Download presentation
Presentation is loading. Please wait.

2
Management of Atrial Fibrillation
Dr.Ajmal Khan TMO Cardiology HMC

3
The Consequences of AF Thromboembolism Mortality Hospitalizations
Stroke: 4.5 increased risk Microemboli: reduced cognitive function Prothrombotic state Mortality 2 increased risk independent of comorbid CV disease Sudden death in HF and HCM Hospitalizations Most common arrhythmia requiring hospitalization 2-3 increased risk for hospitalization Impaired Hemodynamics Loss of atrial kick Irregular ventricular contractions HF Tachycardia-induced cardiomyopathy Reduced QoL Palpitations, dyspnea, fatigue, reduced exercise tolerance AF is an enormous contributor to the growing cost of medical care

4
Definition AF is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation with consequent deterioration of mechanical function. ECG shows, rapid oscillations, or fibrillatory waves that vary in amplitude, shape, and timing, replace consistent P waves, and there is an irregular ventricular response.

7
Classification Recurrent AF :(1) paroxysmal AF (2) persistent AF
(3) permanent AF
 permanent AF.")
8
Classification of Atrial Fibrillation ACC/AHA/ESC Guidelines
First Detected Paroxysmal (Self-terminating) Persistent (Not self-terminating) Permanent Fuster V, Rydén LE, Asinger RW, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation.) J Am Coll Cardiol. 2001;38:
 Persistent (Not self-terminating) Permanent. Fuster V, Rydén LE, Asinger RW, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation.) J Am Coll Cardiol. 2001;38:")
9
Epidemiology of Atrial Fibrillation
Most common sustained cardiac arrhythmia. 0.4% to 1% in the general population. 8% in those older than 80 y. Currently affects > 2.3 million Americans, or 1% of population. Preferentially affects men and the elderly . Prevalence expected to increase by ≥ 2.5-fold by Lifetime risk of developing AF: 1 in 4 for men and women ≥ 40 years of age . Page 9

10
Prevalence of Diagnosed AF
12 Women 11.1 Men 10.3 10 9.1 8 7.3 7.2 Prevalence (%) 6 5.0 5.0 4 3.4 3.0 2 1.7 1.7 1.0 0.9 0.2 0.4 0.1 < 55 55–59 60–64 65–69 70–74 75–79 80–84 ≥ 85 Age (years) 1.89 million adults in study population; N = 17,974 with AF Go AS, et al. JAMA. 2001;285:
 < –59. 60–64. 65–69. 70–74. 75–79. 80–84. ≥ 85. Age (years) 1.89 million adults in study population; N = 17,974 with AF. Go AS, et al. JAMA. 2001;285:")
11
Projected Number of Patients with AF by 2050
MarketScan and Thomson Reuters Medicare Databases, 2009 Olmsted County Data, 2006 (assuming a continued increase in AF incidence) 15.9 15.2 16 Olmsted County Data, 2006 (assuming no further increase in AF incidence) 14.3 13.1 14 ATRIA Study Data, 2000 11.7 12 10.2 12.1 11.7 8.9 11.1 10.3 7.7 Patients with AF (millions) 9.4 8 6.7 8.4 7.56 5.9 7.5 5.1 6 6.8 6.1 Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285: Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114: 5.6 5.42 5.61 4 5.1 5.16 4.78 3.03 4.34 3.80 3.33 2 2.66 2.94 2.44 2.08 1990 1995 2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050 Year ATRIA = Anticoagulation and Risk Factors in Atrial Fibrillation. Naccarelli GV, et al. Am J Cardiol. 2009;104(11):
 Olmsted County Data, (assuming no further increase in AF incidence) ATRIA Study Data, Patients with AF (millions) Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285: Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114: Year. ATRIA = Anticoagulation and Risk Factors in Atrial Fibrillation. Naccarelli GV, et al. Am J Cardiol. 2009;104(11):")
12
Etiologies and factors predisposing patients to AF
Electrophysiological abnormalities Enhanced automaticity (focal AF) Conduction abnormality (reentry) Atrial pressure elevation Mitral or tricuspid valve disease Myocardial disease (primary or secondary, leading to systolic or diastolic dysfunction) Semilunar valvular abnormalities (causing ventricular hypertrophy) Systemic or pulmonary hypertension (pulmonary embolism) Intracardiac tumors or thrombi Atrial ischemia Coronary artery disease
 Conduction abnormality (reentry) Atrial pressure elevation. Mitral or tricuspid valve disease Myocardial disease (primary or secondary, leading to systolic or diastolic dysfunction) Semilunar valvular abnormalities (causing ventricular hypertrophy) Systemic or pulmonary hypertension (pulmonary embolism) Intracardiac tumors or thrombi Atrial ischemia. Coronary artery disease")
13
Etiologies and factors predisposing patients to AF
Inflammatory or infiltrative atrial disease Pericarditis Amyloidosis Myocarditis Age-induced atrial fibrotic changes Drugs Alcohol Caffeine Endocrine disorders Hyperthyroidism Pheochromocytoma

