Download presentation
Presentation is loading. Please wait.

1
THE ROLE OF VIDEO ASSISTED THORACIC SURGERY IN THE MANAGEMENT OF LUNG CANCER NEPAL C. CHOWDHURY, MD CARDIOTHORACIC & VASCULAR SURGERY ST. MARY’S MEDICAL CENTER

2
OVERVIEW OF LUNG CANCER BackgroundBackground–Epidemiology–Significance –Risk factors Goals of surgical therapy for lung cancerGoals of surgical therapy for lung cancer Comparison of thoracotomy vs. minimally invasive lung resectionsComparison of thoracotomy vs. minimally invasive lung resections

3
ESTIMATED CANCER DEATHS FOR SELECTED CANCER SITES IN US, 2007 STATE ALL SITES BRAIN/ NS BREAS T COLOR ECTAL LEUKE MIA LIVER LUNG/ BRONC HUS LYMPH OMA OVARY PANCR EAS PROST ATE OHIO24,6005401,8202,3509506007,3106106501,3701,350 KENTU CKY 9,3901506008603202203,450290220460310 WEST VIRGINI A 4,610902804801301101,450170140220160 US559,65012,74040,46052,18021,79016,780160,39018,66015,28933,37027,050

4
LUNG CANCER Leading cause of cancer death for both men and women More people die of lung cancer than of colon, breast and prostate cancers combined In 2008: about 215,020 new cases of lung cancer (NSCCA and SCCa) 1 About 161,840 will die of this disease in 2008 1 Overall cost of treating lung cancer exceeds $9.6 billion in the US each year 2 1.ACS: www.cancer.org 2. Medical Care v40 IV104-117, 2002

