Download presentation
Presentation is loading. Please wait.

1
Role of B cell in autoimmunity. Application to lupus and Sjögren’s syndrome Xavier Mariette, Rhumatologie, Hôpital Bicêtre, AP-HP, INSERM U802, Université Paris-Sud

2
Autoimmune diseases : T or B ? Until recently: T cell The cell which recognizes the peptide In number of animal models, transfer of the disease by T cells Auto-Ab: hallmark of the disease but no pathogenic role

3
Autoantibodies play a role Pathogenic in some AID : Autoimmune cytopenia, Graves disease, Myasthenia gravis Possibly pathogenic in some AID : Anti-DNA in lupus Anti-Pr3 in Wegener Anti- 2GP1 in antiphospholipid syndrome KRN / NOD mice : only spontaneous model of RA Transferable by anti-GPI Ab Autoimmune diseases : T or B ?

4
B-cells = efficient Ag presenting cells Mainly RF positive B cells MRL lpr/lpr mice Model of lupus, Sjögren, RA Infiltration by T cells JH -/- MRL lpr/lpr (no membrane Ig, no secretion of Ab) No T-cell infiltrate mIgM JH -/- (express membrane Ig but do not secrete Ig) T-cell infiltrate Chan et al, J immunol 1998 et J Exp Med 1999 Autoimmune disease : T or B ?
 No T-cell infiltrate mIgM JH -/- (express membrane Ig but do not secrete Ig) T-cell infiltrate Chan et al, J immunol 1998 et J Exp Med 1999 Autoimmune disease : T or B")
5
3 fonctions du lymphocyte B dans les MAI IL-6 Cartilage loss IL-6 T cell Macrophage Dendritic cell TNF- IL-10 RFRF Fix complement Inflamed synovia Inflammatory damage TNF- Plasma cell RFRF RFRF RFRF RFRF IL-10 TNF- IL-1 B cell Présentation de l’ antigène au LT et Activation du LT Production d’Ac Secrétion de cytokines proinflammatoires

6
CD40L T Lymphocyte CD4 CD3 TCR CMH BAFF-R CD40 B Lymphocyte CD 28 CD80 CD86 CTLA4

7
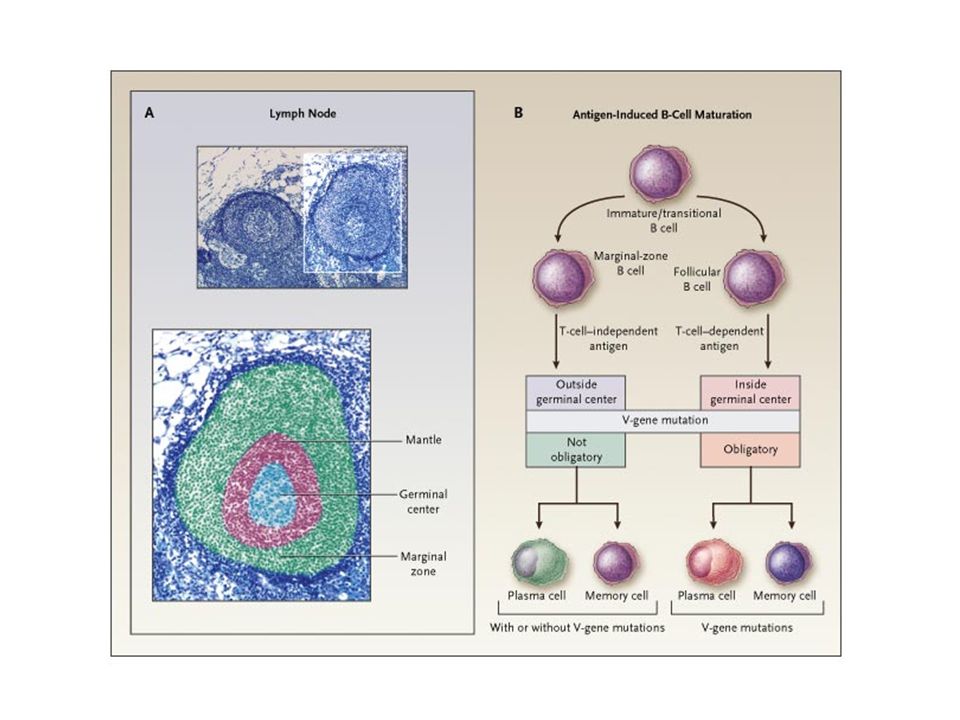
B-cell differentiation Memory B IgD+ IgM + Pro-B T T T T T T T T Centroblasts Memory B IgG+, IgA+ Plasma- cell Naive B T indépendent Marginal zone Transitional Immature B Pre-B T dépendent Bone marrow Secondary lymphoid organs (lymph nodes …) Germinal centre centrocytes Ab Blood Bone marrow Blood
 Germinal centre centrocytes Ab Blood Bone marrow Blood")
8
Expression of CD20 in the different Steps in the Maturation of B Cells c souche Pro B Pre B Naîf Activé Mémoire Plasmo CD20