14
Etiologies and factors predisposing patients to AF
Changes in autonomic tone Increased parasympathetic activity Increased sympathetic activity Primary or metastatic disease in or adjacent to the atrial wall Postoperative Cardiac, pulmonary, or esophageal Congenital heart disease Neurogenic Subarachnoid hemorrhage Nonhemorrhagic, major stroke Idiopathic (lone AF) Familial AF
 Familial AF.")
15
Diagnosis

16
CLINICAL FINDINGS History
Mild symptoms : palpitations ,sweating ,fatigue. Severe symptoms :hypotension ,myocardial ischemia ,myocardial dysfunctions ,stroke ,mesenteric ischemia ,lower limb ischemia Presentations of precipitating factors Asymptomatic

17
Examination Irregularly irregular pulse Pulse deficit
Also look for Hypertension ,Thyrotoxicosis ,CCF ,MS, Pulmonary diseases ,Other causative factors.

18
Clinical evaluation in patients with AF
Electrocardiogram, to identify Rhythm (verify AF) LV hypertrophy P-wave duration and morphology or fibrillatory waves Preexcitation Bundle-branch block Prior MI Other atrial arrhythmias To measure and follow the R-R, QRS, and QT intervals in conjunction with antiarrhythmic drug therapy
 LV hypertrophy P-wave duration and morphology or fibrillatory waves Preexcitation Bundle-branch block Prior MI Other atrial arrhythmias To measure and follow the R-R, QRS, and QT intervals in conjunction with antiarrhythmic drug therapy")
19
Clinical evaluation in patients with AF
Transthoracic echocardiogram, to identify Valvular heart disease LA and RA size LV size and function Peak RV pressure (pulmonary hypertension) LV hypertrophy LA thrombus (low sensitivity) Pericardial disease Blood tests of thyroid, renal, and hepatic function For a first episode of AF, when the ventricular rate is difficult to control
 LV hypertrophy LA thrombus (low sensitivity) Pericardial disease Blood tests of thyroid, renal, and hepatic function. For a first episode of AF, when the ventricular rate is difficult to control")
20
Clinical evaluation in patients with AF
Additional testing One or several tests may be necessary. Exercise testing If the adequacy of rate control is in question (permanent AF) To reproduce exercise-induced AF To exclude ischemia before treatment of selected patients with a type IC antiarrhythmic drug Holter monitoring or event recording If diagnosis of the type of arrhythmia is in question As a means of evaluating rate control Transesophageal echocardiography To identify LA thrombus (in the LA appendage)
 To reproduce exercise-induced AF To exclude ischemia before treatment of selected patients with a type IC antiarrhythmic drug Holter monitoring or event recording. If diagnosis of the type of arrhythmia is in question As a means of evaluating rate control Transesophageal echocardiography. To identify LA thrombus (in the LA appendage)")
21
Management

22
Goals of AF Management Reduction in the risk of CV events and hospitalizations and costs Prevention of thrombo-embolism Reduction of AF burden* QoL Symptoms Reduction in mortality

23
AFib Management Treatment Options
4/14/2017 9:24 PM AFib Management Treatment Options VENTRICULAR RATE CONTROL Pharmacologic Nonpharmacologic ACHIEVEMENT AND MAINTENANCE OF SINUS RHYTHM Pharmacologic Nonpharmacologic AFib Management Treatment Options Major treatment strategies for atrial fibrillation are listed here and include Ventricular rate control, mediated by drugs, devices or ablation Achievement and maintenance of sinus rhythm, mediated by cardioversion and/or antiarrhythmic drugs, and/or ablation Antithrombotic therapy to reduce the risk of thromboembolic complications, in combination with rate control, and as needed, with rhythm control The clinical history and cardiovascular comorbidities of the patient presenting with atrial fibrillation will dictate the most suitable treatment option ____________________ Miller JM, Zipes DP. Therapy for cardiac arrhythmias. In: Zipes DP, Libby P, Bonow RO, Braunwald E, eds. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 7th ed. Philadelphia, Pa: Elsevier Saunders; 2005;I: Fuster V, Ryden LE, Asinger RW, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences. J Am Coll Cardiol. 2001;38:1266i-1266lxx. ANTITHROMBOTIC THERAPY

