Download presentation
Presentation is loading. Please wait.

1
OCCUPATIONAL CANCER Dr. Majid Golabadi Occupational Medicine Specialist Isfahan University of Medical Sciences

2
Cancer is a large group of diseases (over 200) characterized by uncontrolled growth and spread of abnormal cells. What Is Cancer?

3
The majority of cancers in adults: Genetic factors Lifestyle Environmental and occupational exposure

4
Stress Sleep disturbances, Diet: high fat and low in fruits and vegetables Lack of exercise Chemicals In Foods Smoking – 30% of all cancer deaths, 87% of lung cancer deaths Obesity – 50% higher risk for breast cancer in postmenopausal women, 40% higher risk in colon cancer for men Viral Factors

5
5-10% of all human cancers are thought to be caused by occupational exposure to carcinogens Carcinogen: Any chemical, physical or biologic agent present at the workplace which increases the risk of cancer among exposed workers

6
Stages in Tumor Development 1. Initiation Cancers come from an abnormal cell (mutation in DNA) 2. Promotion To a benign or preneoplastic tumor 3. Progression To a malignant tumor

7
Carcinogens Initiator Promoter Complete Carcinogens

8
Medical surveillance : Occupational cancers are completely preventable Induction-latency period 3-5 years for radiation or toxin induced leukemias 40 or more years for some cases of asbestos- induced mesothelioma For Solid tumors usually 10-25 years There is controversy about the existence of threshold doses for carcinogenic agents

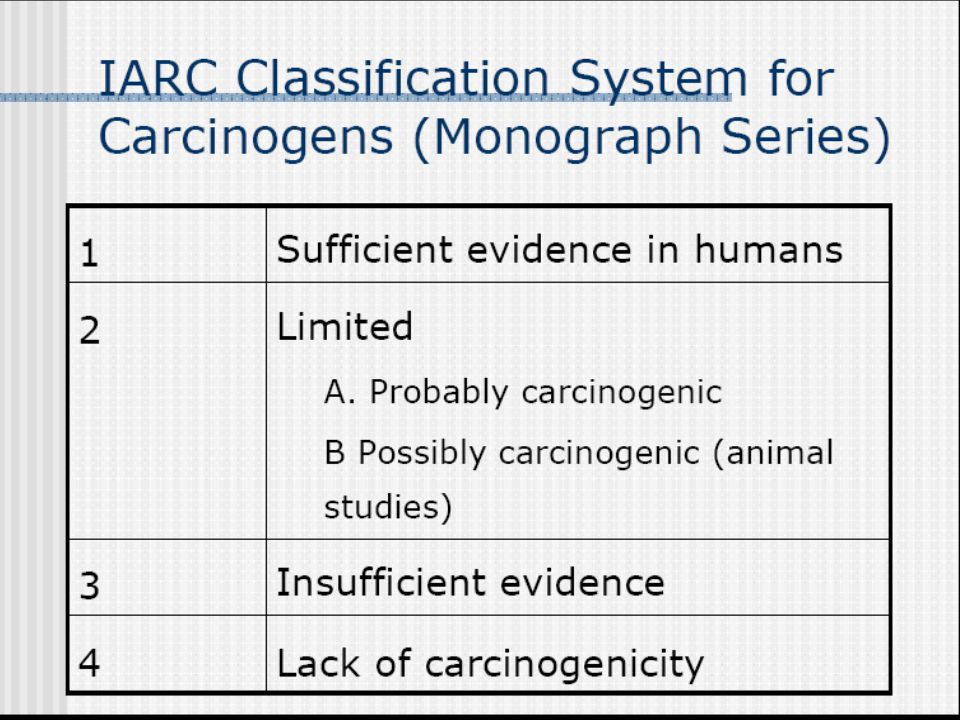
10
OCCUPATIONAL CANCER Avoid the use of chemical in IARC groups 1 and 2A Use agent in group 2B only with very tight controls when there are no viable alternatives