5
RISK FACTORS Tobacco Smoking (responsible for > 87% of cases) Age (>70% of people with lung ca are > 65yo) Asbestosis (50 –90x) Radon: naturally occurring radioactive gas that results from the breakdown of uranium in soil and rocks Radiation therapy to the chest Arsenic, certain mineral exposure (silicosis, berylliosis), uranium, gasoline Family history (inheritance of certain DNA changes on ch 6)
 Age (>70% of people with lung ca are > 65yo) Asbestosis (50 –90x) Radon: naturally occurring radioactive gas that results from the breakdown of uranium in soil and rocks Radiation therapy to the chest Arsenic, certain mineral exposure (silicosis, berylliosis), uranium, gasoline Family history (inheritance of certain DNA changes on ch 6)")
6
CANCERS AMONG MEN Prostate cancer (145.3) –First among men of all races and Hispanic origin. Lung cancer (85.3) –Second among white (84.4), black (104.5), Asian/Pacific Islander (49.7), and American Indian/Alaska Native (51.1) men. –Third among Hispanic men (48.5). Colorectal cancer (58.2) –Second among Hispanic men (50.3). –Third among white (57.0), black (67.6), Asian/Pacific Islander (42.0), and American Indian/Alaska Native (32.6) men. Note: The numbers in parentheses are the rates per 100,000 persons. Source: U.S. Cancer Statistics Working Group. Centers for Disease Control and Prevention, and National Cancer Institute; 2007.
 –Second among white (84.4), black (104.5), Asian/Pacific Islander (49.7), and American Indian/Alaska Native (51.1) men. –Third among Hispanic men (48.5). Colorectal cancer (58.2) –Second among Hispanic men (50.3). –Third among white (57.0), black (67.6), Asian/Pacific Islander (42.0), and American Indian/Alaska Native (32.6) men. Note: The numbers in parentheses are the rates per 100,000 persons. Source: U.S. Cancer Statistics Working Group. Centers for Disease Control and Prevention, and National Cancer Institute;")
7
LEADING CAUSES OF CANCER DEATHS AMONG MEN Leading causes of cancer death among men: Lung cancer (70.3) –First among men of all racial and Hispanic origin. Prostate cancer (25.4) –Second among white (23.4), black (56.1), American Indian/Alaska Native (16.5), and Hispanic (19.3) men. Colorectal cancer (21.6) –Third among men of all races and Hispanic origin. Liver cancer –Second among Asian/Pacific Islander men (15.1). Note: The numbers in parentheses are the rates per 100,000 persons. Source: U.S. Cancer Statistics Working Group. Centers for Disease Control and Prevention, and National Cancer Institute; 2007.
 –Second among white (23.4), black (56.1), American Indian/Alaska Native (16.5), and Hispanic (19.3) men. Colorectal cancer (21.6) –Third among men of all races and Hispanic origin. Liver cancer –Second among Asian/Pacific Islander men (15.1). Note: The numbers in parentheses are the rates per 100,000 persons. Source: U.S. Cancer Statistics Working Group. Centers for Disease Control and Prevention, and National Cancer Institute;")
8
CANCERS AMONG WOMEN Three most common cancers among women: Breast cancer (117.7) –First among women of all racial and Hispanic origin populations. Lung cancer (54.2) –Second among white (55.5) and American Indian/Alaska Native (35.3) women. –Third among black (50.4), Asian/Pacific Islander (26.9), and Hispanic (26.7) women. Colorectal cancer (42.7) –Second among black (50.6), Asian/Pacific Islander (32.1), and Hispanic (34.2) women. –Third among white (41.6) and American Indian/Alaska Native women (28.7). Note: The numbers in parentheses are the rates per 100,000 persons. Source: U.S. Cancer Statistics Working Group. Centers for Disease Control and Prevention, and National Cancer Institute; 2007.
 –Second among white (55.5) and American Indian/Alaska Native (35.3) women. –Third among black (50.4), Asian/Pacific Islander (26.9), and Hispanic (26.7) women. Colorectal cancer (42.7) –Second among black (50.6), Asian/Pacific Islander (32.1), and Hispanic (34.2) women. –Third among white (41.6) and American Indian/Alaska Native women (28.7). Note: The numbers in parentheses are the rates per 100,000 persons. Source: U.S. Cancer Statistics Working Group. Centers for Disease Control and Prevention, and National Cancer Institute;")
9
LEADING CAUSES OF CANCER DEATHS AMONG WOMEN Lung cancer (40.9) –First among white (41.9), black (40.0), Asian/Pacific Islander (18.1), and American Indian/Alaska Native (30.2) women. –Second among Hispanic women (14.4). Breast cancer (24.4) –First among Hispanic women (15.7). –Second among white (23.8), black (32.3), Asian/Pacific Islander (12.6), and American Indian/Alaska Native (15.0) women. Colorectal cancer (15.2) –Third among women of all races and Hispanic origin (15.2). Note: The numbers in parentheses are the rates per 100,000 persons. Source: U.S. Cancer Statistics Working Group. Centers for Disease Control and Prevention, and National Cancer Institute; 2007.
. Breast cancer (24.4) –First among Hispanic women (15.7). –Second among white (23.8), black (32.3), Asian/Pacific Islander (12.6), and American Indian/Alaska Native (15.0) women. Colorectal cancer (15.2) –Third among women of all races and Hispanic origin (15.2). Note: The numbers in parentheses are the rates per 100,000 persons. Source: U.S. Cancer Statistics Working Group. Centers for Disease Control and Prevention, and National Cancer Institute;")
10
COMPARATIVE NO OF DEATH PER YEAR

11
STAGING Tx: unable to visualize tumor Tis T0: no evidence of primary T1 < 3 cm, surrounded by parenchyma T2: > 3cm in size, or or assoc. atelectasis / pneumonitis / in the lobar bronchus, but 2 cm distal to the carina or invading visceral pleura T3 invades the chest wall or pericardium, parietal pleura without involving intrathoracic major structures, within 2 cm of the carina, atelectasis / pneumonitis of whole lung T4: invasion of intrathoracic structures, or satellite nodule in the same lobe, malignant pleural or pericardial effusion NXN0 N1: ipsilateral hilar LN N2: ipsilateral mediastinal or subcarinal N3: contralateral mediastinal / hilar, supraclavicular MxMo M1 including additional nodule in ipsilateral different lobe

