Download presentation
Presentation is loading. Please wait.

1
Long term follow-up after pulmonary radiofrequency ablation T. de Baère, Institut Gustave Roussy - Villejuif - France

3
Lung tumors Cancer - 80% of cancer cured = suregry ± other therapies (radiation/chemo) - Others surgical like techniques ? ablative therapies? Primary lung cancer - Second cause of death in man in France - Leading cause of cancer death in the world - 20% of patients are surgical candidates Lung metastases - 25/30% of cancer patients at autopsy - 50% of renal cell carcinoma - Sarcoma (42%), Colon (14%), Breast (9%), Renal (8%), Testicular (7%), Melanoma (6%), ENT (5%)
, Colon (14%), Breast (9%), Renal (8%), Testicular (7%), Melanoma (6%), ENT (5%).")
4
Lung Surgery Surgical resection of metastases - 1882 : Incidental resection of chest wall sarcoma and 2 metastases - 1947 : First series of 24 resections, including a repeated thoracotomy - 2000 : First report of RF ablation in the lung Criteria for resection metastases (The goal is to cure and to not harm) –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease –No better therapy
 –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease –No better therapy")
5
Lung Radiofrequency Surgical resection of metastases - 1882 : Incidental resection of chest wall sarcoma and 2 metastases - 1947 : First series of 24 resections, including a repeated thoracotomy - 2000 : First report of RF ablation in the lung Criteria for RF Ablation metastases (The goal is to cure and to not harm) –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease –No better therapy
 –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease –No better therapy")
6
Lung Radiofrequency Surgical resection of metastases - 1882 : Incidental resection of chest wall sarcoma and 2 metastases - 1947 : First series of 24 resections, including a repeated thoracotomy - 2000 : First report of RF ablation in the lung Criteria for RF Ablation metastases (The goal is to cure and to not harm) –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease –No better therapy RF can be possible
 –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease –No better therapy RF can be possible")
7
Lung Radiofrequency Surgical resection of metastases - 1882 : Incidental resection of chest wall sarcoma and 2 metastases - 1947 : First series of 24 resections, including a repeated thoracotomy - 2000 : First report of RF ablation in the lung Criteria for RF Ablation metastases (The goal is to cure and to not harm) –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease >> Two sites in a single RF session –No better therapy RF can be possible
 –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease >> Two sites in a single RF session –No better therapy RF can be possible")
8
Lung Radiofrequency Surgical resection of metastases - 1882 : Incidental resection of chest wall sarcoma and 2 metastases - 1947 : First series of 24 resections, including a repeated thoracotomy - 2000 : First report of RF ablation in the lung Criteria for RF Ablation metastases (The goal is to cure and to not harm) –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease >> Two sites in a single RF session –No better therapy –Limited to small size tumors RF can be possible
 –Patient must be able to tolerate –Sufficient pulmonary reserve –Primary tumor controlled / controlable –No extra-pulmponary disease >> Two sites in a single RF session –No better therapy –Limited to small size tumors RF can be possible")
9
420 – 500 kHz sinusoidal current ionic agitatin friction tissues heating Principle of radiofreqiency Temperature > 60°C : immediate cellular death

10
420 – 500 kHz sinusoidal current ionic agitatin friction tissues heating Principle of radiofreqiency Temperature > 60°C : immediate cellular death