24
Guideline-Based AF Treatment Options
Rate control Maintenance of SR Stroke prevention Pharmacologic CCBs -blockers Digitalis Amiodarone Dronedarone Nonpharmacologic Ablate and pace Pharmacologic Nonpharmacologic Pharmacologic Warfarin Aspirin +/- clopidogrel Dabigatran Factor Xa inhibitors Nonpharmacologic Removal/isolation LA appendage Class IA Class IC Class III -blockers Catheter ablation Pacing Surgery Implantable devices CCBs ACE-Is, ARBs Statins Fish oil Prevent remodeling 24

25
Rate and Rhythm Control Definitions
Rate control Rest and exertion control of ventricular response No commitment to maintaining SR Rhythm control Attempts restoration and maintenance of SR Rate control required as needed Can switch from rhythm control to rate control Difficult to switch from rate to rhythm control as duration of AF becomes longer ANTICOAGULATION NEEDED for either strategy Fuster V, et al. J Am Coll Cardiol. 2006;48: 25

26
Major Trials Comparing Rhythm Strategy and Rate Strategy
Major trials include AFFIRM RACE PIAF, STAF, HOT CAFE AF-CHF Page 26 26

27
Trials comparing rate control and rhythm control strategies in patients with AF
Reference Patients (n) AF duration Follow-up (y) Age (mean y ±SD) Clinical events (n) Stroke/embolism Death Rate Rhythm AFFIRM (2002) 128 4060 b/NR 3.5 70±9 88/2027 93/2033 310/2027 356/2033 RACE (2002) 124 522 1 to 399 d 2.3 68±9 7/256 16/266 18/256 18/266 PIAF (2000) 130 252 7 to 360 d 1 61±10 0/125 2/127 2/125
 AF duration. Follow-up (y) Age (mean y ±SD) Clinical events (n) Stroke/embolism. Death. Rate. Rhythm. AFFIRM (2002) b/NR ±9. 88/ / / /2033. RACE (2002) to 399 d ±9. 7/ / / /266. PIAF (2000) to 360 d ±10. 0/125. 2/127. 2/125.")
28
AFFIRM: All-Cause Mortality
30 Rate Rhythm 25 20 p=0.078 unadjusted 15 Mortality, % p=0.068 adjusted 10 5 1 2 3 4 5 Time (years) Rhythm N: 2033 1932 1807 1316 780 255 Rate N: 2027 1925 1825 1328 774 236 The AFFIRM Investigators. N Engl J Med. 2002;347:
 Rhythm N: Rate N: The AFFIRM Investigators. N Engl J Med. 2002;347:")
29
Canadian Cardiovascular Society Recommendations 2011
Favors Rate Control Favors Rhythm Control Persistent AF Paroxysmal AF Newly Detected AF Less Symptomatic More Symptomatic >65 years of age < 65 years of age Hypertension No Hypertension No History of Congestive Heart Failure Congestive Heart Failure clearly exacerbated by AF Previous Antiarrhythmic Drug Failure No Previous Antiarrhythmic Drug Failure

30
Cardioversion of AFib Pharmacological Electrical Early onset AFib
Long-standing AFib Electrical

31
Pharmacological Cardioversion

32
Our Goal

33
Pharmacological Cardioversion
More effective in recent-onset AFib Class IA-IC-III drugs administered IV Class IC favoured in non-cardiopathic patients Class III favoured in cardiopathic patients or those with delays in conduction Oral loading can be performed with class IC drugs Flecainide ( mg) Propafenone ( mg)
 Propafenone ( mg)")
34
Treatment Out-of-Hospital with Class IC Drugs
Symptomatic, rare episodes of AFib Recent onset AFib No structural heart disease Prior hospital experience Good physician-patient relationship Resting conditions for at least 4 hours