9
Importance of subsets of B-cells CD27+ memory B cells : 1/3 of PBMC B cells Increased in lupus Dorner et al ART 2002 Decreased in Sjögren’s Hansen et al Arthritis Rheum 2002 Normal in RA (only 1 study: Bonhorst et al JI 2001 ) 2 kinds of CD27 memory B cells Classical post-GC IgM- (mainly IgG) CD27 memory B cells Marginal zone IgM+ CD27 memory B cells B cells are polarized like T cells Harris et al, Nat Immunol 2000 Be1: produce IFN Be2 : produce IL-4
 2 kinds of CD27 memory B cells Classical post-GC IgM- (mainly IgG) CD27 memory B cells Marginal zone IgM+ CD27 memory B cells B cells are polarized like T cells Harris et al, Nat Immunol 2000 Be1: produce IFN Be2 : produce IL-4")
10
Bm5 Bm4 Bm3 Bm2’ Bm2 Bm1 Bm1-Bm5 classification

12
Sjögren’s syndrome: an example of a disease with B- cell hyperactivity

13
Subsets of B-cells in blood CD27+ memory B cells in blood Bonhorst et al J Immunol 2001, Hansen et al Arthritis Rheum 2002 Bm2 (IgD+, CD38+) and Bm2’ B cells (pre- germinal center cells) Bonhorst et al J Immunol 2001 Correlated with increase of serum BAFF CD19 and retention of BCR in lipid rafts D’Arbonneau et al Arthritis Rheum 2006 Bm2 and Bm2’ and Bm5 and e Bm5 Ratio > 5 = diagnostic marker ? Binard et al, Ann Rheum Dis on line, 9 sept 2008

14
B-cells in salivary glands Represent 10 to 30% of the infiltrate CD27+ memory B cells Hansen et al Arthritis Rheum 2002 Germinal centre like in 20% of patients Salomonsson et al Arthritis Rheum 2003 Correlated with CXCL13 and CCL21 expression Barone et al Arthritis Rheum 2005 Contain transitional (TII) and marginal zone B cells Daridon et al Arthritis Rheum 2006
 and marginal zone B cells Daridon et al Arthritis Rheum 2006")
15
B-cells biomarkers and Sjögren’s Immunoglobulin level serum light chain level Moutsopoulos et al J Immunol 1983 Youinou et al Clin Exp Rheumatol 1988 Gottenberg et al Ann Rheum Dis 2006 (Free light chains) beta2 microglobulin level Michaski et al N Engl J Med 1975 Correlated with extra glandular signs Gottenberg et al Ann Rheum Dis 2005 Correlation between auto-antibodies and extraglandular complications
 beta2 microglobulin level Michaski et al N Engl J Med 1975 Correlated with extra glandular signs Gottenberg et al Ann Rheum Dis 2005 Correlation between auto-antibodies and extraglandular complications")
16
Extraglandular involvement p Value Present (n = 73) Absent (n = 104) Age (years)56.2 (14.6)57.2 (12.5)0.6 Disease duration (years)12.1 (7.0)12.4 (7.1)0.75 Anti-SSA only28.8%30.8%0.29 Anti-SSA and anti-SSB43.8%25%0.004 BLyS (ng/ml)6.1 (9.4)5.0 (5.0)0.39 ß 2 Microglobulin (mg/l)2.2 (0.9)1.7 (0.8)<10 –4 Gamma globulin (g/l)13.5 (7.3)13.2 (5.9)0.8 IgG (g/l)15. 8 (6.7)14.5 (6.8)0.28 IgA (g/l)3.0 (1.4)3.0 (1.5)0.26 IgM (g/l)1.6 (1.2)1.5 (1.0)0.44 RF (IU/ml)159.2 (293.1)135.8 (330.4)0.66 Decreased C3 level13.8%12.3%0.99 Decreased C4 level29.3%17.1%0.12 ESR (mm/h)30.6 (26.2)27.2 (25.9)0.42 C reactive protein (mg/l)10.5 (10.9)6.1 (2.8)0.003
14.5 (6.8)0.28 IgA (g/l)3.0 (1.4)3.0 (1.5)0.26 IgM (g/l)1.6 (1.2)1.5 (1.0)0.44 RF (IU/ml)159.2 (293.1)135.8 (330.4)0.66 Decreased C3 level13.8%12.3%0.99 Decreased C4 level29.3%17.1%0.12 ESR (mm/h)30.6 (26.2)27.2 (25.9)0.42 C reactive protein (mg/l)10.5 (10.9)6.1 (2.8)")
17
From polyclonal B-cell activation to B- cell lymphoma