11
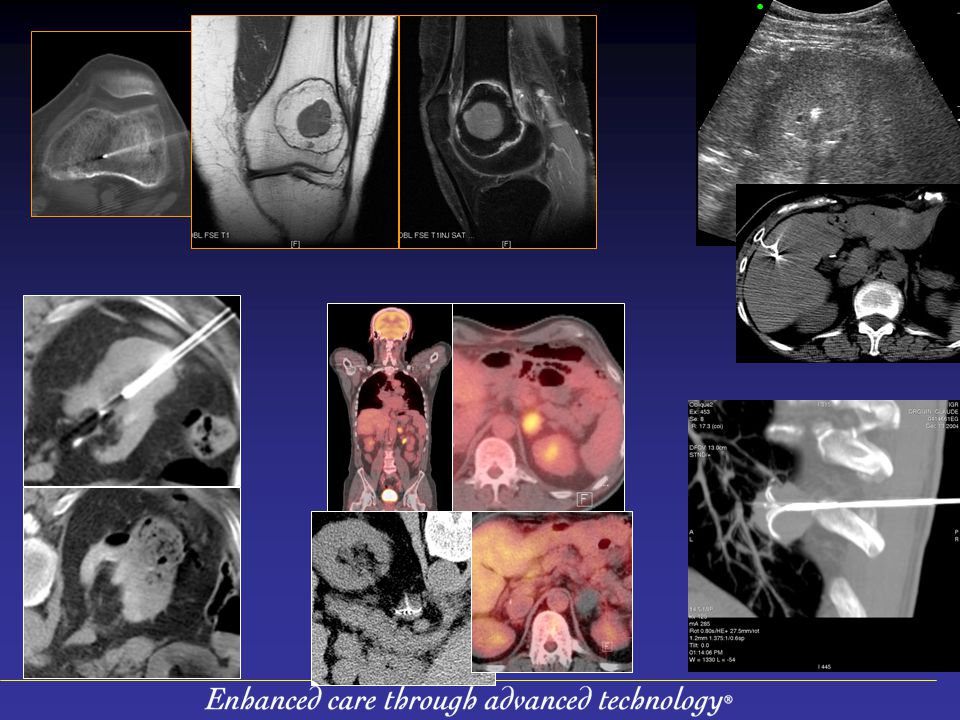
Methods (treatment) Accurate needle placement CT guidance –Needle placement Real time CT or Fluoro CT
 Accurate needle placement CT guidance –Needle placement Real time CT or Fluoro CT")
12
Methods (treatment) Accurate needle placement CT guidance –Needle placement Real time CT or Fluoro CT –Needle/electrode position Multiplanar reconstruction
 Accurate needle placement CT guidance –Needle placement Real time CT or Fluoro CT –Needle/electrode position Multiplanar reconstruction")
13
Material 244 patients (27-81 years) - Age : 62±14 years (27-85) 397 tumors 4 - 70 mm (m=17 ± 9.5) –Métastases : 197 patients (81%) - (343 tumors) –Primary : 47 patients (19%) - (52 tumors) –Unilateral 187 patients (77%), bilateral 57 patients (23%) –Number of tumor / Patient n = 1 (57%), n = 2 (25%), n = 3 (13%), n = 3 (5%), n = 5 or + (6%)
 - Age : 62±14 years (27-85) 397 tumors mm (m=17 ± 9.5) –Métastases : 197 patients (81%) - (343 tumors) –Primary : 47 patients (19%) - (52 tumors) –Unilateral 187 patients (77%), bilateral 57 patients (23%) –Number of tumor / Patient n = 1 (57%), n = 2 (25%), n = 3 (13%), n = 3 (5%), n = 5 or + (6%)")
14
Results 301 RF sessions / 314 lung treated –Usally one lung at a time / 13 bilateral Anesthesia General anesthesia296 Conscious sedation 3 Local 2

15
Pneumothorax with chest tube 12% Alveolar hemorraghe14% Cutaneous burn 1% Death 0.5% (ventricular fibrillation) Side effects and Complications (During treatment)
 Side effects and Complications (During treatment)")
16
No symptom66 % At least one symptom 34 % Pain 23% (mild 4%, moderate19%) Hemoptysis5% Pneumopathy3% Respiratory insufficiency0.5% Side effect (after hospital discharge)
 Hemoptysis5% Pneumopathy3% Respiratory insufficiency0.5% Side effect (after hospital discharge)")
17
Rate of local tumor progression Incomplete local ablation Incomplete local ablation Per tumor : 6.1% (4-9) @1 year, 11.2% (8-15) @ 2 years tumor ≤ 2cm : 3.7% (2-7) @1 year, 8.2% (5-13) @ 2 years tumor >2cm : 12.4% (7-21) @1 year, 19.4% (12-30) @ 2 years P = 0.002

18
Survival Survival : med =25 months 88.7% (84-92) @ 1 year, 70.3% (63-76) @ 2 years Patients without pulmonary evolution (RF site or distant) 57.5% (51-64) @ 1 year, 38.8% (32-47) @ 2 years
 57.5% 1 year, 38.8% 2 years")
19
Survival Survival : med =25 months 88.7% (84-92) @ 1 year, 70.3% (63-76) @ 2 years Patients without pulmonary evolution (RF site or distant) 57.5% (51-64) @ 1 year, 38.8% (32-47) @ 2 years
 57.5% 1 year, 38.8% 2 years")
20
(Simon CJ, Radiology 2007) 18 CRC mets patients 87%@1year, 78%@2 years Survival (Yan TD, Ann Surg Oncol 2007) 55 CRC mets patients 85%@1year, 64%@2 years, 46% @ 3 years 71 CRC mets patients 84%@1year, 62%@2 years, 46% @ 3 years (Yamakado K, JVIR 2007)
 18 CRC mets patients years Survival (Yan TD, Ann Surg Oncol 2007) 55 CRC mets patients years, 3 years 71 CRC mets patients years, 3 years (Yamakado K, JVIR 2007)")
21
Survival LONG-TERM RESULTS OF LUNG METASTASECTOMY: PROGNOSTIC ANALYSES BASED ON 5206 CASES Ugo Pastorino, J Thorac Cardivasc Surg 1997

22
RF ablation lung metastases Minimaly invasive High local success rate Curative treatment in non surgical patients Will replace some surgery ? Size is the main limitation 2.5-3.5 cm > 90 % = 70 % ≤ 50 % 4/5 cm

23
His own lung radiofrequency procedure from a painter patient debaere@igr.frdebaere@igr.fr : What is missing in the room ?

24
Size > 2 cm (p=0.0002) Rectal origin (p=0,02) Number Location (related to the pleura, medistinum Factors for survival
 Rectal origin (p=0,02) Number Location (related to the pleura, medistinum Factors for survival")
Similar presentations





 for Liver Tumour Dr Dai Wing Chiu Queen Mary Hospital.>")



 Plus Bevacizumab for Patients with Unresectable.>")




. Painful Bone metastases.>")




