Download presentation
Presentation is loading. Please wait.

1
Cardio pulmonary resuscitation

2
Cardiac arrest-abrupt cessation of cardiac pump function,which may be reversible
Most victims of SCA demonstrate ventricular fibrillation (VF) at some point in their arrest. Resuscitation is most successful if defibrillation is performed in about the first 5 minutes after collapse High survival rates depends on a public trained in CPR and on well-organized public access defibrillation programs Bystander CPR is performed in about only a third of witnessed arrests.
 at some point in their arrest. Resuscitation is most successful if defibrillation is performed in about the first 5 minutes after collapse. High survival rates depends on a public trained in CPR and on well-organized public access defibrillation programs. Bystander CPR is performed in about only a third of witnessed arrests.")
3
Adult Basic Life Support
BLS refers to maintaining airway patency and supporting breathing and the circulation, without the use of equipment other than a protective device includes recognition of signs of sudden cardiac arrest (SCA), heart attack, stroke, and foreign-body airway obstruction (FBAO); cardiopulmonary resuscitation (CPR); and defibrillation with an automated external defibrillator (AED)
, heart attack, stroke, and foreign-body airway obstruction (FBAO); cardiopulmonary resuscitation (CPR); and defibrillation with an automated external defibrillator (AED)")
4
American Heart Association uses 4 links in a chain -the “Chain of Survival” to illustrate the important time sensitive actions for victims of VF SCA. These links are Early recognition of the emergency and activation of local emergency response system Early bystander CPR: immediate CPR can double or triple the victim’s chance of survival from VF SCA. Early delivery of a shock with a defibrillator: CPR plus defibrillation within 3 to 5 minutes of collapse can produce survival rates as high as 49% to 75% Early advanced life support followed by postresuscitation care delivered by healthcare providers.

6
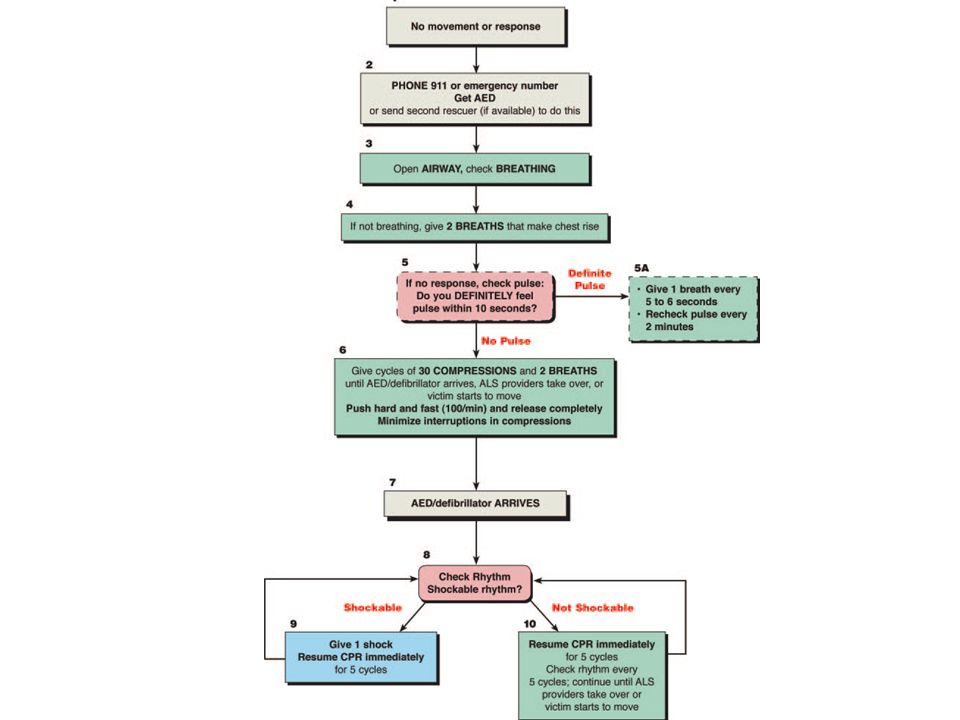
Adult BLS Sequence Steps of BLS consist of a series of sequential assessments and actions, which are illustrated in the BLS algorithm