18
Lymphoma and Sjögren’s The autoimmune disease where the risk is the most important Kassan et al Ann Intern Med 1978: RR = 44 Méta-analysis Zintzaras et al, Arch Intern Med 2005: RR = 19 Theander Ann Rheum Dis 2006: RR = 16 Frequency of mucosal localization Royer 1997: 12/16 Voulgarelis 1999: 27/33 Smedby 2005: 6/12 Theander 2006: 4/11 Histology: frequency of MALT marginal zone B-cell lymphomas

19
Lymphoma and Sjögren’s B-cell lymphoma No association with viruses or specific genetic abnormalities Predictive factors ( Tzioufas et al 1996, Skopouli et al 2000 ) Mixed cryoglobulinemia Low C4 Purpura Frequency of rheumatoid factor activity of membrane Ig of lymphomatous B cells Martin et al, Arthritis Rheum 2000
 Mixed cryoglobulinemia Low C4 Purpura Frequency of rheumatoid factor activity of membrane Ig of lymphomatous B cells Martin et al, Arthritis Rheum 2000")
20
Rheumatoid factor activity of lymphomas complicating Sjögren’s Localization of MALT nt(11, 14)nHomology CDR3- RF Salivary glands1142 (2%)3213 (41%) Stomach20950 (24%)458 (18%) Lung11347 (42%)190 OthersND 40 Bende et al J Exp Med 2005
nHomology CDR3- RF Salivary glands1142 (2%)3213 (41%) Stomach20950 (24%)458 (18%) Lung11347 (42%)190 OthersND 40 Bende et al J Exp Med 2005")
21
Analogies between hepatitis C lymphomas and Sjögren’s lymphomas HCV Virus ? Auto-Ag ? Hépatitis C Sjögren pc RF B BB BB BB BB Chromosomic abnormalities mc RF B Lymphoma BB BB Mariette, Ann Rheum Dis 2001

