Download presentation
Presentation is loading. Please wait.

1
Surveillance Methodology and Economic Burden of SSIs
Maureen Spencer, RN, M.Ed, CIC Infection Preventionist Consultant Boston, MA - USA

2
Purpose of the Infection Control and Prevention Program
Surveillance – detect cases Control - outbreaks, clusters or increasing trends in data Implement prevention measures

3
Surveillance System and CDC Definitions

4
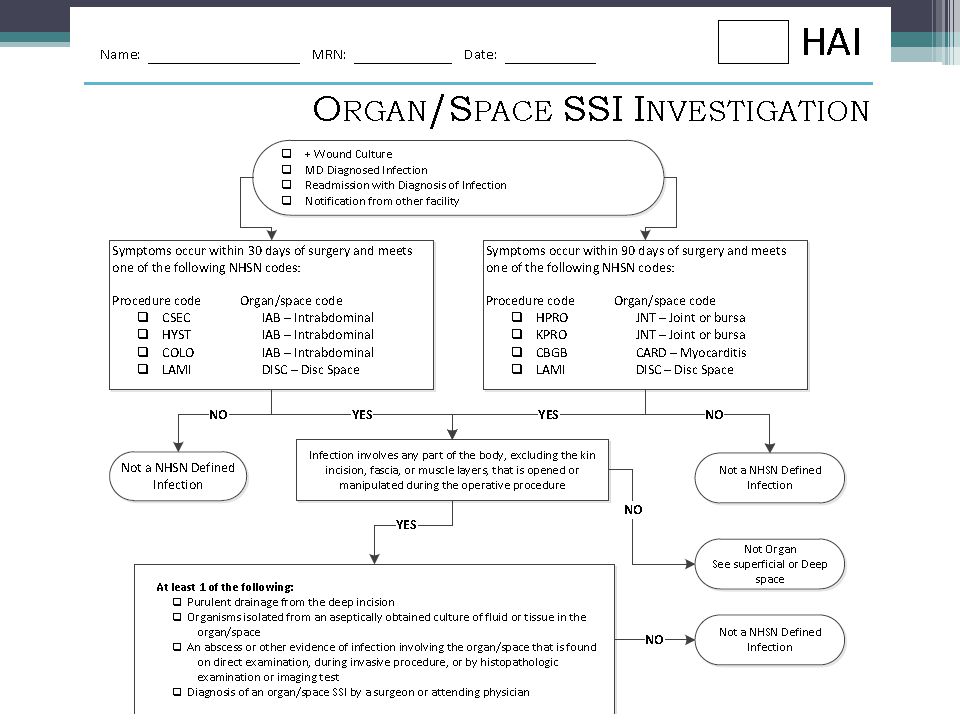
Developed Algorithms For Surveillance (Each Category)
")
5
Case definition Case definitions are designed to capture all potential cases of a disease/condition without contaminating the dataset with extraneous materials NHSN is, by definition, our basic service Special case definitions may be required for specific issues or for outbreaks

6
Case definitions Outbreak Case control studies
May want to date or unit define May want to include symptoms or manifestations Case control studies Permit selection of control group (those without the condition under study) Associated with the event or process
 Associated with the event or process.")
13
Data analysis Data are systematically compiled and interpreted
Data are analyzed using statistical methods Date are compared over time to internal and external databases Comparative databases are used when undesirable variation is identified

14
Numbers Numerator – the “top” number which is also the number of cases identified Denominator – the “bottom number” –(down below) is the total number of individuals studied Rate – the result of dividing the numerator by the denominator and multiplying by a factor
 is the total number of individuals studied. Rate – the result of dividing the numerator by the denominator and multiplying by a factor.")
15
The “Factor” There is no established “factor” for most statistical math in epidemiology Generally report surgical and other similar infection as x/100 events Generally report device related infections by device day x/1000 device days

16
Measures of occurrence
Incidence Measure of frequency with which an event occurs in a population over a specified period of time New cases Prevalence Proportion of persons in a population with a particular disease at a specific point in time (point prevalence) or over a specified time period (period prevalence) Existing cases
 or over a specified time period (period prevalence) Existing cases.")
17
Studies Case Control – two groups, identical, but one with the characteristic under study, and other without. General 1:3 (power) Cohort – all people in a group (enter together, and then observe for occurrence of disease/condition) Prospective – looking forward Retrospective – looking backward This slide for confidence intervals
 Prospective – looking forward. Retrospective – looking backward. This slide for confidence intervals.")
18
Bias Bias can be defined as “any systematic error in the design, conduct or analysis of a study that results in a mistaken estimate of an exposure’s effect on the risk of disease” Selection Bias Information Bias