8
Open the Airway: Lay Rescuer
Head tilt– chin lift maneuver for both injured and noninjured victims. The jaw thrust is no longer recommended for lay rescuers Is difficult for lay rescuers to learn and perform Is often not an effective way to open the airway May cause spinal movement

9
Open the Airway: Healthcare Provider
Head tilt– chin lift maneuver to open the airway of a victim without evidence of head or neck trauma. If cervical spine injury is suspected , open the airway using a jaw thrust without head extension Use a head tilt– chin lift maneuver if the jaw thrust does not open the airway

10
Basic airway management Head tilt and chin lift

11
Basic airway management Head tilt and chin lift

12
Basic airway management Jaw thrust

13
Check Breathing Look, listen, and feel for breathing.
Adequate breathing is not detected within 10 seconds, give 2 breaths If you are a lay rescuer and you are unwilling or unable to give rescue breaths, begin chest compressions . Treat the victim who has occasional gasps as if he or she is not breathing and give rescue breaths.

14
Give 2 rescue breaths, each over 1 second, with enough volume to produce visible chest rise.
recommendations for delivery of rescue breaths during cardiac arrest as follows Deliver each rescue breath over 1 second Give a sufficient tidal volume to produce visible chest rise Avoid rapid or forceful breaths. When an advanced airway (ie, endotracheal tube, Combitube, or LMA) is in place during 2-person CPR, ventilate at a rate of 8 to 10 breaths per minute without attempting to synchronize breaths between compressions
 is in place during 2-person CPR, ventilate at a rate of 8 to 10 breaths per minute without attempting to synchronize breaths between compressions.")
15
Mouth-to-Mouth Rescue Breathing
Open the victim’s airway Pinch the victim’s nose Create an airtight mouth-to-mouth seal. Give 1 breath over 1 second Take a “regular” (not a deep) breath Give a second rescue breath over 1 second Despite its safety, some may hesitate to give mouth-to-mouth rescue breathing and prefer to use a barrier device
 breath. Give a second rescue breath over 1 second. Despite its safety, some may hesitate to give mouth-to-mouth rescue breathing and prefer to use a barrier device.")
16
Mouth-to-Nose Ventilation
Recommended if it is impossible to ventilate through the victim’s mouth,mouth cannot be opened or a mouth-to-mouth seal is difficult to achieve Feasible, safe, and effective

17
Ventilation With Bag and Mask
Simultaneously open the airway with a jaw lift, hold the mask tightly against the patient’s face, and squeeze the bag. The rescuer must also watch to be sure the chest rises with each breath Most effective when provided by 2 trained and experienced rescuers Rescuer delivers the breaths during pauses in compressions and delivers each breath over 1 second

18
Ventilation With an Advanced Airway
Advanced airway devices such as the LMA and the esophageal-tracheal combitube are currently within the scope of BLS practice in a number of regions An advanced airway in place during CPR, 2 rescuers no longer deliver cycles of CPR . instead, The compressing rescuer should give continuous chest compressions at a rate of 100 per minute without pauses for ventilation. The rescuer delivering ventilation provides 8 to 10 breaths per minute. The 2 rescuers should change compressor and ventilator roles approximately every 2 minutes When multiple rescuers are present, they should rotate the compressor role about every 2 minutes.

19
Foreign-Body Airway Obstruction (Choking)
Recognition of airway obstruction is the key to successful outcome, it is important to distinguish this emergency If mild obstruction is present and the victim is coughing forcefully, do not interfere with the patient’s spontaneous coughing and breathing efforts Intervene if signs of severe obstruction develop The cough becomes silent Respiratory difficulty increases Accompanied by stridor The victim becomes unresponsive.