12
STAGING NEW RECOMMENDATION BY IASLC Tx: unable to visualize tumor Tis T0: no evidence of primary T1 < 3 cm, surrounded by parenchymaT1a: <2 cm T1b: 2-3 cm T2: > 3cm in size, T2a: 3-5 cm T2b: 5-7 cm (Tumor > 7 cm : T3) or assoc. atelectasis / pneumonitis / in the lobar bronchus, but 2 cm distal to the carina or invading visceral pleura T3: > 7 cm (T2) or satellite nodule in the same lobe (T4) or invades the chest wall or pericardium, parietal pleura without involving intrathoracic major structures, within 2 cm of the carina, atelectasis / pneumonitis of whole lung T4: invasion of thoracic structures, or satellite nodule in the different ipsilateral lobe (M1a) NXN0 N1: ipsilateral hilar LN N2: ipsilateral mediastinal or subcarinal N3: contralateral mediastinal / hilar, supraclavicular MxMo M:M1a: Pleural and Pericardial dissemination M1b: Distant metastases Molecular staging in Stage I lung cancer: p53, Angiogenesis VIII, erbB-2, and rb (Ann Thorac Surg 2008; 85: S737-42) International association for study of lung cancer
 or satellite nodule in the same lobe (T4) or invades the chest wall or pericardium, parietal pleura without involving intrathoracic major structures, within 2 cm of the carina, atelectasis / pneumonitis of whole lung T4: invasion of thoracic structures, or satellite nodule in the different ipsilateral lobe (M1a) NXN0 N1: ipsilateral hilar LN N2: ipsilateral mediastinal or subcarinal N3: contralateral mediastinal / hilar, supraclavicular MxMo M:M1a: Pleural and Pericardial dissemination M1b: Distant metastases Molecular staging in Stage I lung cancer: p53, Angiogenesis VIII, erbB-2, and rb (Ann Thorac Surg 2008; 85: S737-42) International association for study of lung cancer.")
13
STAGE OF LUNG CANCER AT DIAGNOSIS NCI: SEER cancer statistics review 1973-2002

14
POSTSURGICAL SURVIVAL based on TNM subsets MOUNTAIN, 1997 NARUKE, 1988 STAGETNMN 5- Yr Survival N 1AT1N0M051167.024575.5 1BT2N0M054957.024157.0 IIAT1N1M07655.06652.5 IIBT2N1M028839.015340.0 T3N0M08738.010633.3 IIIAT3N1M05525.08539.0 Any N2M0 34423.036815.1 Mountain CF: Revisions in the International System for Staging Lung Cancer. Chest 111:1710-1717, 1997; Mountain CF, Dressler CM: Regional lymph node classification for lung cancer staging. Chest 111:1718-1723, 1997; and Naruke T, Tomoyuki G, Tsuchiya R, Suemasa K: Prognosis and survival in resected lung carcinoma based on the new international staging system. J Thorac Cardiovasc Surg 96:440-447, 1988.

15
SURGICAL THERAPY OF LUNG CANCER AIM: Complete removal of tumor, and all associated lymphatic drainage Minimize risk of tumor spillage En bloc resection of invaded structures is preferable to discontinuous resection Patient’s safety Should have less postoperative complications

16
PFT Jeng-Shing Wang. Pulmonary Function Tests in preoperative pulmonary evaluation. Resp Med 2004; 98: 598-605

17
TYPES OF SURGICAL LOBECTOMY Standard posterolateral thoracotomy Limited thoracotomy Muscle sparing thoracotomy VATS lobectomy

18
CONVENTIONAL THORACOTOMY 30-40 cm incision, cutting of muscles, and spreading of ribs

19
VATS LOBECTOMY Incisions: 3-4 without rib spreading Anatomic lobectomy using individual hilar dissection & node sampling or dissection Lobes are removed in a bag through one port enlarged up to 6 cm