22
Unusual roles of B cells in AID

23
B-cells and bone destruction in RA Synovial and bone tissue in 8 RA patients Lymphoid infiltrates in bone marrow of subchondral bone with more B cells (CD20) than T cells (CD3) Presence of B-cell attracting chemokines (CCL21 et CXCL13) CD20 CD3 Bugatti et al, Arthritis Rheum 2005, 52: 3448-59
 than T cells (CD3) Presence of B-cell attracting chemokines (CCL21 et CXCL13) CD20 CD3 Bugatti et al, Arthritis Rheum 2005, 52:")
24
B-cells and bone destruction in RA Correlation between osteoclast count and bone marrow inflammatory score ACR 2005 – D’après Bugatti (1311) Bugatti et al, Arthritis Rheum 2005, 52: 3448-59
 Bugatti et al, Arthritis Rheum 2005, 52:")
25
B cells and periodontal bone erosion Model of infectious periodontitis (actinomycete) Ag-Specific B cells in periodontal bone Expressing RANK Ligand Increasing osteoclast formation and bone resorption Inhibited by OPG Han et al, JI 2005; 176: 625-31
 Ag-Specific B cells in periodontal bone Expressing RANK Ligand Increasing osteoclast formation and bone resorption Inhibited by OPG Han et al, JI 2005; 176:")
26
B cells and fibrosis Model of chemical-induced liver fibrosis infiltration of liver with T and B cells Depletion of T cells no change in fibrosis Depletion of B cells improvement of fibrosis How do B cells act for worsening fibrosis ? By an antibody independent mechanism: mIgM JH -/- express membrane Ig but do not secrete Ig and develop as fibrosis as wild type mice Antigen presentation role ? No Cell / cell contact ? Secretion of cytokines ? Novobrantseva et al, JCI 2005; 115:3072-82

27
A new axis in pathogeny of lupus and Sjögren Interferon type 1 or type 2 BAFF (B-cell Activator Factor of the TNF family) or BLyS Activation of B cells
 or BLyS Activation of B cells")
28
Interferon signature in Sjogren’s like in lupus TLR8, TLR9, IFITM1, MICB, TAP2, B2M, CCL20 CCL-18 SOCS-3 Hjermelvik at al Arthritis Rheum. 2005 May;52(5):1534-44. Gottenberg et al, PNAS 2006 Feb 21;103(8):2770-5 424 differentially expressed genes
: Gottenberg et al, PNAS 2006 Feb 21;103(8): differentially expressed genes.")
29
Presence of type 1 IFN-secreting cells in salivary glands of patients Bave at al Arthritis Rheum. 2005 Apr;52(4):1185-95. Interferon signature in Sjogren’s like in lupus
: Interferon signature in Sjogren’s like in lupus.")
30
Presence of pDC in salivary glands CD123 BDCA2 SjogrenControls

31
A new axis in pathogeny Interferon type 1 or type 2 BAFF (B-cell Activator Factor of the TNF family) or BLyS Activation of B cells
 or BLyS Activation of B cells")
32
The BAFF system IFN IFN IL-10 Mono M B lymphocyte BR3BCMATACI CD40 APRIL BAFF BCR sBAFF Survival Autoantibody secretion

33
BAFF Transgenic mice Biological features Increase in peripheral B cells Increase in serum Ig Increase in serum auto-antibodies (RF, Anti- DNA) Clinical features Autoimmune glomerulonephritis Polyarthritis Auto-immune Sialadenitis B-cell lymphoma x2 (x30 in TNF ko mice) Mackay, J Exp Med 1999; Khare, PNAS 2000; Groom, JCI 2002; Batten JI 2004
 Clinical features Autoimmune glomerulonephritis Polyarthritis Auto-immune Sialadenitis B-cell lymphoma x2 (x30 in TNF ko mice) Mackay, J Exp Med 1999; Khare, PNAS 2000; Groom, JCI 2002; Batten JI 2004")
34
Serum BAFF is increased and correlates with the presence of autoantibodies Mariette et al. Ann Rheum Dis, 2003

35
Serum BAFF is increased and correlates with the level of autoantibodies

36
Increase in BAFF in Sjögren: other reports Increase in serum level of BAFF Groom JCI 2002 Correlated with hypergammaglobulinemia Szodoray et al, J Clin Immunol. 2004; 24:600-11 Correlated with anti-SSA secretion Pers JO at al Ann N Y Acad Sci 2005;1050:34-9 Increase in saliva level of BAFF Correlated with complications of periodonditis Pers JO at al, Arthritis Rheum 2005;52:2411-4 Increase in serum level of APRIL Correlated with BAFF level Jonsson et al, J Clin Immunol. 2005

37
IFN IFN TNF Monocyte Epithelial T BAFF Survival Auto-Ab Auto-immunity B NF B Fibroblastic Paracrine or autocrine BAFF secretion Autoimmune B cell Autoimmunity