20
Chest thrusts, back slaps, and abdominal thrusts are feasible and effective for relieving severe FBAO in conscious (responsive) adults and children 1 year of age Abdominal thrust- applied in rapid sequence until the obstruction is relieved If abdominal thrusts are not effective, the rescuer may consider chest thrusts Abdominal thrusts are not recommended for infants < 1 year of age because thrusts may cause injuries

21
If victim with FBAO becomes unresponsive, the rescuer should carefully support the patient to the ground, immediately activate EMS and then begin CPR. Higher sustained airway pressures can be generated using the chest thrust rather than the abdominal thrust Each time the airway is opened during CPR, the rescuer should look for an object in the victim’s mouth and remove it Use a finger sweep only when the provider can see solid material obstructing the airway of an unresponsive patient (class indeterminate)
")
23
chest thrusts

24
chest thrusts

25
Foreign body airway obstruction (FBAO) abdominal thrusts
 abdominal thrusts")
26
Foreign body airway obstruction (FBAO) abdominal thrusts
 abdominal thrusts")
27
Foreign body airway obstruction (FBAO) back slaps
 back slaps")
28
Rescue Breathing Without Chest Compressions
If an adult victim with palpable pulses requires support of ventilation, give rescue breaths at a rate of 10 to 12 breaths per minute Reassess the pulse approximately every 2 minutes

29
Chest Compressions Chest compressions consist of rhythmic applications of pressure over the lower half of the sternum Blood flow generated by chest compressions delivers a small but critical amount of oxygen and substrate to the brain and myocardium In VF chest compressions increase the likelihood that an attempted defibrillation will be successful Chest compressions are especially important if the first shock is delivered 4 minutes after collapse

30
“Effective” chest compressions are essential for providing blood flow during CPR
to give “effective” chest compressions, “push hard and push fast.” Compress at a rate of about 100 compressions per minute, with a compression depth of 4 to 5 cm Allow chest to recoil completely after each compression, and allow approximately equal compression and relaxation times. Minimize interruptions in chest compressions.

31
Chest compressions

32
Chest compressions

33
Chest compressions

34
Chest compressions

35
Compression-Ventilation Ratio
A compression-ventilation ratio of 30:2 is recommended. In infants and children 2 rescuers should use a ratio of 15:2 Once an advanced airway is in place, 2 rescuers no longer deliver cycles of CPR CPR prompt device may be useful in improving quality of CPR

36
Compression-Only CPR Laypersons should be encouraged to do compression-only CPR if they are unable or unwilling to provide rescue breaths, although the best method of CPR is compressions coordinated with ventilations. Survival rates were better with chest compressions only than with no CPR. Rescue breathing is not essential during the first 5 minutes of adult CPR for VF. If the airway is open, occasional gasps and passive chest recoil may provide some air exchange. In addition, a low minute ventilation may be all that is necessary to maintain a normal ventilation-perfusion ratio during CPR.

37
Defibrillation Early defibrillation is critical to survival from sudden cardiac arrest (SCA) for several reasons: The most frequent initial rhythm in witnessed SCA is ventricular fibrillation (VF) The probability of successful defibrillation diminishes rapidly over time VF tends to deteriorate to asystole within a few minutes.
 The probability of successful defibrillation diminishes rapidly over time. VF tends to deteriorate to asystole within a few minutes.")
38
For every minute that passes between collapse and defibrillation, survival rates from witnessed VF SCA decrease 7% to 10% if no CPR is provided When bystander CPR is provided, the decrease in survival rates is more gradual and averages 3% to 4% per minute CPR can double or triple survival from witnessed SCA at most intervals to defibrillation. CPR prolongs VF(ie, the window of time during which defibrillation can occur) and provides a small amount of blood flow that may maintain some oxygen and substrate delivery to the heart and brain
 and provides a small amount of blood flow that may maintain some oxygen and substrate delivery to the heart and brain.")
39
Shock First Versus CPR First
When any rescuer witnesses an out-of-hospital arrest and an AED is immediately available on-site, the rescuer should use the AED as soon as possible Healthcare providers who treat cardiac arrest in hospitals and other facilities with AEDs on-site should provide immediate CPR and should use the AED/defibrillator as soon as it is available When an out-of-hospital cardiac arrest is not witnessed by EMS personnel, they may give about 5 cycles of CPR before checking the ECG rhythm and attempting defibrillation particularly when call-to-response interval is > 5 min.

