Download presentation
Presentation is loading. Please wait.

1
page1

2
IN THE NAME OF GOD

3
Sonography of Scrotum and Testes
.

4
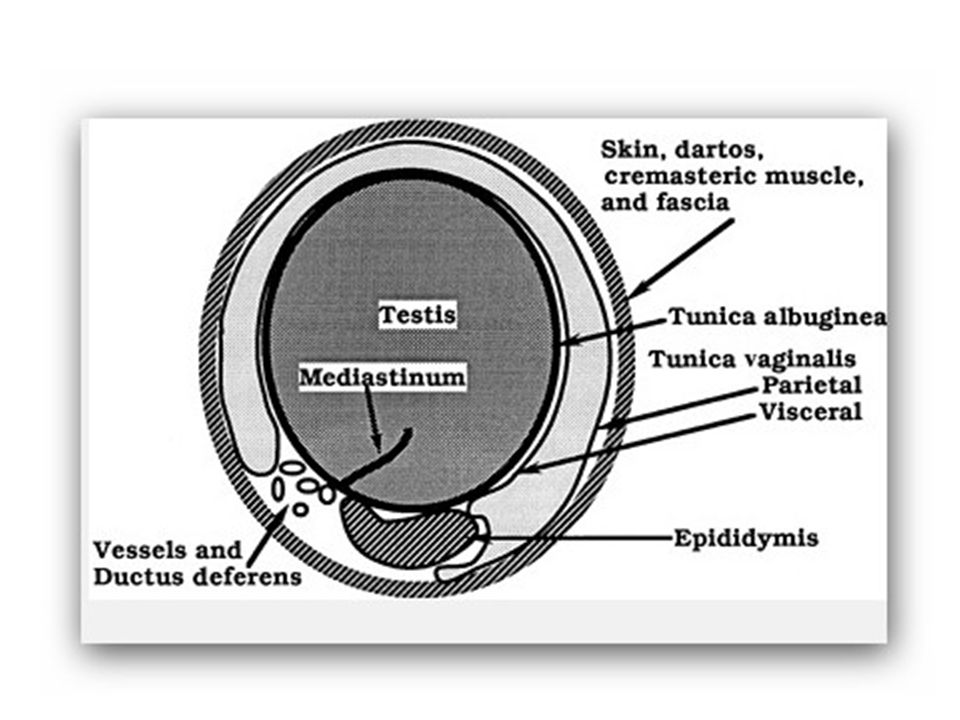
Anatomy The scrotum is divided by the midline raphe. Each half of the scrotum contains a spermatic cord, testis, and epididymis. The testes descend into the scrotum at approximately the 28th gestational week via the inguinal canal through the peritoneal recess, which is called the processus vaginalis. The processus vaginalis gradually closes through infancy and childhood. The testis is covered by a visceral layer of tunica vaginalis, except where in contact with epididymis, and by the tunica albuginea. The posterior surface of the tunica albuginea extends into the testis to form the mediastinum testis. This is seen as a middle echogenic line on longitudinal US of the testis The testis has lobules containing the seminiferous tubules. Testicular lobules are occasionally identified as lines radiating from the mediastinum testis

8
The size and shape of the testes change with age
The size and shape of the testes change with age. Testicular size is influenced by gonadal hormones. In boys, from birth to 5 months of age, the testicular volume rises to a maximum of 0.44 (±0.03) cm3. The rise in testicular volume coincides with a peak in gonadotropic hormones, so-called minipuberty, at approximately 3 to 4 months of age. After age 5 months, the testicular volume steadily declines and reaches its minimum volume at approximately 9 months of age and remains approximately the same size until puberty. The testis is rounded in newborns and gradually becomes ovoid with growth.
 cm3. The rise in testicular volume coincides with a peak in gonadotropic hormones, so-called minipuberty, at approximately 3 to 4 months of age. After age 5 months, the testicular volume steadily declines and reaches its minimum volume at approximately 9 months of age and remains approximately the same size until puberty. The testis is rounded in newborns and gradually becomes ovoid with growth.")
9
The epididymis has three parts: head, body, and tail
The epididymis has three parts: head, body, and tail. In the normal epididymis, only the head is routinely identified. The epididymal head is located in the upper pole of the scrotum, is triangular in shape, and has the same echogenicity as the testis. Testicular appendixes are remnants of the mesonephric and paramesonephric ducts. They can be identified by US in cases of hydrocele The spermatic cord appears as an echogenic band on longitudinal images and ovoid on transverse images as it passes in the inguinal canal. Color Doppler shows the testicular artery and pampiniform venous plexus .In the inguinal canal, the normal thickness of the spermatic cord is up to 4 mm. The normal inguinal canal does not contain fluid.

10
Ultrasound (US) is a readily available and relatively inexpensive imaging modality that can be performed on patients at any age without the need for sedation or any other pretest preparation. US examinations are safe and there is no significant biologic risk from radiation exposure. Different pathologies of the scrotum may have similar clinical presentation, such as acute scrotal pain or scrotal mass. US of the scrotum can better guide treatment by improving the definition of the scrotal pathology. For these reasons, US became the imaging modality of choice for evaluation of scrotal pathology, and, in most cases, US is the first and only imaging needed for evaluation of scrotal pathology.