35
Pill-in-the-Pocket In a selected (no or mild HD), risk-stratified patient population with recurrent AFib not currently taking AADs 79% developed ≥ 1 episodes of recurrent AFib during 15 ± 5m follow-up Acute oral flecainide or propafenone successfully terminated 94% of episodes within 113 ± 84 min, with side effects in 7% of patients Alboni P, et al. N Engl J Med (2004) 351: 2384
 351:")
36
Amiodarone for Cardioversion of Recent-Onset AFib: Meta-analysis
Bolus only Bolus+infusion 100 95 Amiodarone IV (3-7 mg/kg ± infusion g/day) Amiodarone oral (25-30 mg/kg) Time to conversion > 6-8 h Amiodarone > 1.5 g/day IV > placebo Amiodarone mg/kg oral > placebo Amiodarone not > other AADs Safe in patients with structural cardiopathies and low LVEF 80 69 60 55 Conversion (%) 40 34 20 2-4 h 8 h
 Amiodarone oral (25-30 mg/kg) Time to conversion > 6-8 h. Amiodarone > 1.5 g/day IV > placebo. Amiodarone mg/kg oral > placebo. Amiodarone not > other AADs. Safe in patients with structural cardiopathies and low LVEF Conversion (%) h. 8 h.")
37
Electrical Cardioversion

38
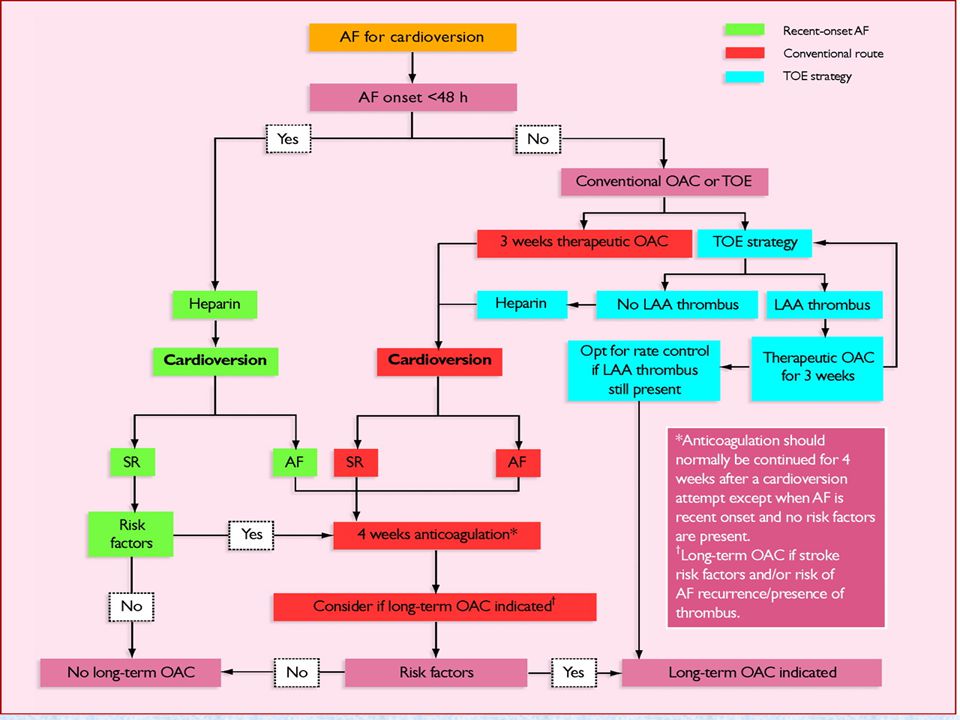
Indications Failure of pharmacological measures for patients with AF with ongoing myocardial ischemia, symptomatic hypotension, angina, or HF. Immediate direct-current cardioversion is recommended for patients with AF involving preexcitation when very rapid tachycardia or hemodynamic instability occurs. AF of <48hr ---cardioversion without prior anticoagulation. For high risk patients---IV UFH or LMWH before cardioversion. AF of > 48 hr or uncertain duration follow the protocol of anticoagulation.