40
When VF is present for more than a few minutes, the myocardium is depleted of oxygen and metabolic substrates. A brief period of chest compressions can deliver oxygen and energy substrates, increasing the likelihood that a perfusing rhythm will return after defibrillation

41
1-Shock Protocol Versus 3-Shock Sequence
Interruption in chest compressions is associated with a decreased probability of conversion of VF in the 3-shock sequence. Rhythm analysis of 3-shock sequence performed by commercially available AEDs revealed delays of up to 37 seconds between delivery of the first shock and delivery of the first post-shock compression Animal studies documented harmful effects from interruptions to chest compressions The rescuer should not delay resumption of chest compressions to recheck the rhythm or pulse. After 5 cycles (about 2 minutes) of CPR, the AED should then analyze the cardiac rhythm and deliver another shock if indicated.
 of CPR, the AED should then analyze the cardiac rhythm and deliver another shock if indicated.")
42
The rescuer providing chest compressions should minimize interruptions in chest compressions for rhythm analysis and shock delivery When 2 rescuers are present, the rescuer operating the AED should be prepared to deliver a shock as soon as the compressor removes his or her hands from the victim’s chest

43
Monophasic Waveform Defibrillators
deliver current of one polarity (ie,direction of current flow). Biphasic Waveform Defibrillators lower-energy biphasic waveform shocks have equivalent or higher success for termination of VF than monophasic waveform shocks delivering escalating energy (200 J, 300 J, 360 J) with successive shocks. it is reasonable to use selected energies of 150 J to 200 J with a biphasic truncated exponential waveform or 120 J with a rectilinear biphasic waveform for the initial shock.
. Biphasic Waveform Defibrillators. lower-energy biphasic waveform shocks have equivalent or higher success for termination of VF than monophasic waveform shocks delivering escalating energy (200 J, 300 J, 360 J) with successive shocks. it is reasonable to use selected energies of 150 J to 200 J with a biphasic truncated exponential waveform or 120 J with a rectilinear biphasic waveform for the initial shock.")
44
Automated External Defibrillators
AEDs are sophisticated, reliable computerized devices that use voice and visual prompts to guide lay rescuers and healthcare providers to safely defibrillate VF SCA Lay rescuer AED programs to improve survival rates from out-of-hospital SCA AEDs are of no value for arrest not caused by VF/pulseless VT, and they are not effective for treatment of nonshockable rhythms that may develop after termination of VF

46
Safe use of oxygen during defibrillation
Take off any oxygen mask/nasal cannulae & place them at least 1m away from the patient’s chest. Leave the ventilation bag connected to the tracheal tube or other airway adjunct. Alternatively, disconnect any bag-valve device from the tracheal tube (or other airway adjunct) and remove it at least 1m from the patient’s chest during defibrillation Minimise the risk of sparks during defibrillation. Self-adhesive defibrillation pads are less likely to cause sparks than manual paddles.
 and remove it at least 1m from the patient’s chest during defibrillation. Minimise the risk of sparks during defibrillation. Self-adhesive defibrillation pads are less likely to cause sparks than manual paddles.")
47
Electrode-patient interface
Transthoracic impedance (TTI)varies with body mass- approximately 70—80 Ω in adults To reduce transthoracic impedance, the defibrillator operator should use conductive materials Paddles should be well separated, and the paste or gel should not be smeared on the chest between the paddles Defibrillation for patients with permanent pacemakers or ICDs, do not place the electrodes over or close to the device generator Pacemakers and ICDs should be reevaluated after the patient receives a shock
varies with body mass- approximately 70—80 Ω in adults. To reduce transthoracic impedance, the defibrillator operator should use conductive materials. Paddles should be well separated, and the paste or gel should not be smeared on the chest between the paddles. Defibrillation for patients with permanent pacemakers or ICDs, do not place the electrodes over or close to the device generator. Pacemakers and ICDs should be reevaluated after the patient receives a shock.")
48
Paddle electrodes and self-adhesive pad electrodes 8 to 12 cm in diameter perform well, although defibrillation success may be higher with electrodes 12 cm in diameter rather than with those 8 cm in diameter

49
Electrode position

50
Pads versus paddles

51
No evidence that attempting to “defibrillate” asystole is beneficial
Studies revealed the group that received shocks showed a trend toward a worse outcome than the group that did not receive shocks. With recent recognition of the importance of minimizing interruptions in chest compressions, attempt shock delivery for asystole is not recommended