19
The monthly record of cases
Record demographic data for each case Use consistent methods Column A: Last Name Column B: First Name Column C: Medical Record #Physician Physician name Physician identification # (check, as often there are two different numbers in the hospital) Age – useful in stratification Gender – equivocal data set Admission date (critical!) Onset date (used to calculate # hospital days admission to onset)
 Age – useful in stratification. Gender – equivocal data set. Admission date (critical!) Onset date (used to calculate # hospital days admission to onset)")
20
Line Listing Line List: A line list is an organized, detailed list of each record of a surgical site infection Example Suppose you are interested in looking at all CLABSIs in 2010 that occurred in the ICU and the Orthopedic Unit You would like to produce a line list that includes basic patient demographics (patient ID, DOB, gender, and age at event), information on the event (date admitted, date of surgey, date of onset, location of patient when SSI developed
, information on the event (date admitted, date of surgey, date of onset, location of patient when SSI developed.")
21
Line list heading – Depends on the HAI
Infection site Use standard nomenclature - NHSN SSI SST CAUTI Procedure codes Procedure date Surgeon code Surgeon assistant and others in the room Date of Admission Date of Onset of Infection Antibiotics ASA score Incision time Closure time Patient room number

22
Next columns Organism Culture site
Use standard nomenclature! CNS vs. Coag neg staph vs. S. epidermidis Spell the words correctly Culture site Final attribution – Hosp Onset, Comm Onset, Comm Acquired Comment field– generally cannot sort by anything except the first word but useful for keeping notes

23
Frequency Table Frequency Table: A frequency table is an organized display of counts and percentages The data are organized by a row variable and a column variable, and the frequency table provides a count of the number of observations in the data set that meet the specifications of both the row and column variables Example Suppose you are interested in looking at the distribution of each SSI across the different services in your facility, for all events that were identified in 2012

24
EXAMPLE OF HAI FREQUENCY TABLE IN EXCEL FILE
UHS HAI Dashboard

26
Descriptive Epidemiology
Cross tabulations: infections/organisms infections/nursing units infections/services infections/risk factors Evaluate trends and clusters Conduct studies and investigations Retrospective case reviews, Case-Control Studies

27
Examples of Cross Tabulations
CLABSI by ICUs CLABSI by device type CLABSI by organisms SSIs by services SSIs by surgeons SSIs by nursing unit Risk factors by SSIs SSI rates over a time period

28
SSI by Service - 2012 SERVICE CABG TOTAL HIP TOTAL KNEE ABD HYSTEC
COLON Gen Surgery 4 Cardiac Surgery 2 Orthopedic Surgery 3 Gynecology Surgery

29
Example CLABSI Analysis 2011-2012
Nursing Unit 2011 (n=13) 2012 (n = 4) SICU 34 24 NICU 3 1 PICU 2 MICU 42 4 WEST 5 SOUTH 16 23 What do these numerators mean? Next calculate rates by line days
 2012 (n = 4) SICU NICU PICU. 2. MICU WEST. 5 SOUTH What do these numerators mean Next calculate rates by line days.")
30
CLABSI BY ORGANISMS - 2012 5 8 2 1 4 10 12 6 23 14 7 SICU NICU PICU
NURS UNIT STAPH AUREUS MRSA CNS ALPHA STREP ECOLI PSEUD AERUG CANDIDA SICU 5 8 2 1 4 NICU PICU MICU 10 12 4 WEST 5 SOUTH 6 TOTALS 23 14 7

31
SSI RATES TYPE OF SURGERY # SSIs # PROCEDURES % RATE THA 2 100 2% TKA
3 75 4% CABG 25 8% COLON 4 15 27% ABD HYSTERCTOMY 16 19%

32
SSIs BY SURGEONS - RATES
CODE CABG TKA THA COLON ABD HYSTER A 1.2 B 1.0 C 0.9 D 0.4 0.8 E 0.0 F 5.6 G 4.8 H 0.0 (0/6 cases) I 30.0 (3/10 cases)
 I (3/10 cases)")
33
Risk Factors for Infections
Surgery Diabetes Obese (BMI > 30) Hema-toma Drains Staples Smoking Steroids THA 50% 75% 25% 90% 20% 10% TKA 60% 80% 35% 85% 95% 5% CABG 70% 0% 45% COLON ABD HYSTER ? What percentage of non-infected patients had risk factors ? What percentage of Surgeon I patients had these risk factors Obesity diabetes risk factors at this institution Staples are used often which may be increasing the risk Drains being used in orthopedic surgery – increase risk
 Hema-toma. Drains. Staples. Smoking. Steroids. THA. 50% 75% 25% 90% 20% 10% TKA. 60% 80% 35% 85% 95% 5% CABG. 70% 0% 45% COLON. ABD HYSTER. What percentage of non-infected patients had risk factors. What percentage of Surgeon I patients had these risk factors. Obesity diabetes risk factors at this institution. Staples are used often which may be increasing the risk. Drains being used in orthopedic surgery – increase risk.")
34
Pie Chart Pie Chart: A pie chart is a graphical representation of data. The different slices of the pie represent different values of a variable, with the relative size of the slice representing the amount of data included in the slice