20
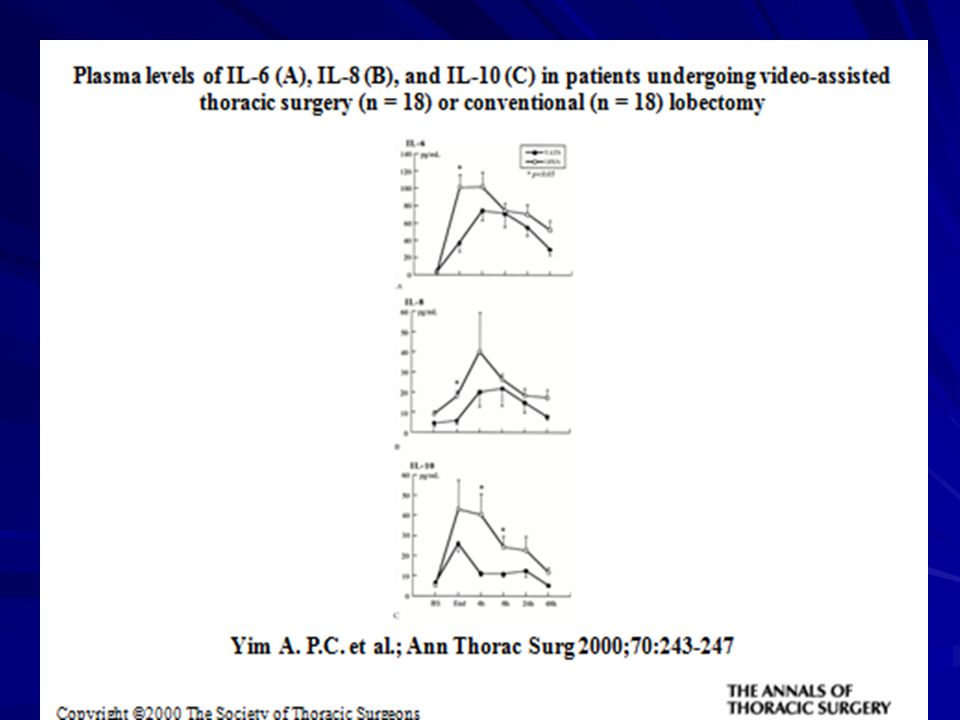
VATS LOBECTOMY SUGGESTED ADVANTAGES Less postoperative pain Preservation of pulmonary funtion Blunted inflammatory cytokine response Shorter chest tube duration Shorter length of stay Reduced overall cost Early return to full activity ? Adjuvant Rx better tolerated

21
INDICATIONS OF VATS LOBECTOMY Stage 1 lung cancer A few cases of benign disease (Bronchiectasis, Giant bullae) Elderly patients with a poor performance status
 Elderly patients with a poor performance status")
22
CONTRAINDICATIONS OF VATS LOBECTOMY Absolute Inability to achieve complete resection –T3 or T4 tumors –N2 or N3 disease Inability to obtain single lung ventilation Large Tumor > 5 cm (too large to remove through utility incision) Relative Conditions that compromise the safety of dissection -- Pre-op chemotherapy / radiation therapy or both -- Presence of hilar lympnadenopathy complicating dissection -- Presence of extensive adhesions Invasion of extra-pulmonary structure Tumors visible at bronchoscopy
 Relative Conditions that compromise the safety of dissection -- Pre-op chemotherapy / radiation therapy or both -- Presence of hilar lympnadenopathy complicating dissection -- Presence of extensive adhesions Invasion of extra-pulmonary structure Tumors visible at bronchoscopy")
23
CONCERNS Is it safe? So far no intra-operative death or major complication Visualization: Is it complete cancer operation? Any advantages over conventional thoracotomy?

24
CONCERNS contd. Post-operative pain: usually less (has been shown in many publications Post-operative pulmonary function Effect on inflammatory response: Quality of life

25
Copyright ©2008 The Society of Thoracic Surgeons Demmy T. L. et al.; Ann Thorac Surg 2008;85:S719-728S Pain control at 3 weeks after video assisted thoracic surgery (VATS) lobectomy
 lobectomy.")
33
Copyright ©2008 The Society of Thoracic Surgeons Demmy T. L. et al.; Ann Thorac Surg 2008;85:S719-728S Discharge independence after thoracoscopic lobectomy