52
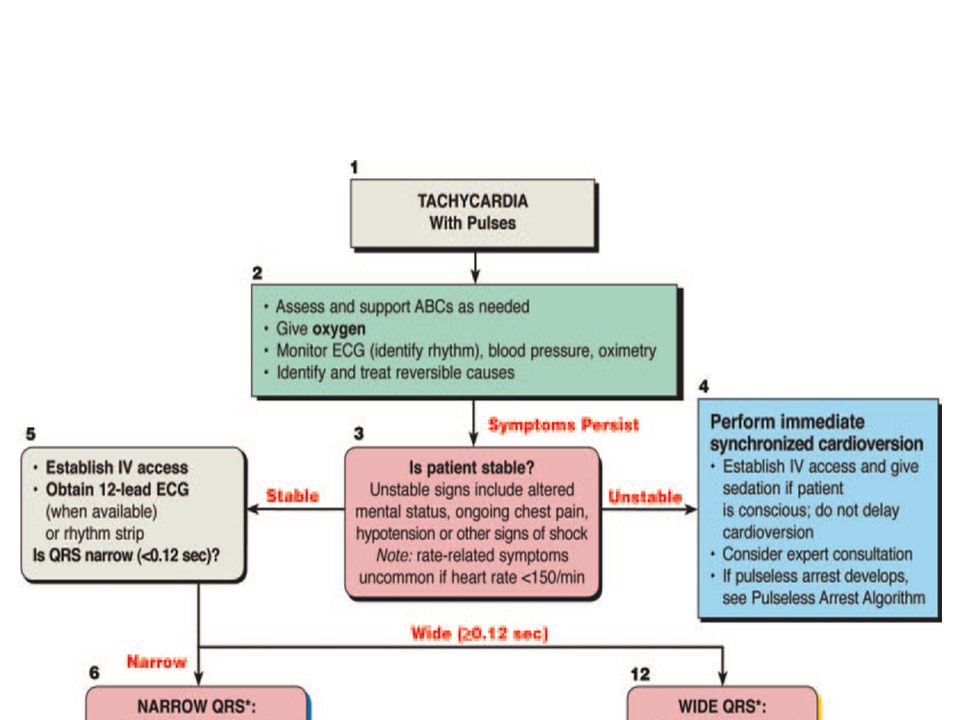
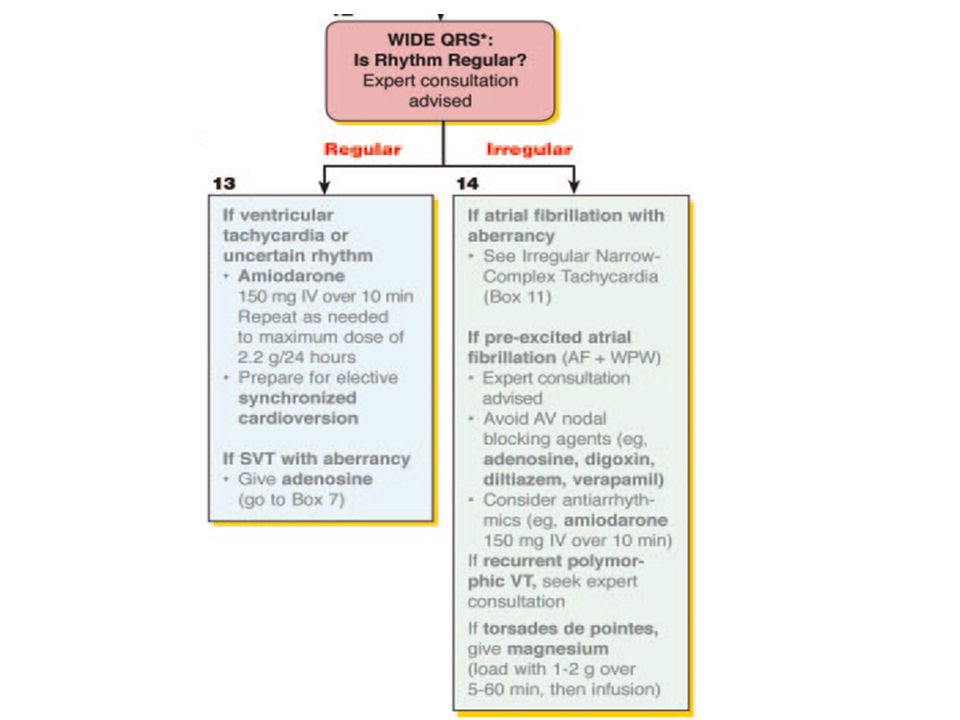
Synchronized Cardioversion
Synchronized cardioversion is shock delivery that is timed (synchronized) with the QRS complex Must be synchronised to occur with the R wave of the ECG rather than with the T wave: VF can be induced if shock is delivered during the relative refractory portion of the cardiac cycle. Synchronisation can be difficult in VT because of the wide-complex & variable forms of ventricular arrhythmia. If synchronisation fails, give unsynchronised shocks to the unstable patient in VT to avoid prolonged delay in restoring sinus rhythm. Ventricular fibrillation or pulseless VT requires unsynchronised shocks.