35
Pie Chart Example The top value for each slice is the value of the “chart variable” (e.g., location). The second value is a count of the number of events included in each slice of the pie Example: Distribution of HAIs

36
Bar Chart Bar Chart: A bar chart is a graphical representation of data where the length or height of the bars represents counts of cases or rates

37
Number of Cases by Surgery Date

38
Days from Surgery to Infection - HPRO & KPRO

39
Orthopedic Surgical Site Infection Rates
OR Environmental controls: Traffic, Attire,Scrub, Air Handling Antibacterial sutures MRSA and Staph aureus Elimination Program CHG/Alcohol Prep Laminectomy outbreak due to locally administered steroids (depomedrol) 7 x increase risk of infection if obese and diabetic Increase in hematomas after use of Lovenox and Plavix
 7 x increase risk of infection if obese and diabetic. Increase in hematomas after use of Lovenox and Plavix.")
40
NEBH SSI Rates 2003 – 2010 (outpatient and inpatient infections)
Total hip investigation – increase in post-op hematomas in infected patients being evaluated by a case-control study 2008 – Total knee investigation – noticed increase rate in patients receiving toradol, marcaine and duromorph – needle on syringe was not being changed between each vial – changed practice 2007 – Laminectomy rate increased – case control study revealed locally adminiistered steroids increased infection rate in obese/diabetic pts 40

41
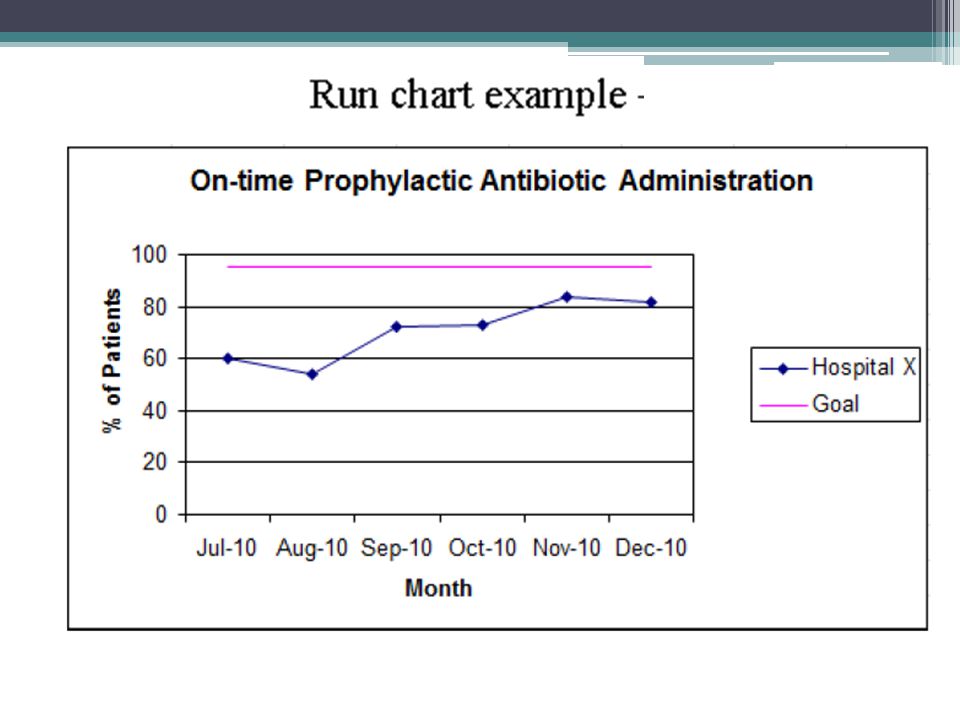
Run Chart Run Chart: A run chart (or control chart) is a line graph showing change in a variable over a selected time period This is a useful output if you would like to view, for example, the change in rates over time and 2 standard deviation above the mean

42
Instituted AMD Gauze and Standardized dressing technique
MRSA/MSSA Eradication Program Instituted AMD Gauze and Standardized dressing technique

43
Standardized Infection Ratio (SIR)
Standardized Infection Ratio (SIR), a statistic used to measure relative difference in HAI occurrence during a reporting period compared to a common referent period (i.e., standard population). SIR compares the actual number of HAIs with the predicted number based on the baseline U.S. experience (i.e., standard population), adjusting for several risk factors that have been found to be most associated with differences in infection rates
, a statistic used to measure relative difference in HAI occurrence during a reporting period compared to a common referent period (i.e., standard population). SIR compares the actual number of HAIs with the predicted number based on the baseline U.S. experience (i.e., standard population), adjusting for several risk factors that have been found to be most associated with differences in infection rates.")
44
Next Step: Calculate SIR by HAI by facility and compare to national data from NHSN

45
The “p” value The p value is the probability that an event will occur in a given set of trials A p of 1 means it will occur every time the trial occurs (if there were 100 “z” in a pile of 100 scrabble tiles, the probability of getting a “z” is 1 “by chance” Thus, a p of 0.05 means that 95% of the time or 95/100 you will not get a “z” if there were a random mix of tiles with only one z