40
2011 ACC/AHA/HRS Guidelines: Antiarrhythmic Approaches to Maintain SR in Patients with Recurrent PAF or Persistent AF* Maintenance of SR No (or minimal) heart disease HTN CAD HF Dronedarone Flecainide Propafenone Sotalol Substantial LVH Dofetilide Dronedrone Sotalol Amiodarone Dofetilide No Yes Amiodarone Dofetilide Catheter ablation Dronedarone Flecainide Propafenone Sotalol Amiodarone Amiodarone Catheter ablation Catheter ablation Dronedarone is added in parentheses here as a possible position in this table where it may become recommended in future guidelines statements. A Safety-Driven Approach Amiodarone Dofetilide Catheter ablation Catheter ablation
 heart disease. HTN. CAD. HF. Dronedarone. Flecainide Propafenone Sotalol. Substantial LVH. Dofetilide. Dronedrone Sotalol. Amiodarone Dofetilide. No. Yes. Amiodarone Dofetilide. Catheter ablation. Dronedarone. Flecainide Propafenone Sotalol. Amiodarone. Amiodarone. Catheter ablation. Catheter ablation. Dronedarone is added in parentheses here as a possible position in this table where it may become recommended in future guidelines statements. A Safety-Driven Approach. Amiodarone Dofetilide. Catheter ablation. Catheter ablation.")
41
Efficacy of AADs in AF Trials
100 Amiodarone Dronedarone 80 Sotalol Class IC 60 Placebo Patients in SR at 1 Year (%) 40 20 CTAF SAFE-T AFFIRM DAFNE* EURIDIS* ADONIS EURIDIS/ ADONIS Pooled DIONYSOS†
 CTAF. SAFE-T. AFFIRM. DAFNE* EURIDIS* ADONIS. EURIDIS/ ADONIS Pooled. DIONYSOS†")
42
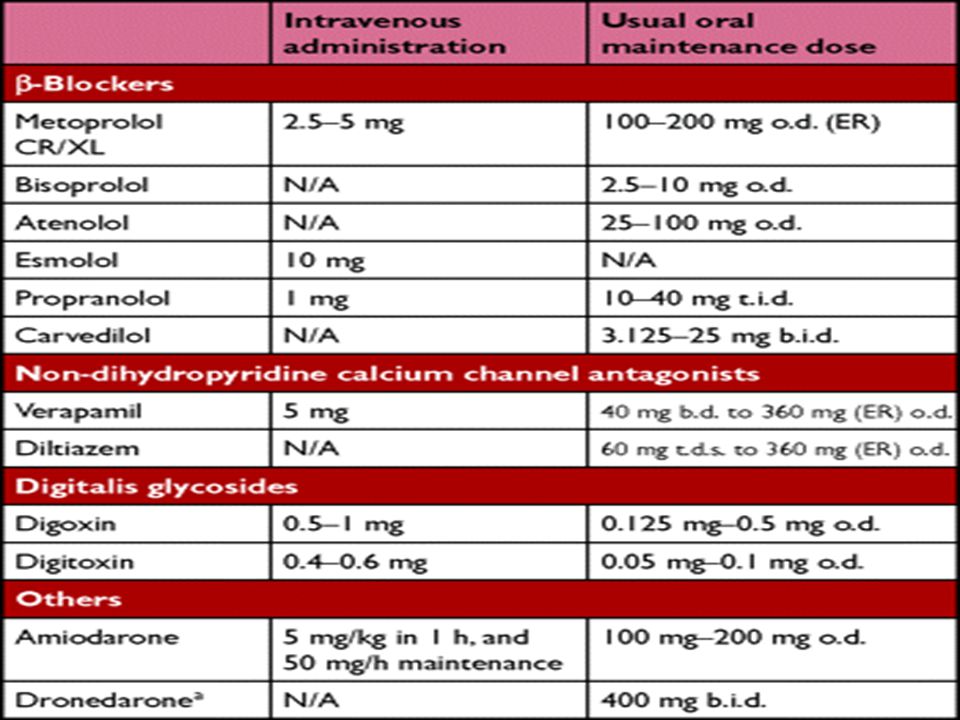
Treatment Options for AFib Drugs to Control Ventricular Rate

43
Permanent AFib and Ventricular Rate Control
Indications for control of ventricular rate: Failure of antiarrhythmic therapy for preventing recurrence Alternative treatment to maintain sinus rhythm

44
Canadian Cardiovascular Society Recommendations 2011
Favors Rate Control Favors Rhythm Control Persistent AF Paroxysmal AF Newly Detected AF Less Symptomatic More Symptomatic >65 years of age < 65 years of age Hypertension No Hypertension No History of Congestive Heart Failure Congestive Heart Failure clearly exacerbated by AF Previous Antiarrhythmic Drug Failure No Previous Antiarrhythmic Drug Failure