 with the QRS complex. Must be synchronised to occur with the R wave of the ECG rather than with the T wave: VF can be induced if shock is delivered during the relative refractory portion of the cardiac cycle. Synchronisation can be difficult in VT because of the wide-complex & variable forms of ventricular arrhythmia. If synchronisation fails, give unsynchronised shocks to the unstable patient in VT to avoid prolonged delay in restoring sinus rhythm. Ventricular fibrillation or pulseless VT requires unsynchronised shocks.")
53
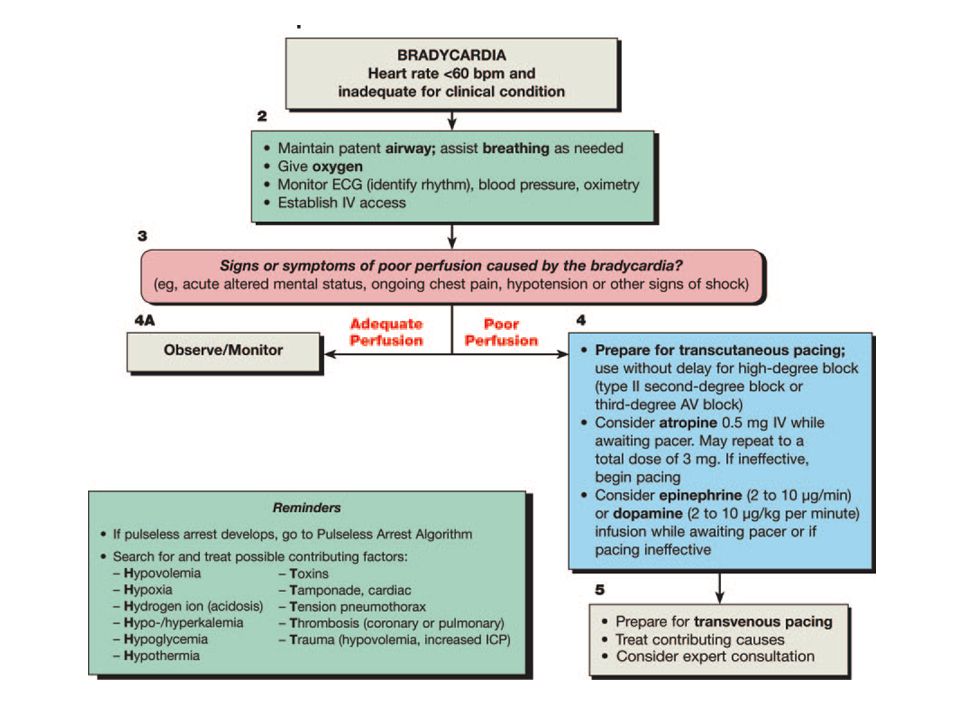
Pacing Pacing is not recommended for patients in asystolic cardiac arrest. Pacing can be considered in patients with symptomatic bradycardia.