46
Risk Factors for SSI MEDICAL
Patient-associated risk factors identified by studies in Malaysia and Vietnam Country Source Risk variable Surgical procedure Risk estimate (95% CI) P value Malaysia Praveen 20091 Intra-operative adhesions Inguinal hernioplasty Not reported 0.013 Post-operation haematoma 0.001 Yong 20012 Type 2 diabetes Total hip replacement OR 21.4 (1.53, 300.2) 0.023 Obesity OR 20.2 (2.13, 191.5) 0.009 Vietnam Nguyen 20013 Dirty wound Any surgical procedure OR 5.67 (1.92, 16.74) 0.002 Sohn 20024 OR 2.92 (1.35, 6.15) NR Thu 20055 All orthopaedic surgery OR 8.7 (4.55, 16.44) <0.001 ASA > 2 OR 3.9 (1.77, 8.82) 1. Praveen S et al. Asian J Surg (1): Yong KS, et al. Med J Malays Suppl C:57-60. 3. Nguyen D et al. Infect Control Hosp Epidemiol (8): Sohn AH et al. Infect Control Hosp Epidemiol (7): 5. Thu LTA et al. J Hosp Infect (4): MEDICAL
 P value. Malaysia. Praveen Intra-operative adhesions. Inguinal hernioplasty. Not reported Post-operation haematoma Yong Type 2 diabetes. Total hip replacement. OR 21.4 (1.53, 300.2) Obesity. OR 20.2 (2.13, 191.5) Vietnam. Nguyen Dirty wound. Any surgical procedure. OR 5.67 (1.92, 16.74) Sohn OR 2.92 (1.35, 6.15) NR. Thu All orthopaedic surgery. OR 8.7 (4.55, 16.44) < ASA > 2. OR 3.9 (1.77, 8.82) 1. Praveen S et al. Asian J Surg (1): Yong KS, et al. Med J Malays Suppl C: Nguyen D et al. Infect Control Hosp Epidemiol (8): Sohn AH et al. Infect Control Hosp Epidemiol (7): Thu LTA et al. J Hosp Infect (4): MEDICAL.")
47
Surgical site infection
SSI classification by surgical procedure 1 2 3 4 5 6 7 8 1. Duerink DO et al. J Hosp Infect (2): Sohn AH et al. Infect Control Hosp Epidemiol (7): 3. Praveen S et al. Asian J Surg (1): Dhillon KS et al. Med J Malays (3): 5. Syahrizal AB et al. Med J Malays Suppl D: Yang K et al. J Arthroplasty (1): 7. Kehachindawat P et al. J Med Assoc Thai 2007;90(7): Thu LTA et al. Infect Control Hosp Epidemiol (8): MEDICAL
: Sohn AH et al. Infect Control Hosp Epidemiol (7): Praveen S et al. Asian J Surg (1): Dhillon KS et al. Med J Malays (3): Syahrizal AB et al. Med J Malays Suppl D: Yang K et al. J Arthroplasty (1): Kehachindawat P et al. J Med Assoc Thai 2007;90(7): Thu LTA et al. Infect Control Hosp Epidemiol (8): MEDICAL.")
48
Incidence of ssi MEDICAL Gastrointestinal surgery
Country Source Surgical procedure Incidence (%) Malaysia Mahadeva 20091 Percutaneous endoscopic gastrostomy 33/103 (32%) Thambidorai 20082 Appendectomy in children Open: 34/61(55.7%) Laparoscopic: 3/51 (5.9%) Mahadeva S et al. Int J Clin Pract (5): Thambidorai CR et al. Singapore Med J (12): MEDICAL
 Malaysia. Mahadeva Percutaneous endoscopic gastrostomy. 33/103 (32%) Thambidorai Appendectomy in children. Open: 34/61(55.7%) Laparoscopic: 3/51 (5.9%) Mahadeva S et al. Int J Clin Pract (5): Thambidorai CR et al. Singapore Med J (12): MEDICAL.")
49
Incidence of ssi MEDICAL Orthopaedic surgery Incidence of SSI: 4 – 15%
Country Source Surgical procedure Incidence (%) Malaysia Dhillon 19951 All orthopaedic surgery 48/703 (6.8%) Syahrizal 20012 Total knee arthroplasty 11/100 (11.0%) Tay 20003 Total hip arthroplasty 10/109 (9.2%) Dhillon KS et al. Med J Malays (3): Syahrizal AB et al. Med J Malays Suppl D:5-8. Tay BH et al. Med J Malays Suppl C:74-85. MEDICAL
 Malaysia. Dhillon All orthopaedic surgery. 48/703 (6.8%) Syahrizal Total knee arthroplasty. 11/100 (11.0%) Tay Total hip arthroplasty. 10/109 (9.2%) Dhillon KS et al. Med J Malays (3): Syahrizal AB et al. Med J Malays Suppl D:5-8. Tay BH et al. Med J Malays Suppl C: MEDICAL.")
50
Incidence of ssi MEDICAL Gynaecology & Obstetrics surgery
Country Source Surgical procedure Incidence (%) Malaysia Huam 19971 Caesarean section Antibiotic prophylaxis: 3/100 (3.0%) No prophylaxis: 13/100 (13.0%) Ramli 20092 Laparoscopic ovarian cystectomy 2/ (5.4%) Huam SH et al. Med J Malays (1):3-7. Ramli R et al. Int Med J (4): MEDICAL
 Malaysia. Huam Caesarean section. Antibiotic prophylaxis: 3/100. (3.0%) No prophylaxis: 13/100 (13.0%) Ramli Laparoscopic ovarian cystectomy. 2/37 (5.4%) Huam SH et al. Med J Malays (1):3-7. Ramli R et al. Int Med J (4): MEDICAL.")
51
Incidence of SSI MEDICAL Other surgical procedures Country Source
Malaysia Ahmad 19971 Free flap surgery 10/ (16.4%) Hisham 20012 Total thyroidectomy 3/ (3.1%) Ng 20043 CABG 34/ (2.1%) Praveen 20094 Inguinal hernioplasty 15/ (7.4%) Ahmad TS et al. Ann Acad Med Singapore (6): Hisham AN et al. ANZ J Surg (4): Ng CY et al. Asian Cardiovasc Thorac Ann (3): Praveen S et al. Asian J Surg (1):59-63. MEDICAL
 Hisham Total thyroidectomy. 3/98 (3.1%) Ng CABG. 34/1594 (2.1%) Praveen Inguinal hernioplasty. 15/202 (7.4%) Ahmad TS et al. Ann Acad Med Singapore (6): Hisham AN et al. ANZ J Surg (4): Ng CY et al. Asian Cardiovasc Thorac Ann (3): Praveen S et al. Asian J Surg (1): MEDICAL.")
52
Quality Process Tools for Infection Prevention