11
OCCUPATIONAL HUMAN CARCINOGENS GROUP 1 (IARC) CLASSIFICATION Arsenic Lung, Skin, Liver Asbestos Pleura & peritoneum, Lung, Larynx, GI BenzeneLeukemia BerylliumLung CadmiumLung ChromiumLung Coal tar Skin, Scrotum, Lung Mustard gas Lung Nickel Lung, Nasal sinus Solar radiation Skin Vinyl chloride Liver
 CLASSIFICATION Arsenic Lung, Skin, Liver Asbestos Pleura & peritoneum, Lung, Larynx, GI BenzeneLeukemia BerylliumLung CadmiumLung ChromiumLung Coal tar Skin, Scrotum, Lung Mustard gas Lung Nickel Lung, Nasal sinus Solar radiation Skin Vinyl chloride Liver")
12
Selected industrial processes causally associated with human cancer Industrial process AgentCancer site Aluminum production PAH Lung,bladde r Shoe manufacture BenzeneLeukemia Iron and steel founding PAH,Silicalung Rubber industryAromatic amines, solvents Bladder, leukemia

13
عوامل زیان آور شغلی

14
LUNG MESOTHELIOMA NASAL CAVITY & SINUSES LARYNX BLADDER LIVER SKIN HEMATOLOGIC

15
LUNG CANCER

16
The currently accounts for almost 30% of all cancer deaths The most preventable risk factor: cigarette smoking In occupations with high prevalence of smoking There is no one cell type that is pathognomonic of an occupationally related lung cancer

17
Asbestos Radon Chloromethyl ethers PAHs Chromium Nickel Arsenic Mustard

18
Asbestos (Asbestos miners, Textile, Insulation,filter, Shipyard)
")
19
Blue asbestos (Crocidolyte) White asbestos (Chrysotile) Brown asbestos (Amosite)
 White asbestos (Chrysotile) Brown asbestos (Amosite)")
20
Asbestos The accounting for 20% of all deaths in asbestos- exposed 7% of all lung cancer is attributable to asbestos exposure. A latency period: 20 years Synergic effect with Smoking Cigarette smoke: initiator Asbestos: promoter Adenocarcinoma

21
Radon (Uranium mining, Domestic exposure) Excessive lung cancer in uranium miners is independent of cigarette smoking, although exposure to both is synergistic
 Excessive lung cancer in uranium miners is independent of cigarette smoking, although exposure to both is synergistic")
22
Polycyclic Aromatic Hydrocarbons (PAHs) From the incomplete combustion of coal tar, pitch, oil and coke The scrotal cancer in chimney sweeps (Dermal exposure to soot) Coke oven workers, Roofers, Printers, Truckers, Rubber plant workers, Asphalt workers
 From the incomplete combustion of coal tar, pitch, oil and coke The scrotal cancer in chimney sweeps (Dermal exposure to soot) Coke oven workers, Roofers, Printers, Truckers, Rubber plant workers, Asphalt workers")
23
Chloromethyl Ethers Chloromethylmethyl ether (CMME) Bischloromethyl ether (BCME) Bactericides, Pesticides, Dispersing agents, Water repellents, Flame-proofing agents Small cell lung cancer
 Bischloromethyl ether (BCME) Bactericides, Pesticides, Dispersing agents, Water repellents, Flame-proofing agents Small cell lung cancer")
24
Arsenic (Organic Arsenic) Lead, Copper and Zinc smelting Pesticides Chromium Chromate production Nickel Soluble forms
 Lead, Copper and Zinc smelting Pesticides Chromium Chromate production Nickel Soluble forms")
25
Probably Carcinogenic for lung cancer Acrilonitryl Beryllium Cadmium Vinyl chloride Formaldehyde Acid Sulfuric