55
Adult advanced life support
Advanced life support is aimed to revert cardiac rhythm to one that is hemodynamically effective,optimise ventilation,maintain and support circulation

58
Shockable rhythms (VF/pulseless VT)
If VF/VT is confirmed, give 1shock (150—200-J biphasic or 360-J monophasic). Without reassessing the rhythm or feeling for a pulse, resume CPR (30:2)immediately after the shock, starting with chest compressions.
. Without reassessing the rhythm or feeling for a pulse, resume CPR (30:2)immediately after the shock, starting with chest compressions.")
59
Continue CPR for 2 min, then pause briefly to check the monitor: if there is still VF/VT, give a second shock (150—360-J biphasic or 360-J monophasic). Resume CPR immediately after the second shock.

60
Pause briefly after 2 min of CPR to check monitor: if still VF/VT, → adrenaline followed immediately by a third shock (150—360-J biphasic or 360-J monophasic) and resumption of CPR (drug-shock-CPR-rhythm check sequence)
")
61
After drug delivery and 2 min of CPR, analyse rhythm.
If VF/VT persists after the third shock, give an IV bolus amiodarone 300 mg. Inject amiodarone during the brief rhythm analysis before delivery of the fourth shock.

62
Rhythm checked 2 min after a shock → nonshockable rhythm is present and the rhythm is organised (complexes appear regular or narrow), try to palpate a pulse. Rhythm checks must be brief, and pulse checks undertaken only if an organised rhythm is observed. If an organised rhythm is seen during a 2 min period of CPR, do not interrupt chest compressions to palpate a pulse unless the patient shows signs of life suggesting ROSC. If there is any doubt about the presence of a pulse in the presence of an organised rhythm, resume CPR. If the patient has ROSC, begin postresuscitation care.

63
Regardless of the arrest rhythm, give adrenaline 1mg every 3—5 min until ROSC is achieved
This will be once every two loops of the algorithm.

64
Persistent ventricular fibrillation
In VF persists, consider changing the position of the paddles. Review all potentially reversible causes and treat any that are identified.

65
Non-shockable rhythms (PEA and asystole)
Start CPR 30:2 and give adrenaline 1mg as soon as iv access is achieved Despite the lack of evidence that routine atropine for asystolic cardiac arrest increases survival, give atropine 3mg (the dose that will provide maximum vagal blockade) if there is asystole or the rhythm is slow PEA (rate <60 min−1)
 if there is asystole or the rhythm is slow PEA (rate <60 min−1)")
66
After 2 min of CPR, If no rhythm is present (asystole), or if there is no change in the ECG appearance, resume CPR immediately. If an organised rhythm is present, attempt to palpate a pulse. If no pulse (or if there is any doubt about the presence of a pulse), continue CPR. If signs of life return during CPR, check the rhythm and attempt to palpate a pulse If a pulse is present, begin post-resuscitation care.
, continue CPR. If signs of life return during CPR, check the rhythm and attempt to palpate a pulse. If a pulse is present, begin post-resuscitation care.")
67
If there is doubt about whether the rhythm is asystole or fine VF, do not attempt defibrillation; instead, continue chest compressions and ventilation. Fine VF that is difficult to distinguish from asystole will not be shocked successfully into a perfusing rhythm

68
Intravenous access and drugs

69
Central venous v/s Peripheral drug delivery
+peak drug concentrations are higher +circulation times are shorter -insertion of a CV catheter requires interruption CPR -is associated with several complications. +quicker, easier to perform and safer. -Drugs injected must be followed by a flush of at least 20 ml of fluid and elevation of the extremity for 10—20 s to facilitate drug delivery to the central circulation

70
Intraosseous route. Achieves adequate plasma concentrations in a time comparable with injection through a central venous catheter Also enables withdrawal of marrow for venous blood gas analysis and measurement of electrolytes & Hb concentration.

72
Tracheal route During CPR, the equipotent dose of adrenaline given via the trachea is 3-10 times ↑ than the IV dose If given via the trachea, adrenaline dose is 3mg diluted to at least 10 ml with sterile water. Dilution with water instead of 0.9% saline may achieve better drug absorption

77
Potentially reversible causes
Minimise the risk of hypoxia by ensuring that the patient’s lungs are ventilated adequately with 100% oxygen Hypovolemia-restore intravascular volume rapidly with fluid,coupled with urgent surgery Intravenous calcium chloride -hyperkalaemia, hypocalcaemia,calcium-channel-blocking drug overdose.

