median or ulnar nerve in 20% of elbow dislocations Ulnar nerve palsies more common in pediatricUlnar nerve palsies more common in pediatric Most neuro deficits are transientMost neuro deficits are transient

28
Dislocation-Elbow Nerve inuryNerve inury Neuropraxia involving median or ulnar nerve in 20% of elbow dislocationsNeuropraxia involving median or ulnar nerve in 20% of elbow dislocations Ulnar nerve palsies more common in pediatricUlnar nerve palsies more common in pediatric Most neuro deficits are transientMost neuro deficits are transient

29
Dislocation-ankle

30
Dislocation-ankle Described by relationship of talus to tibiaDescribed by relationship of talus to tibia Usually associated with fractureUsually associated with fracture Pre/post-reduction neurovascular exam and x- raysPre/post-reduction neurovascular exam and x- rays Adequate analgesia vs conscious sedationAdequate analgesia vs conscious sedation Reduction (even if open)Reduction (even if open) SplintSplint Ortho for washout if openOrtho for washout if open
Reduction (even if open) SplintSplint Ortho for washout if openOrtho for washout if open")
31
Fractures,Examine vascular status

32
Compartement syndrom Limb threateningLimb threatening Increased pressure in tight fascial compartmentIncreased pressure in tight fascial compartment Muscle necrosis at > 30mm HgMuscle necrosis at > 30mm Hg Ischemic injury at 4 hrsIschemic injury at 4 hrs Irreversible injury 4-8 hrsIrreversible injury 4-8 hrs Signs: disproportionate pain, 5 P’sSigns: disproportionate pain, 5 P’s o Pain o Pallor o Paraesthesiae o Paralysis o Pulseless

33
0 mm Hg0 mm Hg 10 mm Hg10 mm Hg 30 mm Hg30 mm Hg 60 mm Hg60 mm Hg 120 mm Hg120 mm Hg Pulse PressurePulse Pressure IschemiaIschemia Elevated PressureElevated Pressure NormalNormal Difference between diastolic pressure and compartment pressure (delta pressure)< 30mmHg is indication for immediate decompressionDifference between diastolic pressure and compartment pressure (delta pressure)< 30mmHg is indication for immediate decompression
< 30mmHg is indication for immediate decompressionDifference between diastolic pressure and compartment pressure (delta pressure)< 30mmHg is indication for immediate decompression")
34
Causes of compartement syndrom Fractures ~75%Fractures ~75% Crush injuryCrush injury BurnsBurns ExtravasationExtravasation Tourniquets, constrictive dressings/plastersTourniquets, constrictive dressings/plasters Snake bitesSnake bites

37
Management Early recognition!Early recognition! Urgent fasciotomiesUrgent fasciotomies

38
Compartement syndrom Volkman ischaemic contracturesVolkman ischaemic contractures Permanent nerve damagePermanent nerve damage Limb ischaemia and amputationLimb ischaemia and amputation Rhabdomyolysis and renal failureRhabdomyolysis and renal failure

Similar presentations