Download presentation
Presentation is loading. Please wait.

1
60 y.o. Nodule in the finger CASE 28

7
Case History Oct 2004 Excision with split-skin grafting Histology moderately differentiated squamous cell carcinoma with large areas of necrosis and brisk mitotic activity. Second episode of red cell aplasia- CLL- immuosupressed Blood transfusion Rituximab

8
October 2004

9
October 2005

10
Three months later

11
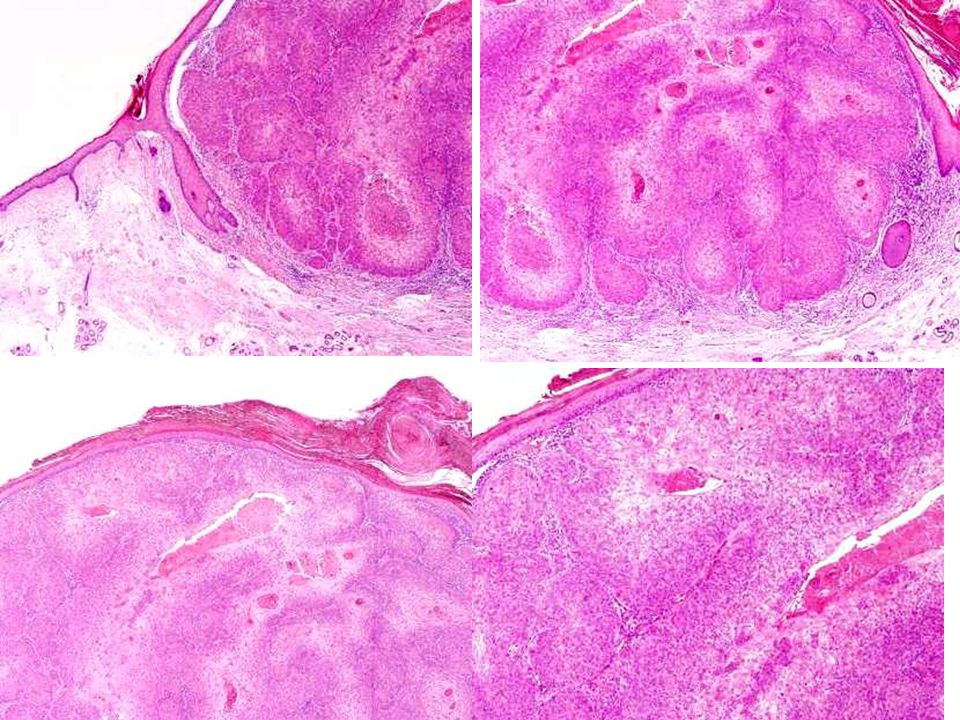
Histology

12
PAS Stain

13
Revised Diagnosis Eccrine porocarcinoma

14
Progress Dec 2005 Amputation declined Interferon alpha 5 million units three-times weekly April 06 New inguinal lymphadenopathy CT appearance in keeping with metastatic disease Commenced weekly Paclitaxel 70mg/m 2

15
January 2006

16
April 2006

17
August 2006

18
December 2006

19
Management Summary Interferon-alpha Dec 2005-April 2006 –5MU sc 3 times a week Paclitaxel chemotherapyApril 2006 –weekly for 12/52 Capecitabine August 2006 –2g bd for 14/7 2 cycles over 6/52; PO –(Fluoropyrimidine Tegafur) Thalidimide
 Thalidimide")
20
Eccrine porocarcinoma (EP) Rare tumour derived from the acrosyringium of the eccrine gland First described in 1963 by Mehregan and Pinkus 200 cases in the literature Most prevalent malignant eccrine tumour
 Rare tumour derived from the acrosyringium of the eccrine gland First described in 1963 by Mehregan and Pinkus 200 cases in the literature Most prevalent malignant eccrine tumour")
23
Eccrine Porocarcinoma –F>M –Age 73 years (29-91years) –Site Lower Extremity (44%) Trunk (24%) Head (18%) –Clinical Appearance Variable –Histologic Pattern Wide variation →Diagnostic Error –Prognosis Mitosis (14mitosis/high power field) Lymphovascular invasion Tumour Depth (>7mm)
 –Site Lower Extremity (44%) Trunk (24%) Head (18%) –Clinical Appearance Variable –Histologic Pattern Wide variation →Diagnostic Error –Prognosis Mitosis (14mitosis/high power field) Lymphovascular invasion Tumour Depth (>7mm)")
24
Eccrine Porocarcinoma

25
Clinical presentation 6 th to 8 th decade Equal sex preponderance Lower limb>>trunk>head&neck>upper limb Soliatry enlarging nodule Variable appearance Diagnosis rarely suspected clinically 18%-30% arise within benign eccrine poroma

26
ECCRINE POROCARCINOMA: HISTOLOGY Cords and lobules of polygonal cell tumor in the dermis, some of which have squamoid features and central necrosis Overt nuclear atypia with nucleoli Permeative peripheral growth Intraepidermal tumour cells in "lakes," often centered on acrosyringial pores

27
Histology Poromatous basaloid epithelial cells Ductal differentiation Cytological atypia Variety of patterns: Squamous differentiation Clear cell differentiation Mucus metaplasia Spindle cell differentiation

28
Prognosis Robson et al 2001 Retrospective study 54 cases of EP 9 (17%) local recurrence 10 (19%) regional lymph nodes 6 (11%) distant metastases (4 deaths, 7%)
 local recurrence 10 (19%) regional lymph nodes 6 (11%) distant metastases (4 deaths, 7%)")
29
Histological parameters associated with aggressive disease >14 Mitoses per high power field Tumour depth >7mm Lymphovascular invasion Presence of an advancing infiltrative border

30
Treatment-metastatic disease Radiotherapy not effective Chemotherapy TamoxifenPaclitaxel Isotretinoin5-FU/Cisplatin/Radiotherapy IFN-alphaIsotretinoin/IFN-alpha DocetaxelDocetaxel +topical 5-FU 5-FUIFN-alpha +IL-2

31
Previous reports of patients with metastatic EP (mEP) treated with taxanes AuthorClinical presentation RxOutcome Plunkett et al, 2001 45 y.o. Renal transplant, history of Hodgkins lymphoma, mEP to lung Failed epirubicin Docetaxel 100mg/m 2 Disease stability 3/12 post treatment,required 2nd course Gutermuth et al 2004 67 y.o. mEP to regional lymph nodes IFN-alpha 9Miu 3x-weekly, 5# weekly Paclitaxel 100mg/m 2 No evidence of disease progression after 7 months De Bree et al 2005 69 y.o,mEP to ribs Failed IFN-alpha and isotretinoin Daily top 5-FU and 3# intra- arterial docetaxel 75mg/m 2, 2# systemic docetaxel 80mg/m 2 Disease stability after 25 months with complete histological response of skin lesions (anaphylaxis to systemic docetaxel after 3 rd # so treatment stopped)
.")
32
Pathogenesis Poorly understood-polyoma virus co-carcinogen? Role of immunosuppression? C Harwood et al, 2003 Immunosuppressed renal transplant population at greatly increased risk of appendageal tumour compared with immunocompetent population Greater proportion of these were malignant

33
DERMATOPATHOLGY- CPC

34
WELCOME! GRAZIE! 2012

Similar presentations















>")