11
Color Doppler demonstrates capsular and intratesticular vessels.
In prepubertal testes, it can be difficult to detect intratesticular flow, but the capsular arteries are easier to identify. It is, however. The resistive index of the intratesticular arteries changes with age from high to low resistive index

13
Indications for Scrotal Ultrasound
Pain: trauma, inflammation, torsion Mass: testicular, extratesticular Evaluation of a possible hernia and its contents Search for occult neoplasm in cases of retroperitoneal or mediastinal lymphadenopathy Follow-up of previous infections, tumors, lymphoma, leukemia Small testes, atrophy Location of undescended testes Infertility Precocious puberty or feminization

14
The acute scrotum Acute scrotal pain is a medical urgency as 12% to 26% of boys who have it have testicular torsion. The main differential diagnosis includes testicular torsion, torsion of appendix testis, and epididymitis. It is crucial to rapidly diagnose testicular torsion because prognosis of the testis depends on the duration of torsion.[Ischemia of the testis can be reversible in the first 6 hours.[US is typically required when the clinical assessment is equivocal for testicular torsion. Testicular torsion typically presents as an acute, excruciating scrotal pain of short duration before a patient arrives in the emergency room. Physical examination typically reveals diffuse tenderness, abnormal high and horizontal position of the testis, and absence of the cremasteric reflex.

15
Gray-scale findings of testicular torsion may be normal
Gray-scale findings of testicular torsion may be normal. Testicular gray-scale abnormalities include testicular swelling or heterogeneous or decreased testicular echotexture. Heterogeneous parenchymal echotexture usually indicates testicular nonviability. Other findings include swelling of the epididymis, hydrocele, and scrotal skin edema .Epididymal swelling is common in testicular torsion and, in a few cases, associated with increased epididymal flow. A gray-scale study should include evaluation of the spermatic cord. A coiled spermatic cord could be the only sign for testicular torsion as perfusion of the testis can be normal in partial torsion (<360°) or even increased in a case of torsion-detorsion. Evaluation of the spermatic cord increases the sensitivity for detection of testicular torsion.
 or even increased in a case of torsion-detorsion. Evaluation of the spermatic cord increases the sensitivity for detection of testicular torsion.")
16
Decreased testicular blood flow on a color Doppler study is the most sensitive finding that indicates testicular torsion. Testicular capsular blood flow may increase and erroneously suggest, in young boys, the presence of testicular perfusion. Therefore, prudent examination of intratesticular blood flow is necessary. Spectral evaluation of the blood flow and documentation of venous and arterial wave flow are important. Initially, only venous flow may be absent. Comparing the intratesticular flow to the contralateral testis is important, as any decrease in perfusion or change in the waveform may be the first indication of testicular torsion

17
Acute torsion of the testis

18
Rates of testicular salvage by time from start of symptoms.
Davenport, M. BMJ 1996;312: Copyright ©1996 BMJ Publishing Group Ltd.

19
Torsion of Testicular Appendix
The appendix testis, a müllerian duct remnant located at the superior pole of the testicle, is the most common appendix to twist. The epididymal appendix, located at the head of the epididymis, is a wolffian duct remnant. Torsion of testicular appendix can occur at any age but is most common between the ages of 7 and 12 years. The pain is typically indolent and not as severe as the pain from testicular torsion. Duration of scrotal pain is significantly longer than that of testicular torsion. A palpable tender nodule in the upper pole of the scrotum and the blue dot sign, which represents the bluish discoloration of the torsed appendix, are specific signs for torsion of testicular appendix. US typically demonstrates an extratesticular nodule with no vascularity in the upper pole of the scrotum. The maximal diameter of the torsed appendix varies from 4 to 16 mm. There may be an overlap between the size of torsed and normal appendixes when the nodule is smaller than 6 mm.

20
The torsed appendix leads to secondary inflammation in the surrounding structures. The epididymis is almost always swollen with increased perfusion, and occasionally there is swelling and increased perfusion of the testis. Other findings include scrotal wall edema and hydrocele. In some cases, when the torsed appendix is not identified by US, the findings cannot be distinguished from acute epididymitis. Treatment includes analgesic and anti-inflammatory medications. Surgery is reserved for patients in excruciating pain who are not responding to medication or when it is not possible to clinically distinguish from testicular torsion.

21
Scrotal appendages. (A) Appendix testis
Scrotal appendages. (A) Appendix testis. (B) Appendix epididymis originating from the surface of an epididymal cyst. Both appendages are seen because of thepresence of peritesticularfluid. Arrow, appendages. EC, epididymal cyst
 Appendix testis. (B) Appendix epididymis originating from the surface of an epididymal cyst. Both appendages are seen because of thepresence of peritesticularfluid. Arrow, appendages. EC, epididymal cyst.")
22
Torsed appendix testis
Torsed appendix testis.enlarged avascular appendix testis surrounded by increased blood flow

24
Acute Epididymitis Epididymitis is an inflammation of the epididymis. Epididymitis is described in response to infection, trauma, vasculitis, or urine refluxing into the ejaculatory ducts but in most cases is idiopathic.The diagnosis is often based on clinical presentation of a few days of acute scrotal pain, swelling, and tenderness of the epididymis. Presentation in young boys and those with recurrent epididymitis should lead to further evaluation with renal US and cystourethrography for associated anomalies. Anomalies that are described in association with epididymitis include ectopic ureter to the seminal vesicles and lower urinary tract anomalies, such as recto-ureteral fistula and strictures of the urethra. Recurrent epididymitis can also occur in boys with neurogenic bladder or functional bladder abnormalities.

25
Gray-scale US findings of epididymo-orchitis include an enlarged epididymis. The echotexture of the epididymis varies, depending on time of evolution, from decreased to increased echogenicity. Inflammation of the testis, orchitis, is confirmed by enlarged testis with heterogeneous echotexture. Indirect signs of inflammation, such as reactive scrotal wall edema and hydrocele, are present in most cases. Duplex US demonstrates hyperemia of the epididymis and, when orchitis is present, increased testicular perfusion.

26
Acute epididymitis

27
Epididymo-orchitis

Similar presentations