38
Quantification of BAFF by Q-PCR in salivary glands RNA extracted from labial salivary glands 0 2 4 6 8 10 12 pSS Patients Controls BAFF mRNA/actine 3.8 fold, P = 0.003 Gottenberg et al, PNAS 2006

39
Lavie et al, J Pathol 2004 Detection of BAFF in salivary glands Sjögren Normal Sarcoidosis

40
Sjögren BAFF Sjögren CD3Sjögren BAFF + CD3 Detection of BAFF in salivary glands Lavie et al, J Pathol 2004

41
BAFF can be expressed by salivary ducts [ BAFF ] = 0[ BAFF ] = [ AC ][ BAFF ] = 2 [ AC ] BAFF
![BAFF can be expressed by salivary ducts [ BAFF ] = 0[ BAFF ] = [ AC ][ BAFF ] = 2 [ AC ] BAFF](http://images.slideplayer.com/14/4224650/slides/slide_41.jpg "BAFF can be expressed by salivary ducts [ BAFF ] = 0[ BAFF ] = [ AC ][ BAFF ] = 2 [ AC ] BAFF")
42
Presence of BAFF in salivary B cells Daridon et al Arthritis Rheum. 2007

43
BAFF in salivary glands : T cells, epithelial cells and B cells BAFF Daridon et al Arthritis Rheum. 2007

44
Effect of IFN on BAFF mRNA in salivary epithelial cells Ittah et al Arthritis Research Therapy, 2006

45
BAFF mRNA BAFF Protein TLR2TLR3 -actin TLR7TLR9 BAFF expression by SGECs after TLR stimulation Ittah et al Eur J immunol, 2008Apr;38(4):1058-64
:")
46
BAFF is highly induced by viral infection or poly (I:C) stimulation of epithelial cells Salivary epithelial cells* Airway epithelial cells** Oral epithelial cells*** Epidermal and intestinal epithelial cells*** This induction of BAFF may be TLR dependant or independent Type 1 IFN dependent or independent * Ittah et al Eur J immunol 2008 ** Kato et al, JI 2006 *** Xu et al, Nature Immunol 2007 BAFF is induced by viral infection
 stimulation of epithelial cells Salivary epithelial cells* Airway epithelial cells** Oral epithelial cells*** Epidermal and intestinal epithelial cells*** This induction of BAFF may be TLR dependant or independent Type 1 IFN dependent or independent * Ittah et al Eur J immunol 2008 ** Kato et al, JI 2006 *** Xu et al, Nature Immunol 2007 BAFF is induced by viral infection")
47
Cross-regulation between type 1 IFN and TNF Banchereau, Pascual Immunity 2006

48
TRIPSS: Design of the study Visits Pre-inclusion W0 W2 W6 W10 W14 W18 W22 D-14 Infliximab 5mg/kg or placebo Evaluation Mariette et al, Arthritis Rheum 2004

49
Primary end point: Decrease of at least 30% in 2 of the 3 VAS 0 5 10 15 20 25 30 30% Response at W10 INF Placebo P=0.89 Mariette et al, Arthritis Rheum 2004