26
Medical monitoring in the workplace (Screening ) Periodic examination: History, Physical exam, smoke, training Symptoms: persistent cough, blood-streaked sputum, chest pain, Voice change Environmental monitoring Serial Chest Radiography and Sputum cytology (OSHA,NIOSH) CT Scan (spiral,…..), HRCT
 Periodic examination: History, Physical exam, smoke, training Symptoms: persistent cough, blood-streaked sputum, chest pain, Voice change Environmental monitoring Serial Chest Radiography and Sputum cytology (OSHA,NIOSH) CT Scan (spiral,…..), HRCT")
27
Prevention Primary prevention: The most effective methods Complete avoidance of exposure to the carcinogen Identification of etiologic agents in the workplace Worker education

28
Asbestos miners Textile manufacturing Insulation and filter production Construction workers Welders, Plumbers, electricians Roofers Shipyard workers Asbestos

29
The latency period: 30 years or more Cigarette smoking dose not increase the risk of MM Pleural effusion, pleural thickening or nodularity, interstitial pulmonary fibrosis, pleural plaques, pleural calcification Symptoms: Persistent gnawing chest pain, dyspnea, dry cough, weight loss MESOTHELIOMA CXRay: Unilateral pleural effusion CT_Scan: Most sensitive test for pleural surface Sputum cytology Thoracentesis Thorachotomy and thoracoscopy

30
MESOTHELIOMA Treatment: Surgical Radiotherapy Chemotherapy Prognosis: 75% of patients die within 1 year after diagnosis Pleura, peritoneal

32
More frequent in men than women (2:1) Usually squamous cell histology (50%), The disease is very uncommon in workers under 50 years of age, and rates increase with age
 Usually squamous cell histology (50%), The disease is very uncommon in workers under 50 years of age, and rates increase with age")
33
Wood and other dusts ( Furniture, Textile, boot and shoe manufacturing, bakes ) Chromium ( Nasal septum ulcer and perforation ) (Chromate pigment production, metal plating ) Nickel (Nickel refinery workers) Isopropyl alcohol, Formaldehyde (laboratory workers, other industries ) Owen workers, foundry workers, Radium, Radon, mustard
 Chromium ( Nasal septum ulcer and perforation ) (Chromate pigment production, metal plating ) Nickel (Nickel refinery workers) Isopropyl alcohol, Formaldehyde (laboratory workers, other industries ) Owen workers, foundry workers, Radium, Radon, mustard")
34
Symptoms: Unilateral nasal obstruction Non-healing ulcer Occasional bleeding A low-grade chronic infection, associated with discharge, obstruction,and minor intermittent bleeding

35
Chronic hypertrophic rhinitis Dry atrophic nasal mucosa Nasal polyps Almost Adenocarcinomas

36
Prevention Primary prevention: Complete avoidance of exposure to the carcinogen is the ultimate goal, but this is not always possible Identification of etiologic agents in the workplace Worker education

38
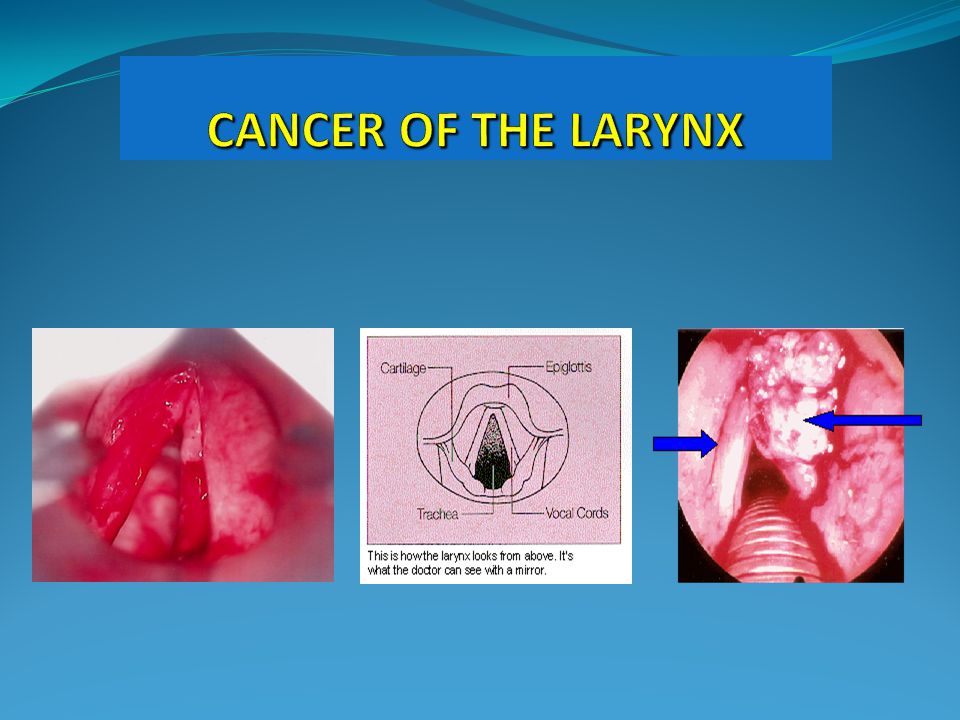
Laryngeal cancer is primarily a disease of older workers. Cancer of the larynx is much more common than sinonasal cancer Cigarette smoking and alcohol abuse are the primary etiologic factors Much more frequent in men than women (4.5:1),usually middle aged or older
,usually middle aged or older.")
39
Asbestos miners Textile manufacturing Insulation and filter production Shipyard workers Asbestos