54
Peri-operative Team Factors Care Delivery problems (CDPs)
SSI Fishbone Diagram Patient Factors Surgeon Technique Work Environmental Factors Pre-operative Factors Peri-operative Team Factors Organizational and Management Factors Care Delivery problems (CDPs) Lack of traffic control – too many in room Contaminated environment Lack of hand hygiene Financial constraints Improper surgical hand antisepsis Patient body colonization Poor communication among team Inadequate surgical prophylaxis Poor leadership Improper surgical attire Lack of pre-op shower Increase hospitalization days Surgical irrigation Unsterile instruments Non-coated sutures Use of Staples or steri-strips MRSA or MSSA nasal colonization Obese Poor staff levels Lack of discontinuation of antibiotics at 24 hrs Use of Drains Infection at another site The fishbone is often used in root cause analysis and provides a systematic frame work to work through all the potential factors that may have contributed to the situation. If you have been to the Dept of Pediatrics M&M you have seen this used Diabetic Poor surgical technique Workload and shift patterns Smoker Contamination of incision post-op Lack of re-dosing of antibiotic Contaminated environment Immunosuppressive agents Design, availability and maintenance of equipment Environment and physical plant problems (air handling system) Inadequate staffing for post-op care Lack of hand hygiene Lack of foley catheter removal within 48 hrs
 Lack of traffic control – too many in room. Contaminated environment. Lack of hand hygiene. Financial constraints. Improper surgical hand antisepsis. Patient body colonization. Poor communication among team. Inadequate surgical prophylaxis. Poor leadership. Improper surgical attire. Lack of pre-op shower. Increase hospitalization days. Surgical irrigation. Unsterile instruments. Non-coated sutures. Use of Staples or steri-strips. MRSA or MSSA nasal colonization. Obese. Poor staff levels. Lack of discontinuation of antibiotics at 24 hrs. Use of Drains. Infection at another site. The fishbone is often used in root cause analysis and provides a systematic frame work to work through all the potential factors that may have contributed to the situation. If you have been to the Dept of Pediatrics M&M you have seen this used. Diabetic. Poor surgical technique. Workload and shift patterns. Smoker. Contamination of incision post-op. Lack of re-dosing of antibiotic. Contaminated environment. Immunosuppressive agents. Design, availability and maintenance of equipment. Environment and physical plant problems (air handling system) Inadequate staffing for post-op care. Lack of hand hygiene. Lack of foley catheter removal within 48 hrs.")
55
How Much Do These Infections Cost???