50
Anti-TNF may increase IFN and BAFF Controlled trial in Sjogren’s with etanercept (n=17) EtanerceptPlacebo IFN activity baseline (units) 3.81 ± 1.864.61 ± 3.47 IFN activity 3 months (units) 7.87 ± 5.95 p=0.04 3.92 ± 3.81 p=0.67 BAFF baseline (ng/ml) 0.86 ± 0.280.80 ± 0.23 BAFF 3 months (ng/ml) 1.12 ± 0.25 p=0.03 0.95 v 0.32 p=0.24 Mavragani et al, Arthritis Rheum 2007
 EtanerceptPlacebo IFN activity baseline (units) 3.81 ± ± 3.47 IFN activity 3 months (units) 7.87 ± 5.95 p= ± 3.81 p=0.67 BAFF baseline (ng/ml) 0.86 ± ± 0.23 BAFF 3 months (ng/ml) 1.12 ± 0.25 p= v 0.32 p=0.24 Mavragani et al, Arthritis Rheum 2007")
51
Change in gammaglobulin level between W10 and baseline in TRIPSS Placebo n=38Infliximab n=39 Gammaglobulin (g/l) 0.12 1.161.03 1.94 0.02 IgG (g/l) 0.06 1.190.87 2.47 0.10 IgA (g/l) 0.03 0.560.13 0.42 0.40 IgM (g/l) -0.01 0.400.48 0.87 0.005 Mariette et al, Arthritis Rheum 2004
 0.12 IgG (g/l) 0.06 IgA (g/l) 0.03 IgM (g/l) Mariette et al, Arthritis Rheum 2004")
52
Induction of anti-nuclear antibodies by infliximab ATTRACT: RA (102 weeks): ANAPlacebo: 27%Infliximab: 62% anti-dsDNAPlacebo: 0%Infliximab: 15% ACCENT I: Crohn (54 weeks): ANAAll patients: 49% anti-dsDNAAll patients: 26%
: ANAPlacebo: 27%Infliximab: 62% anti-dsDNAPlacebo: 0%Infliximab: 15% ACCENT I: Crohn (54 weeks): ANAAll patients: 49% anti-dsDNAAll patients: 26%")
53
Lupus induced by anti-TNF The CRI study Retrospective study in France 22 cases : 10 cutaneous reactions with ANA and anti-DNA Ab 6 infliximab, 4 etanercept 12 true SLE with 4 ACR criteria 9 infliximab, 3 etanercept Recovery in all patients after withdrawal of anti-TNF but need of steroids in 6 cases M De Bandt, Arthritis Research Therapy 2005

54
B-cell targeted therapy in lupus and Sjögren’s

55
Rituximab in lupus 18 open studies including 2 to 32 patients Efficacy on most symptoms including nephritis Decrease of anti-DNA Ab No decrease of anti-ENA Ab Decrease of memory B cells and plasmablast Re-establishment of tolerance ? Randomized control studies are going on

56
Rituximab in lupus Press release - 29 avril 2008 -- « Genentech, Inc. (NYSE: DNA) and Biogen Idec, Inc. (Nasdaq: BIIB) announced today that a Phase II/III study of Rituxan® (rituximab) for systemic lupus erythematosus (SLE, commonly called lupus) did not meet its primary endpoint defined as the proportion of Rituxan treated patients who achieved a major clinical response (MCR) or partial clinical response (PCR) measured by BILAG, a lupus activity response index, compared to placebo at 52 weeks. The study also did not meet any of the six secondary endpoints. » This study excluded patients with lupus nephritis (LN). A total of 257 patients from approximately 55 sites in the U.S. and Canada were randomized 2:1 to receive Rituxan plus prednisone or placebo plus prednisone in two infusions 15 days apart.
 and Biogen Idec, Inc. (Nasdaq: BIIB) announced today that a Phase II/III study of Rituxan® (rituximab) for systemic lupus erythematosus (SLE, commonly called lupus) did not meet its primary endpoint defined as the proportion of Rituxan treated patients who achieved a major clinical response (MCR) or partial clinical response (PCR) measured by BILAG, a lupus activity response index, compared to placebo at 52 weeks. The study also did not meet any of the six secondary endpoints. » This study excluded patients with lupus nephritis (LN). A total of 257 patients from approximately 55 sites in the U.S. and Canada were randomized 2:1 to receive Rituxan plus prednisone or placebo plus prednisone in two infusions 15 days apart..")
57
Other positive open studies with rituximab Lupus Sjögren’s Syndrome ANCA-associated vasculitis Cryoglobulinemia Inflammatory myopathies Aquired anti-F VIII antibodies Pemphigus Multiple sclerosis ++ (positive RC) Myasthenia gravis Anti-MAG-associated demyelinating neuropathy
 Myasthenia gravis Anti-MAG-associated demyelinating neuropathy")
58
AIR registry: non RA autoimmune diseases 179 patients 46 SLE 42 primary Sjögren’s syndrome 21 vasculitis 17 myositis 53 other diseases 116 patients already had at least 1 follow-up visit Mean follow-up : 35.2 weeks 79 patient years