40
Hoarseness is an early presenting symptom Usually squamous cell histology At the time of diagnosis: 60% localized 30% regional spread 10% distance metastases 40% supra-glottic, 59% glottic, 1% sub-glottic

41
Prevention Primary prevention: Complete avoidance of exposure to the carcinogen is the ultimate goal, but this is not always possible Identification of etiologic agents in the workplace Worker education Periodic examination: History, Physical exam, smoke, training Environmental monitoring (limits)
")
42
BLADDER CANCER

43
5% of all malignant tumors M/F = 2/1 Cigarette smoking is the most important etiologic factor (60%) Water infected to pesticides and other chemicals The latency period: mean of 20 years Presenting complaints of hematuria and vesical irritability Diagnosis by urine cytologic examination and cystoscopy
 Water infected to pesticides and other chemicals The latency period: mean of 20 years Presenting complaints of hematuria and vesical irritability Diagnosis by urine cytologic examination and cystoscopy")
44
Naphtylamine (Textile workers, Dye & pigment manufacture, Rubber manufacture) 4-Aminobiphenyl (Tire & Rubber manufacture) Benzidine (Dye & pigment manufacture) Chlornaphazine (leather worker) O-toluidine (Painters, Textile workers, Bootblacks) Phenastin (Petroleum workers, Hairdressers)
 4-Aminobiphenyl (Tire & Rubber manufacture) Benzidine (Dye & pigment manufacture) Chlornaphazine (leather worker) O-toluidine (Painters, Textile workers, Bootblacks) Phenastin (Petroleum workers, Hairdressers)")
45
High exposed workers Textile workers, Dye & pigment manufacture, Tire & Rubber manufacture leather worker Painters, Bootblacks Petroleum workers, Hairdressers

46
4- Aminobiphenyl

47
Chlornaphazine

48
Benzidine

49
Pathogenesis & Pathology Body exposure via GI, Dermal or Respiratory Caused by contact of the bladder epithelium with carcinogens in the urine The bladder is exposed to higher concentration of these materials than other body tissues Urothelial tumors: 90% transitional cell type 6-8 % squamous cell 2% adenocarcinoma

50
Clinical findings The most common: Hematuria 80% Painless, gross, and intermittent 20%: the vesical irritability alone, with increased frequency, dysuria, urgency and nocturia U/A: RBC, Blood Anemia, Uremia

51
Prognosis Prognosis varies with the stage of the disease Superficial: The excellent 5-year survival Muscle invasion: 40-50% of patients 5-year survival Local spread of disease in the pelvis: 10-17% of patients survive 5 years