56
Relative Economic Burden Associated with HAIs
Est. Annual # of Infections Direct Cost per Patient (2007$) Avg. Increased Length of Stay Attributable Mortality SSI Surgical Site Infections CLA-BSI Central-Line Associated Blood Stream Infections VAP Ventilator Associated Pneumonia CA-UTI Catheter-Associated Urinary Tract Infections Other / MDROs* Multi-Drug Resistant Organisms (e.g., MRSA, C. difficile, VRE, etc.) 290,485 (~17% of HAIs) 248,678 (~14% of HAIs) 250,205 (~15% of HAIs) 561,667 (~32% of HAIs) 386,090 (~22% of HAIs) $34,670 $29,156 $28,508 $1, ~$30,000 ~12 days ~10-24 days ~9-13 days 1 day ~9.1 days 4% 26% 24% 1% ~4% * NOTE: MDRO often cause other infection types (e.g., SSI, BSI, VAP, UTI); MDRO statistics reflect CDC estimates for methicillin-resistant Staphylococcus aureus (MRSA) only. SOURCES: Klevens, et al., “Estimating Health Care-Associated Infections and Deaths in U.S. Hospitals, 2002,” Public Health Review, 2007; CDC: “The Direct Medical Cost of HAIs in U.S. Hospitals and the Benefits of Prevention”, March 2009; Kirkland, et al., “The Impact of Surgical Site Infections”, Infect Control Hosp Epidemiol, 1999; Arch Internal Med, 1988; Arch Internal Med, 1974; Infect Control Hosp Epidemiol, 2002; CareFusion MedMined Analysis, 2009. 56
 Avg. Increased Length of Stay. Attributable Mortality. SSI Surgical Site Infections. CLA-BSI Central-Line Associated Blood Stream Infections. VAP Ventilator Associated Pneumonia. CA-UTI Catheter-Associated Urinary Tract Infections. Other / MDROs* Multi-Drug Resistant Organisms (e.g., MRSA, C. difficile, VRE, etc.) 290,485 (~17% of HAIs) 248,678 (~14% of HAIs) 250,205 (~15% of HAIs) 561,667 (~32% of HAIs) 386,090. (~22% of HAIs) $34,670. $29,156. $28,508. $1,007 ~$30,000. ~12 days. ~10-24 days. ~9-13 days. 1 day ~9.1 days. 4% 26% 24% 1% ~4% * NOTE: MDRO often cause other infection types (e.g., SSI, BSI, VAP, UTI); MDRO statistics reflect CDC estimates for methicillin-resistant Staphylococcus aureus (MRSA) only. SOURCES: Klevens, et al., Estimating Health Care-Associated Infections and Deaths in U.S. Hospitals, 2002, Public Health Review, 2007; CDC: The Direct Medical Cost of HAIs in U.S. Hospitals and the Benefits of Prevention , March 2009; Kirkland, et al., The Impact of Surgical Site Infections , Infect Control Hosp Epidemiol, 1999; Arch Internal Med, 1988; Arch Internal Med, 1974; Infect Control Hosp Epidemiol, 2002; CareFusion MedMined Analysis,")
57
Economic burden of SSI MEDICAL
Extended hospital stay associated with SSI In Vietnam, SSI is associated with an increase in hospital stay of 7-19 days Country Source Surgical procedure Type of stay Length of stay (days) SSI No SSI Difference P value Vietnam Nguyen 20011 Any surgical procedure Total stay 14 (SD: 10.8) 9.1 (SD: 7.1) 4.9 <0.001 Sohn 20022 Post-operative 26 10 16 <0.0001 Thu 20053 All orthopaedic surgery 28.1 9 19.1 Thu 20064 Orthopaedic surgery 21 15 Neurosurgery 27 17 Thu 20075 7 NR 1. Nguyen D et al. Infect Control Hosp Epidemiol (8): Sohn AH et al. Infect Control Hosp Epidemiol (7): 3. Thu LTA et al. J Hosp Infect (4): Thu LTA et al. Infect Control Hosp Epidemiol (8): 5. Thu LTA et al. Infect Control Hosp Epidemiol (5): MEDICAL
 SSI. No SSI. Difference. P value. Vietnam. Nguyen Any surgical procedure. Total stay. 14 (SD: 10.8) 9.1 (SD: 7.1) 4.9. < Sohn Post-operative < Thu All orthopaedic surgery Thu Orthopaedic surgery Neurosurgery Thu NR. 1. Nguyen D et al. Infect Control Hosp Epidemiol (8): Sohn AH et al. Infect Control Hosp Epidemiol (7): Thu LTA et al. J Hosp Infect (4): Thu LTA et al. Infect Control Hosp Epidemiol (8): Thu LTA et al. Infect Control Hosp Epidemiol (5): MEDICAL.")
58
Economic cost of ssi MEDICAL
In Thailand, SSI is associated with an increase in hospital stay of 7-19 days Source Surgical procedure Type of stay Length of stay (days) SSI no SSI Difference P value Danchaivijitr 20051 Any surgical procedure Post-operative stay NS 12.6 Kasatpibal 20052 Craniotomy 48.0 16.8 31.2 <0.0001 Colectomy 27.4 8.7 18.7 0.0001 Cholecystectomy 16.7 8.1 8.6 0.0147 Appendectomy 17.2 4.2 13.0 Mastectomy 20.5 9.8 10.7 0.0038 Herniorrhaphy 2.0 11.0 Lohsiriwat 20093 Colorectal surgery Hospital stay 15.9 8.3 7.6 <0.001 1. Danchaivijitr S et al. J Med Assoc of Thailand 2005;88 Suppl 10:S75-S Kasatpibal N et al. J Med Assoc of Thailand 2005;88(8): 3. Lohsiriwat V et al. J Med Assoc of Thailand 2009;92(1):12-6. MEDICAL
 SSI. no SSI. Difference. P value. Danchaivijitr Any surgical procedure. Post-operative stay. NS Kasatpibal Craniotomy < Colectomy Cholecystectomy Appendectomy Mastectomy Herniorrhaphy Lohsiriwat Colorectal surgery. Hospital stay < Danchaivijitr S et al. J Med Assoc of Thailand 2005;88 Suppl 10:S75-S Kasatpibal N et al. J Med Assoc of Thailand 2005;88(8): Lohsiriwat V et al. J Med Assoc of Thailand 2009;92(1):12-6. MEDICAL.")
59
Mean hospitalization cost (THB)
Economic cost of ssi Hospitalization cost associated with SSI in Thailand Surgical procedure Mean hospitalization cost (THB) SSI no SSI Difference P value Craniotomy 117,135 50,018 67,116 <0.0001 Colectomy 69,958 27,642 42,316 0.0170 Cholecystectomy 52,975 22,812 30,163 0.0341 Appendectomy 27,647 8,482 19,165 0.0004 Mastectomy 23,413 16,699 6,713 0.1449 Herniorrhaphy 17,801 6,882 10,919 0.0007 All 6 procedures 75,544 31,886 43,658 Source: Kasatpibal N et al. J Med Assoc of Thailand 2005;88(8): MEDICAL
 SSI. no SSI. Difference. P value. Craniotomy. 117, , ,116. < Colectomy. 69, , , Cholecystectomy. 52, , , Appendectomy. 27,647. 8, , Mastectomy. 23, ,699. 6, Herniorrhaphy. 17,801. 6, , All 6 procedures. 75, , ,658. Source: Kasatpibal N et al. J Med Assoc of Thailand 2005;88(8): MEDICAL.")
60
Edmiston, et al. APIC June 2012