59
Lupus and Sjögren SLE (data on 36 patients) Glomerulonephritis : 10 patients Mean corticosteroid dosage : 22.4 mg/day No concomitant IS : 8 patients Concomitant IS : 28 patients HQ : 13, MTX : 5, MMF : 7, AZA : 2, CPH : 1 Efficacy : 21/36 (58%) Retreatments : 11 patients pSS (data on 36 patients) 33/36 (92%): systemic involvement Mean corticosteroid dosage : 13.5 mg/day No concomitant IS : 30.5 % Efficacy on systemic complications : 23/36 (64%) Retreatments : 7
 Glomerulonephritis : 10 patients Mean corticosteroid dosage : 22.4 mg/day No concomitant IS : 8 patients Concomitant IS : 28 patients HQ : 13, MTX : 5, MMF : 7, AZA : 2, CPH : 1 Efficacy : 21/36 (58%) Retreatments : 11 patients pSS (data on 36 patients) 33/36 (92%): systemic involvement Mean corticosteroid dosage : 13.5 mg/day No concomitant IS : 30.5 % Efficacy on systemic complications : 23/36 (64%) Retreatments : 7")
60
Overall tolerance in non RA AIDs 2 deaths pSS patient with metastatic Paget’s disease SLE patient with Endocarditis due to Staph Aureus after the second course (γglob 4.3 g/l before the 2nd course) 5 severe infections : 6.3/100 patient years Staphylococcus Aureus endocarditis Staphylococcus pneumonia Corynebacteria pneumonia undocumented pneumonia Staphylococcus Aureus arthritis 4 moderate serum-sickness like reactions SLE : 2 Vasculitis : 1 pSS: 1
 5 severe infections : 6.3/100 patient years Staphylococcus Aureus endocarditis Staphylococcus pneumonia Corynebacteria pneumonia undocumented pneumonia Staphylococcus Aureus arthritis 4 moderate serum-sickness like reactions SLE : 2 Vasculitis : 1 pSS: 1")
61
Rituximab in Sjögren’s: 3 open studies StudyDutch 1 French 3 Patients 15 patients 6 lymphoma 9 early disease (<4yrs) 16 patients 5 lymphomas 11 systemic features Efficacy Lymphoma: 3/7 Dryness: only in patients with residual glandular function Lymphoma: 4/5 Systemic signs: 9/11 Subj dryness: 5/16 Obj dryness: 2/16 French 2 ( Brittany ) 16 patients Disabling subjective symptoms Dryness: subjective improvement in patients with early pSS 1. Pijpe et al. Arthritis Rheum, 2005 2. Devauchelle-Pensec et al.. Arthritis Rheum, 2007 3. Seror et al. Ann Rheum Dis, 2006

62
Sjögren’s syndrome: the dutch Study Open study of 15 patients 9 with early pSS 6 with pSS and MALT lymphoma Tolerance: 3 of 9 patients without lymphoma developed serum sickness 1 week after the 2nd infusion Pijpe at al, Arthritis Rheum 2005

63
Effect of rituximab on mouth dryness Pijpe at al, Arthritis Rheum 2005

64
The French study: biological findings A significant median level decrease of RF : 124 to 7.5 IU/mL (p=0.004, n=13 ) Gammaglobulin : 13.4 to 9.6 g/L (p=0.003, n=15) IgG : 10.8 to 7.7 g/L (p=0.003, n=11) Beta-2 microglobulin : 3.3 to 2.3 mg/L (p =0.02, n=12) Seror et al. Ann Rheum Dis, 2006

65
A small randomized controlled study 8 patients with rituximab and 9 with placebo Mean decrease of fatigue VAS: 50% with rituximab 20% with placebo P=0.24 between the 2 groups but significant decrease only in the rituximab group 1 episode of serum sickness disease in the rituximab group Dass et al, Ann Rheum Dis 2008 online 14 Feb Rituximab in Sjögren’s: the first RCT