52
Screening Urine cytology and U/A: Screening tool Sensitivity (75%),specifity (99.9%) Used to screen only certain at risk occupations The screening of high-risk patients may result in a significant reduction of the stage of disease at diagnose, with improved long-term survival
,specifity (99.9%) Used to screen only certain at risk occupations The screening of high-risk patients may result in a significant reduction of the stage of disease at diagnose, with improved long-term survival")
53
Vinyl chloride (PVC production) Arsenic (Pesticide, Copper,Lead, Zinc smelting, Wine maker, Fowler) Thorotrast
 Arsenic (Pesticide, Copper,Lead, Zinc smelting, Wine maker, Fowler) Thorotrast")
54
Hepatic Angiosarcoma Angiosarcoma of the liver is a rare tumor M/F: 4/1 Major exposure to vinyl chloride Sign & symptoms RUQ abdominal pain, weight loss Hepatomegaly on physical examination Diagonisis by hepatic arterogram and liver biopsy

55
Clinical Findings Non-specific: Fatigue, weakness, and weight loss are seen in 25-50% of patients The some patients may be asymptomatic Abdominal pain is the most common symptom, usually in the RUQ Phx: Hepatomegaly with ascites Jaundice Splenomegaly, abdominal mass, tenderness

56
Laboratory findings A mild anemia, target cells and schistocytes Leukocytosis and thrombocytopenia (1/2 patients) Prolonged PT Almost all patients: abnormality of liver function testing ALT, AST and ALP
 Prolonged PT Almost all patients: abnormality of liver function testing ALT, AST and ALP")
57
Screening tests Periodic testing: History and physical examination CBC, LFT (SGOT, SGPT, ALP)
")
58
UV radiation (Outdoor workers, welding arc) PAHs (coal tar workers, Electrode production, Pigment Industry, Roofers, Shale oil worker) Ionizing radiation (Uranium miners, Health care workers, Military personnel) Arsenic (Pesticide, Copper,Lead, Zinc smelting) Chronic inflamation
 PAHs (coal tar workers, Electrode production, Pigment Industry, Roofers, Shale oil worker) Ionizing radiation (Uranium miners, Health care workers, Military personnel) Arsenic (Pesticide, Copper,Lead, Zinc smelting) Chronic inflamation")
59
UV Radiation Major risk is ultraviolet radiation There are 4.8 million outdoor workers in the USA (agriculture,…) The estimated 300000 workers are exposed to industrial radiation sources ( welding arc, germicides and printing processors)
 The estimated workers are exposed to industrial radiation sources ( welding arc, germicides and printing processors)")
60
PAHs

61
Ionizing radiation & skin cancer High risk: more than 1000 cGy Early radiation workers with heavy exposure: Predominantly SCC The hands and feet and occasionally on the face More recently, basal cell cancers have been described following repeated occupational exposures

62
Punctate keratoses of the palms and soles and hyperpigmentation are frequently seen Arsenic

63
Ionizing radiation (Nuclear power plant worker, Health care worker, Military personnel) Benzene (Petrochemical and refinery worker, Rubber worker)
 Benzene (Petrochemical and refinery worker, Rubber worker)")
64
Ionizing radiation & aplastic anemia Dose dependent Large dose & long term (small amount) Risk: Increased until 3-5 years after exposure After which there is a marked decline in incidence Treatment: Bone marrow transplantation,hematopoietic growth factors
 Risk: Increased until 3-5 years after exposure After which there is a marked decline in incidence Treatment: Bone marrow transplantation,hematopoietic growth factors")
65
Benzene & leukemia Benzene is a cyclic hydrocarbon obtained in distillation of petroleum and coal tar It is used widely in chemical synthesis in many industries Explosives,soap,perfums, Drugs,dyes,rubber,shoes

66
Benzene & leukemia Workers exposed for 5 years or more had a 21-fold increased risk of death from leukemia Aplastic or hypoplastic anemia Acute, chronic (30 years after exposure) Exposure to 100 ppm cause cytopenia
 Exposure to 100 ppm cause cytopenia")
Similar presentations






>")








. Leukemia is cancer of the blood.>")



 l malignant (very common) r Metastatic (Very common)>")