61
Plus Antibacterial Sutures
One year prospective study of 3789 total joints In July 2005, implemented a full-year evaluation of antibacterial sutures usage in an orthopedic setting Changed product over July 4th holiday and did not tell all surgeons (only those involved with study) At the end of the year-long trial period: 45% reduction in SSIs caused by Staph aureus and MRSA Reduction in total joint infections rate during trial period Infection rate dropped from 0.44% to 0.33% with three less infections NAON Poster Presentation Spencer M, et al: Reducing the Risk of Orthopedic Infections: The Role of Innovative Suture Technology
 At the end of the year-long trial period: 45% reduction in SSIs caused by Staph aureus and MRSA. Reduction in total joint infections rate during trial period. Infection rate dropped from 0.44% to 0.33% with three less infections. NAON Poster Presentation Spencer M, et al: Reducing the Risk of Orthopedic Infections: The Role of Innovative Suture Technology.")
62
Three Less Staph Aureus Infections
Incremental cost: $ 3 x $40,000 Sensitive Staph aureus = $120,000 3 x $100,000 MRSA = $300,000 UHS – to convert a 25 hospital system will increase the budget by 1% or $35,000

63
NEBH SSI Rates 2003 – 2010 (outpatient and inpatient infections)
Total hip investigation – increase in post-op hematomas in infected patients being evaluated by a case-control study 2008 – Total knee investigation – noticed increase rate in patients receiving toradol, marcaine and duromorph – needle on syringe was not being changed between each vial – changed practice 2007 – Laminectomy rate increased – case control study revealed locally adminiistered steroids increased infection rate in obese/diabetic pts 63