66
TEARS Etude multicentrique de phase II randomisée menée en double aveugle, contrôlée versus placebo Coordonnateur : Pr Alain Saraux (Brest) Centres participants : Pr A. Saraux / V Devauchelle (Brest)*, Pr Olivier Vittecoq (Rouen) Pr E Hachulla (Lille) Pr X Mariette (KB)* Pr J Sibilia (Strasbourg)* Tolérance et efficacité du rituximab dans le syndrome de Sjögren ESR ML20771 Promoteur : Hôpital de Brest (PHRC) Dr J Morel (Montpellier) Pr A Perdriger (Rennes) Dr X Puechal (Le Mans) Dr J-M Berthelot (Nantes) Dr D Alcaix (Le Havre) Pr L Guillevin (Cochin) Dr JJ Dubost (Clermont Ferrand)
*, Pr Olivier Vittecoq (Rouen) Pr E Hachulla (Lille) Pr X Mariette (KB)* Pr J Sibilia (Strasbourg)* Tolérance et efficacité du rituximab dans le syndrome de Sjögren ESR ML20771 Promoteur : Hôpital de Brest (PHRC) Dr J Morel (Montpellier) Pr A Perdriger (Rennes) Dr X Puechal (Le Mans) Dr J-M Berthelot (Nantes) Dr D Alcaix (Le Havre) Pr L Guillevin (Cochin) Dr JJ Dubost (Clermont Ferrand).")
67
Schéma de l’étude S2 S16S48 Placebo* n=60 Rituximab n=60 Patients SGS n = 120 Randomisation S24J15J1 SélectionInclusionPériode de suivi Rituximab 1000mg ou Placebo (* Serum phy ) Visites de suivi Début des inclusions : Q4 2007 Durée des inclusions : 36 semaines J-30J-7 S6S36 Evaluation principale
 Visites de suivi Début des inclusions : Q Durée des inclusions : 36 semaines J-30J-7 S6S36 Evaluation principale")
68
Serum BAFFPBMC BAFF mRNA D Increase in BAFF after rituximab Lavie et al, Ann Rheum Dis 2006 2 SLE 2 SS 1 RA

69
The level of BAFF before RTX could predict the lenght of B-cell depletion Pers et al, A§R 2007

70
Increase of BAFF after rituximab Interest of association of anti-BAFF and rituximab ? to avoid stimulation of auto-reactive B cells via BAFF To prolong B-cell depletion

71
Epralizumab (anti-CD22 Ab) : open study Patient demographics and baseline disease characteristics n =15 Gender (female/male)13/2 Age (years)49 (33–73) Median years post-diagnosis2.9 (1–16) Unstimulated salivary flow (ml/minute) 0.07 ± 0.13 Fatigue VAS (mm)56 ± 22 Focus score ≥ 112 (80%) Anti-Ro antibodies12 (80%) Anti-La antibodies11 (73%) ESR (mm/hour)33 ± 15 IgG (mg/dl)2,114 ± 934 Steinfeld et al ART 2006
 : open study Patient demographics and baseline disease characteristics n =15 Gender (female/male)13/2 Age (years)49 (33–73) Median years post-diagnosis2.9 (1–16) Unstimulated salivary flow (ml/minute) 0.07 ± 0.13 Fatigue VAS (mm)56 ± 22 Focus score ≥ 112 (80%) Anti-Ro antibodies12 (80%) Anti-La antibodies11 (73%) ESR (mm/hour)33 ± 15 IgG (mg/dl)2,114 ± 934 Steinfeld et al ART 2006")
72
Epralizumab (anti-CD22 Ab) : open study Steinfeld et al ART 2006
 : open study Steinfeld et al ART 2006")
73
Epralizumab (anti-CD22 Ab) : open study Steinfeld et al ART 2006
 : open study Steinfeld et al ART 2006")
74
Conclusion B cells play a role in autoimmunity 3 RCT demonstrated efficacy of rituximab in RA But no large RCT demonstrated efficacy of rituximab in other systemic diseases Problems with end-points The currents targets to be explored in controlled studies in lupus and Sjögren’s The IFN pathway BAFF (or BLyS) B cells The new treatments will come from new pathogenic concepts
 B cells The new treatments will come from new pathogenic concepts")
Similar presentations








 & Multiple Sclerosis>")




>")