78
Tension pneumothorax-needle thoracocentesis,chest drain
Cardiac tamponade-needle pericardiocentesis, thoracotomy. Toxic substances-appropriate antidotes Thromboembolic -Thrombolysis may be considered in adult cardiac arrest, on a case-by-case basis, following initial failure of standard resuscitation in patients in whom an acute thrombotic etiology for the arrest is suspected. Intravenous fluids-initial stages of resuscitation there are no clear advantages to using colloid: use saline

79
Monitoring and Medications
Arterial blood gas monitoring-not a reliable indicator of the severity of tissue hypoxemia No clinical utility of checking pulses during ongoing CPR End-tidal CO2 monitoring is a safe and effective noninvasive indicator of cardiac output during CPR and may be an early indicator of ROSC in intubated patients

80
Postresuscitation Support
Optimize cardiopulmonary function and systemic perfusion,especially perfusion to the brain Transport the victim of out-of-hospital cardiac arrest to the hospital emergency department To identify the precipitating causes of the arrest Institute measures to prevent recurrence Institute measures that may improve long-term, neurologically intact survival

81
Induced Hypothermia-Unconscious adult patients with spontaneous circulation after out-of-hospital VF cardiac arrest should be cooled to 32-34°C for at least h. Glucose Control mmol/l using insulin Organ-Specific Evaluation and Support Mechanical ventilation

82
CPR Techniques and Devices
High-frequency chest compressions (HFCC) High-frequency (>100 compressions min−1) manual or mechanical chest compressions improve haemodynamics but have not been shown to improve longterm outcome.
 High-frequency (>100 compressions min−1) manual or mechanical chest compressions improve haemodynamics but have not been shown to improve longterm outcome.")
83
Interposed abdominal compression (IAC-CPR)
")
84
Open-chest CPR Open-chest CPR
for patients with cardiac arrest in the early postoperative period after cardiothoracic surgery when the chest or abdomen is already open

85
“Cough” CPR Not useful for the treatment of an unresponsive victim
Human “cough” CPR has been reported only in awake,monitored patients who developed ventricular fibrillation (VF) or rapid ventricular tachycardia Can maintain consciousness for up to 90 seconds.
 or rapid ventricular tachycardia. Can maintain consciousness for up to 90 seconds.")
86
Precordial thump Single precordial thump may be given for a witnessed and monitored sudden collapse, and a defibrillator is not immediately to hand. Should be undertaken immediately after confirmation of cardiac arrest Ulnar edge of a tightly clenched fist used to deliver a sharp impact to the lower half of the sternum from a height of about 20 cm, then retract immediatelymost likely May succeed in converting VT to sinus rhythm Successful treatment of VF by precordial thump is much less likely:

87
Active compression-decompression CPR (ACD-CPR)
")
88
Active compression-decompression CPR (ACD-CPR) is performed with a hand-held device equipped with a suction cup to actively lift the anterior chest during decompression. It is thought that decreasing intrathoracic pressure during the decompression phase enhances venous return to the heart May be considered for use in the in-hospital setting when providers are adequately trained (Class IIb).
.")
89
Impedance threshold device (ITD)
")
90
Valve that limits air entry into the lungs during chest recoil between chest compressions.
Designed to reduce intrathoracic pressure and enhance venous return to the heart. ITD as an adjunct to CPR in intubated adult cardiac arrest patients can improve hemodynamic parameters(Class IIa).
.")
91
Impedance threshold device (ITD)
")
92
Mechanical piston CPR

93
Mechanical piston CPR

94
Load-distributing band CPR or vest CPR
The load-distributing band (LDB) is a circumferential chest compression device composed of a pneumatically or electrically actuated constricting band and backboard
 is a circumferential chest compression device composed of a pneumatically or electrically actuated constricting band and backboard.")
95
Phased thoracic—abdominal compression—decompression CPR (PTACD-CPR)
Phased thoracic-abdominal compression-decompression CPR (PTACD-CPR) combines the concepts of IAC-CPR and ACD-CPR A hand-held device alternates chest compression and abdominal decompression with chest decompression and abdominal compression
 combines the concepts of IAC-CPR and ACD-CPR. A hand-held device alternates chest compression and abdominal decompression with chest decompression and abdominal compression.")
96
Cardiocerebral resuscitation (CCR)
Cardiocerebral resuscitation (CCR) represents a bundle of specific therapies designed to enhance perfusion during cardiopulmonary arrest by emphasizing chest compressions over ventilations and “priming” the heart with compressions before and after defibrillation attempts.
 represents a bundle of specific therapies designed to enhance perfusion during cardiopulmonary arrest by emphasizing chest compressions over ventilations and priming the heart with compressions before and after defibrillation attempts.")
98
Thank you

Similar presentations
















>")