64
Potential Savings Orthopedic Surgical Site Infections
Cost: ~ $25,000/each FY03 – 63/8837 cases (0.7%) million FY04 – 60/9669 cases (0.6%) 1.5 million FY05 – 49/9216 cases (0.5%) 1.2 million FY06 – 46/8986 cases (0.5%) 1.1 million FY /9027 cases (0.4%) $975,000 FY /8884 cases (0.4%) $925,000 64 64
 1.6 million. FY04 – 60/9669 cases (0.6%) 1.5 million. FY05 – 49/9216 cases (0.5%) 1.2 million. FY06 – 46/8986 cases (0.5%) 1.1 million. FY /9027 cases (0.4%) $975,000. FY /8884 cases (0.4%) $925,")
65
First Year Potential Cost Savings
UHS Healthcare-Acquired Infections 2010 2011 (through October) % Rate Reduction UHS 2011 Benchmark Rate # HAIs Reduced Potential Cost Savings Catheter Associated UTI (rate per Foley days) 1.39 0.64 54% 0.2 97 $90,630 CLABSI rate by catheter days) 1.44 0.66 0.0 59 $1,486,956 VAP (rate by ventilator days) 1.41 0.91 35% 47 $912,256 CABG SSI (overall rate by surgical procedures) 0.71 0.20 73% 4 $138,680 Total Hip (overall rate by surgical procedures) 0.73 0.53 27% 6 $208,020 Total Knee (overall rate by surgical procedures) 0.57 0% 12 $416,040 C.Difficile (rate per 10,000 patient days) 3.23 2.41 25% 7.0 150 $948,900 MRSA (rate per 1,000 patient days) 0.36 0.14 61% 0.4 252 $7,560,000 Total 627 $11,761,482
 % Rate Reduction. UHS 2011 Benchmark Rate. # HAIs. Reduced. Potential Cost Savings. Catheter Associated UTI (rate per Foley days) % $90,630. CLABSI rate by catheter days) $1,486,956. VAP (rate by ventilator days) % 47. $912,256. CABG SSI (overall rate by surgical procedures) % 4. $138,680. Total Hip (overall rate by surgical procedures) % 6. $208,020. Total Knee (overall rate by surgical procedures) % 12. $416,040. C.Difficile (rate per 10,000 patient days) % $948,900. MRSA (rate per 1,000 patient days) % $7,560,000. Total $11,761,482.")
66
Healthcare Acquired Infections
% Reduction UHS 2012 Benchmark Rate Infection Prevention Measures in Process Catheter Associated UTI (rate per Foley days) 57% 0.0 Infection Control Foley Catheter Tray and Silver Foley Catheter, CHG washcloths CLABSI (rate by catheter days) 54% Central Line Insertion Kits, Alcohol Caps for Injection Hub Protection, CHG washcloths, Central Line Checklist VAP (rate by ventilator days) 11% CHG rinse with oral care kits, VAP bundle checklist, CHG washcloths, nebulizer cleaning procedures, VAP rounds CABG SSI (overall rate by surgical procedures) 71% MRSA screening before surgery, CHG preop showers/cloths , Incisional sealants, CHG/alcohol skin prep Total Hip (overall rate by surgical procedures) 15% Total Knee (overall rate by surgical procedures) 50% C.Difficile (rate per 10,000 patient days) 12% 4.0/10,000 patient days Bleach wipes and bleach disinfectant solution, Rapid PCR Diagnostics for Early Diagnosis and Precautions, Enhanced environmental cleaning, cubicle curtain changes, room decontamination units for high rates MRSA (rate per 1,000 patient days) 62% 0.4 CHG Washcloths, Pre-admission and Pre-op Screening, Rapid PCR Diagnostics for Early Diagnosis and Precautions
 57% 0.0. Infection Control Foley Catheter Tray and Silver Foley Catheter, CHG washcloths. CLABSI. (rate by catheter days) 54% Central Line Insertion Kits, Alcohol Caps for Injection Hub Protection, CHG washcloths, Central Line Checklist. VAP (rate by ventilator days) 11% CHG rinse with oral care kits, VAP bundle checklist, CHG washcloths, nebulizer cleaning procedures, VAP rounds. CABG SSI (overall rate by surgical procedures) 71% MRSA screening before surgery, CHG preop showers/cloths , Incisional sealants, CHG/alcohol skin prep. Total Hip (overall rate by surgical procedures) 15% Total Knee (overall rate by surgical procedures) 50% C.Difficile (rate per 10,000 patient days) 12% 4.0/10,000 patient days. Bleach wipes and bleach disinfectant solution, Rapid PCR Diagnostics for Early Diagnosis and Precautions, Enhanced environmental cleaning, cubicle curtain changes, room decontamination units for high rates. MRSA (rate per 1,000 patient days) 62% 0.4. CHG Washcloths, Pre-admission and Pre-op Screening, Rapid PCR Diagnostics for Early Diagnosis and Precautions.")
67
Conclusions The overall incidence of SSI in South East Asia varies between 1-20%. SSI account for approximately 20% of all HAI. Variability in SSI incidence related to surgical procedure and risk factors (eg, diabetes, wound classification). SSI have a substantial economic impact through increased hospital stay, additional treatment and consequently loss of productivity Clinical studies in patients undergoing abdominal, spinal and cardiac surgery show that VICRYL Plus sutures significantly reduce the incidence of SSI MEDICAL
. SSI have a substantial economic impact through increased hospital stay, additional treatment and consequently loss of productivity. Clinical studies in patients undergoing abdominal, spinal and cardiac surgery show that VICRYL Plus sutures significantly reduce the incidence of SSI. MEDICAL.")
Similar presentations







: What the Direct Caregiver Should Know>")



 Betty C. Jung, RN, MPH, CHES.>")













 Blood Stream Infections Ventilator Associated Pneumonia (VAP) Surgical Site Infections.>")