46
Anticoagulation and Antiplatelet Therapy

47
AF and Stroke AF increases stroke risk 4- to 5-fold
Stroke is the most common and devastating complication of AF Incidence of all-cause stroke in patients with AF is 5% AF is an independent risk factor for stroke. Risk for stroke increases with age Stroke risk persists even in asymptomatic AF Stroke risk persists in patients with a “high-risk” profile despite a strategy of rhythm control (AFFIRM study, RACE study) Annual Stroke Rate (%) 10 8 6 4 2 Permanent AF Intermittent AF AFib is an independent risk factor for stroke; in fact, it increases the risk of stroke approximately 5-fold.1,2 It is estimated that 15% of all strokes in the United States are attributable to AFib, and the proportion increases markedly with age.1 Additionally, ischemic stroke associated with AFib is often more severe than stroke due to other causes.3 A retrospective study determined that those with AFib were more likely than those without AFib to be bedridden following a stroke (41.2% vs 23.7%, P<.0005).3 Finally, asymptomatic, or “silent,” AFib is common and may also increase the risk of stroke.4 Moderate Risk High Risk Low Risk 1. Fuster V, Rydén LE, Asinger RW, et al. ACC/AHA/ESC guidelines for the management of patients with AF: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With AF) developed in collaboration with the North American Society of Pacing and Electrophysiology. J Am Coll Cardiol. 2001;38: 2. Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of AF on the risk of death: the Framingham Heart Study. Circulation. 1998;98: 3. Dulli DA, Stanko H, Levine RL. AF is associated with severe acute ischemic stroke. Neuroepidemiology. 2003;22: 4. Page RL, Tilsch TW, Connolly SJ, et al. Asymptomatic or “silent” AF: frequency in untreated patients and patients receiving azimilide. Circulation. 2003;107: ©2008 sanofi-aventis U.S. LLC Page 47
 Annual Stroke Rate (%) Permanent AF. Intermittent AF. AFib is an independent risk factor for stroke; in fact, it increases the risk of stroke approximately 5-fold.1,2 It is estimated that 15% of all strokes in the United States are attributable to AFib, and the proportion increases markedly with age.1 Additionally, ischemic stroke associated with AFib is often more severe than stroke due to other causes.3 A retrospective study determined that those with AFib were more likely than those without AFib to be bedridden following a stroke (41.2% vs 23.7%, P<.0005).3 Finally, asymptomatic, or silent, AFib is common and may also increase the risk of stroke.4. Moderate Risk. High Risk. Low. Risk. 1. Fuster V, Rydén LE, Asinger RW, et al. ACC/AHA/ESC guidelines for the management of patients with AF: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With AF) developed in collaboration with the North American Society of Pacing and Electrophysiology. J Am Coll Cardiol. 2001;38: Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of AF on the risk of death: the Framingham Heart Study. Circulation. 1998;98: Dulli DA, Stanko H, Levine RL. AF is associated with severe acute ischemic stroke. Neuroepidemiology. 2003;22: Page RL, Tilsch TW, Connolly SJ, et al. Asymptomatic or silent AF: frequency in untreated patients and patients receiving azimilide. Circulation. 2003;107: ©2008 sanofi-aventis U.S. LLC. Page 47.")
48
Approach to thromboprophylaxis in patients with AF

49
Stroke Risk Stratification in AF
CHADS2 Risk criteria score Risk Factor Score Cardiac failure 1 HTN Age ≥75 y Diabetes Stroke 2 Lip GY, Halperin JL. Am J Med. 2010;123(6): 49
:")
50
CHAD2 score and stroke rate

51
Less validated or weaker risk factors Moderate-risk factors
High-risk factors Female gender Age greater than or equal to 75 y Previous stroke, TIA or embolism Age 65 to 74 y Hypertension Mitral stenosis Coronary artery disease Heart failure Prosthetic heart valvea Thyrotoxicosis LV ejection fraction 35% or less Diabetes mellitus

52
Antithrombotic therapy for patients with atrial fibrillation
Risk category Recommended therapy No risk factors Aspirin, 81 to 325 mg daily One moderate-risk factor Aspirin, 81 to 325 mg daily, or warfarin (INR 2.0 to 3.0, target 2.5) Any high-risk factor or more than 1 moderate-risk factor Warfarin (INR 2.0 to 3.0, target 2.5)
 Any high-risk factor or more than 1 moderate-risk factor. Warfarin (INR 2.0 to 3.0, target 2.5)")
53
Stroke Prevention in AF
Warfarin vs Placebo in Stroke Prevention in AF AFASAK-1 SPAF BAATAF CAFA SPINAF EAFT ALL Trials 100% % % % % Favors Warfarin Favors Placebo/ Control Warfarin reduces incidence of stroke by about 64% Hart R, et al. Ann Intern Med. 2007;146:

54
Antiplatelet Therapy in AF
ACTIVE-W: 6706 randomized patients; trial stopped Clopidogrel +ASA Warfarin P = .0003 6 5 4 Outcome/Year (%) 3 P = .001 P = .53 2 1 Vascular Event Stroke Major Bleeding ACTIVE = AF Clopidogrel Trial with Irbesartan for Prevention of Vascular Events.
 3. P = P = Vascular Event. Stroke. Major Bleeding. ACTIVE = AF Clopidogrel Trial with Irbesartan for Prevention of Vascular Events.")
55
Antiplatelet Therapy in AF
ACTIVE-A: 7554 randomized patients; median follow-up of 3.6 years P = .01 8 Clopidogrel +ASA 7 ASA 6 5 Outcome/Year (%) 4 P<.001 3 P<.001 2 1 Vascular Event Stroke Major Bleeding Active = AF Clopidogrel Trial with Irbesartan for Prevention of Vascular Events. ACTIVE Investigators. N Engl J Med. 2009;360(20):
 4. P< P< Vascular Event. Stroke. Major Bleeding. Active = AF Clopidogrel Trial with Irbesartan for Prevention of Vascular Events. ACTIVE Investigators. N Engl J Med. 2009;360(20):")
56
NEW ANTICOAGULANTS

57
Characteristics of new oral anticoagulants
Agent Mechanism of Action Dosing Onset Half Life Reversibility Clinical Development Apixaban Direct factor Xa inhibitor Oral 2x daily 3 hr 12 hr No Phase 3; ARISTOTLE, AVERROES Rivaroxaban 1–2x daily 9 hr Phase 3; ROCKET AF DU 176b 1–2 hr 9–11 hr Phase 3; ENGAGE-AF Betrixaban Not reported 19 hr Phase 2; EXPLORE Xa YM 150 Phase 2 Idrabiotaparinux Indirect factor Xa inhibitor Weekly SC Injection 80–130 hr Yes, IV avidin Phase 3; BOREALIS–AF Dabigatran etexilate Direct thrombin inhibitor 12–17 hr Phase 3; RE–LY AZD 0837 1 hr ATI-5923 Tecarfarin Vitamin K antagonist Variable Oral 1x daily 136 hr Yes, vitamin K Phase 2/3; EMBRACE AC Sobieraj-Teague M, et al. Semin Thromb Hemost. 2009;35:

58
Stroke Prevention in Atrial Fibrillation
Dabigatran etexilate vs warfarin (RE-LY) 4.00 Dabigatran 110 mg 3.50 Dabigatran 150 mg Warfarin INR 2.0–3.0 3.00 † Dabigatran vs warfarin * P < Non-inferiority **P < Non-inferiority, superiority †P = 0.003 ††P < 0.001 § P < 0.001 2.50 Percent/Year 2.00 * 1.50 ** 1.00 0.50 †† 0.00 Stroke/Systemic Major Bleed Intracranial Embolism Hemorrhage Connolly S, et al. N Engl J Med. 2009;361:
 Dabigatran 110 mg Dabigatran 150 mg. Warfarin INR 2.0– † Dabigatran vs warfarin. * P < Non-inferiority. **P < Non-inferiority, superiority. †P = ††P < § P < Percent/Year * ** †† Stroke/Systemic. Major Bleed. Intracranial. Embolism. Hemorrhage. Connolly S, et al. N Engl J Med. 2009;361:")
59
AVERROES Trial E R ASA (81-324 mg daily; up to 36 mo/end of study)
Unsuitable for warfarin therapy N= 5600 E R Double-blind Apixaban (5 mg twice daily; 2.5 mg in selected patients up to 36 mo/end of study) AVERROES, Apixaban Versus ASA to Reduce the Risk Of Stroke.
 AVERROES, Apixaban Versus ASA to Reduce the Risk Of Stroke.")
60
AVERROES: Stroke or Systemic Embolic Event
95% CI, P<.001 0.05 ASA Cumulative Risk 0.03 Apixaban* 0.01 0.0 3 6 9 12 18 21 Months No. at Risk ASA 2791 2720 2541 2124 1541 626 329 Apix 2809 2761 2567 2127 1523 617 353

61
Clinical Challenges With New Anticoagulants
No validated tests to measure anticoagulation effect No established therapeutic range No antidote for most agents Assessment of compliance more difficult than with vitamin K antagonists Potential for unknown long-term adverse events Balancing cost against efficacy Lack of head-to-head studies comparing new agents