34
Copyright ©2008 The Society of Thoracic Surgeons Demmy T. L. et al.; Ann Thorac Surg 2008;85:S719-728S Outpatient support, including home health care, rehabilitation, nursing home care, or death, required for 200 consecutive thoracic surgery patients by age group at Roswell Park Cancer Institute preceding the video-assisted thoracic surgery (VATS) lobectomy preference era
 lobectomy preference era.")
35
VATS LOBECTOMY VS OPEN LOBECTOMY Operative time: (227+47 min vs 196+64 min) Mean blood loss: (150+126 ml vs 300 +192 ml; P = 0.0089) Demmy et al Ann thorc surg 1999;68 Days in hospital: (5.3+3.7days vs 12.2+11.1 days; P = 0.02) Chest tube duration: (4.0+2.8 days vs 8.3+8.9 days; P = 0.06)
 Mean blood loss: ( ml vs ml; P = ) Demmy et al Ann thorc surg 1999;68 Days in hospital: ( days vs days; P = 0.02) Chest tube duration: ( days vs days; P = 0.06)")
36
OTHER CONCERNS Risk and management of intra-operative bleeding Tumor recurrence in the incision Adequacy of cancer operation

37
VATS LOBECTOMY: EXPERIENCE WITH 1,100 CASES McKenna RJ et al, ATS 2006; 81 Retrospective review of 1100 VATS lobectomies performed from 1992-2004 Diagnoses: –Primary lung cancer:1015 –Benign lung disease:53 –Pulmonary metastases or lymphoma:32 Conversion to thoracotomy:28 –Optimal resection:7 –Bleeding:6 –Tumor size:3 – Adhesions:4 –Other:7

38
PREOPERATIVE AND POSTOPERATIVE STAGING OF 1015 PATIENTS (VATS) STAGEPREOPERATIVEPOSTOPERATIVE IAIBIIAIIBIIIAIIIBIV 653 (59.4%) 313 (28.5%) 14 (1.3%) 12 (0.9%) 23 (2.2%) 00 561 (51%) 248 (22.5%) 50 (4.5%) 28 (2.5%) 109 (9.9%) 17 (1.5%) 2 (0.2%)
 STAGEPREOPERATIVEPOSTOPERATIVE IAIBIIAIIBIIIAIIIBIV 653 (59.4%) 313 (28.5%) 14 (1.3%) 12 (0.9%) 23 (2.2%) (51%) 248 (22.5%) 50 (4.5%) 28 (2.5%) 109 (9.9%) 17 (1.5%) 2 (0.2%)")
39
COMPLICATIONS AFTER VATS ANATOMIC RESECTION No intra-operative deaths Peri-operative deaths (n=9) --Respiratory failure (3), PE (3), MI (2) mesenteric infarction (1) Complications 15.3% – Air leak:56 – Afib:32 – Serous drainage: 14 – Readmission:13 – MI:10 – Empyema:4 – BPF:3 Blood transfusions required in 4.1%
 --Respiratory failure (3), PE (3), MI (2) mesenteric infarction (1) Complications 15.3% – Air leak:56 – Afib:32 – Serous drainage: 14 – Readmission:13 – MI:10 – Empyema:4 – BPF:3 Blood transfusions required in 4.1%")
40
5 YR SURVIVAL RATES AFTER OPEN VS VATS LOBECTOMY Mountain et al, Chest: 111: 1710, 1997 Rami-porta et al, Lung Ca: 29: 113, 2000 McKenna et al ATS: 81: 421, 2006 MOUNTAINRAMI-PORTAMCKENNA STAGE N % IAIBIIAIIBIIIAIIIBIV 511 67% 549 57% 76 55% 375 38% 399 26% 1030 4% 1427 1% 235 58% 817 50% 31 66% 290 42% 389 25% 138 28% 27 28% 497 76% 245 75% 245 56% 59 72% 108 33% 17 17%

41
VATS LOBECTOMY SUMMARY Safe, oncologically effective strategy Demonstrated feasibility Demonstrated advantages: 1. Less pain and analgesic requirement 2. Preserved pulmonary function 3. Less postoperative morbidity 4. Less chest tube drainage and shorter length of stay 5. Early return to full activity

Similar presentations













 M0 - No metastases M1 - Metastases present.>")