62
Catheter AF Ablation Indications:
Symptomatic AF refractory or intolerant to at least 1 class I or III AAD. Selected symptomatic patients with HF and/or reduced ejection fraction Presence of an LA thrombus is contraindication to catheter ablation of AF Discontinuation of anticoagulation is not an indication for ablation CARD Progress Indicators 9. Recognize ablation as an option for treating patients with AF. (knowledge — for PCPs and GenCards only) Learning Objectives 3. Select the optimal treatment strategy—ie, appropriate pharmacotherapy (including antiarrhythmic therapy), ablation—for patients with AF based on patient characteristics [Progress Indicators 6, 9, 11] and make appropriate referral for ablation [Progress Indicator 10] Instructional Objectives 9. Presented with treatment options for AF patients, participants will recognize ablation as an acceptable option PCP 5. Select the optimal treatment strategy—ie, appropriate pharmacotherapy (including antiarrhythmic therapy), ablation—for patients with AF based on patient characteristics [Progress Indicators 6, 9, 11]
 Learning Objectives. 3. Select the optimal treatment strategy—ie, appropriate pharmacotherapy (including antiarrhythmic therapy), ablation—for patients with AF based on patient characteristics [Progress Indicators 6, 9, 11] and make appropriate referral for ablation [Progress Indicator 10] Instructional Objectives. 9. Presented with treatment options for AF patients, participants will recognize ablation as an acceptable option. PCP. 5. Select the optimal treatment strategy—ie, appropriate pharmacotherapy (including antiarrhythmic therapy), ablation—for patients with AF based on patient characteristics [Progress Indicators 6, 9, 11]")
63
Common Lesions Performed in AF Ablation
A. Circumferential ablation around left and right PV antra B. and C. Additional linear lesion sets for the roof, mitral isthmus, carinae, SVC, and cavotricuspid isthmus D. Targeting fractionated electrograms and/or ganglionic plexi SVC SVC A. B. RSPV RSPV LSPV LSPV LIPV LIPV RIPV RIPV IVC IVC SVC SVC C. D. RSPV RSPV LSPV LSPV LIPV RIPV LIPV RIPV IVC IVC

64
Treatment of atrial fibrillation in special population

65
Management of atrial fibrillation associated with the Wolff-Parkinson-White (WPW) preexcitation syndrome Immediate direct-current cardioversion is recommended in hemodynamically unstable patients. Intravenous procainamide , ibutilide ,flecainide or amiodarone is recommended to restore sinus rhythm in hemodynamically stable patients. Intravenous administration of AV nodal blocking drugs i.e. digitalis glycosides or nondihydropyridine calcium channel antagonists is not recommended. Catheter ablation of the accessory pathway is recommended in symptomatic patients.

66
Hyperthyroidism Administration of a beta blocker to control the rate of ventricular response . Alternative is nondihydropyridine calcium channel antagonist (diltiazem or verapamil). Oral anticoagulation (INR 2.0 to 3.0) is recommended in the presence of risk factors for stroke.
. Oral anticoagulation (INR 2.0 to 3.0) is recommended in the presence of risk factors for stroke.")
67
Management of atrial fibrillation during pregnancy
Digoxin, a beta blocker, or nondihydropyridine calcium channel to control the rate . Flecainide , ibutilide , quinidine or procainamide to restore sinus rhythm in hemodynamically stable patient. Direct-current cardioversion in hemodynamically unstable patient. Anticoagulation in the presence of risk factor for stroke.

68
Management of atrial fibrillation in patients with pulmonary disease
Correction of hypoxemia and acidosis . A nondihydropyridine calcium channel antagonist (diltiazem or verapamil) to control the ventricular rate. Direct-current cardioversion in hemodynamically unstable patient. IV flecainide may be used to restore sinus rhythm in hemodynenicall y stable patient.
 to control the ventricular rate. Direct-current cardioversion in hemodynamically unstable patient. IV flecainide may be used to restore sinus rhythm in hemodynenicall y stable patient.")
69
Interruption of anticoagulation for diagnostic or therapeutic procedures
Anticoagulation may be interrupted for a period of up to 1 wk for surgical or diagnostic procedures. In high-risk patients (particularly those with prior stroke, TIA, or systemic embolism), or when a series of procedures requires interruption of oral anticoagulant therapy for longer periods, unfractionated or low-molecular-weight heparin may be administered.
, or when a series of procedures requires interruption of oral anticoagulant therapy for longer periods, unfractionated or low-molecular-weight heparin may be administered.")
70
Summary AF is a common disease that is increasing in prevalence
For any patient with AF, decisions need to be made regarding antithrombotic therapy, rate control, and/or rhythm control Guidelines provide recommendations for the management of patients with AF Anticoagulation is essential in AF patients with risk markers, regardless of any restoration of SR New agents and procedures may provide antiarrhythmic and antithrombotic options with improved outcomes for managing AF

71
Thank you for your attention!

Similar presentations




 -Pt acutely unwell with palpitations -Pt with haemodyanically unstable acute onset AF -2 nd /3 rd heart block -Exercise.>")
















, Greater Glasgow and Clyde Honorary Clinical Lecture, University of Strathclyde.>")