Download presentation
Presentation is loading. Please wait.

1
Matrix Model of Outpatient Treatment for Substance Dependence
Originally Developed Specifically For Stimulant Abuse and Dependence METH SUMMIT May 19-21, 2003 Fargo, North Dakota Ahndrea Weiner M.S., LMFT Clinical Director Matrix Institute on Addictions

2
Methamphetamine Treatment Admissions
In 1993, amphetamine treatment admission rates were high in a few Western States - - California, Oregon, Hawaii and Nevada. By 1999, high amphetamine treatment admission rates were seen in most States west of the Mississippi. Between 1993 and 1999, amphetamine treatment admission rates increased by 250 percent or more in 14 States and by 100 to 249 percent in another 10 States. Methamphetamine is the primary form of amphetamine seen in the United States and made up 94 percent of all amphetamine treatment admissions reported to SAMHSA's Treatment Episode Data Set (TEDS) in 1999.
 in")
3
Definition of Effectiveness
The degree to which a therapeutic technique decreases the amount of frequency of drug or alcohol use, promotes prosocial behavior change compatible with a drug-free lifestyle and/or increases the engagement or retention of patients in process of treatment or self-help.

4
Treatment Medical & Behavioral
Drugs Sedatives Stimulants Opioids Alcohol Medical Treatment Yes No Behavioral Treatment Yes

5
www.drugabuse.gov Principles of Drug Addiction Treatment
Three decades of scientific research and clinical practice have yielded a variety of effective approaches to drug addiction treatment. In April 1998, NIDA held The National Conference on Drug Addiction Treatment: From Research to Practice which summarized this extensive body of research. Based on the findings reported at this conference, NIDA published in October 1999, Principles of Drug Addiction Treatment: A Research-Based Guide to foster more widespread use of scientifically-based components of drug addiction treatment. Key components of this guide are highlighted in the following slides.

6
Manuals in Psychosocial Treatment
Reduce therapist differences Ensure uniform set of services Can more easily be evaluated Enhance training capabilities Facilitate research to practice

7
Matrix Model An Integrated, Empirically-based, Manualized Treatment Program

8
Motivation for Treatment
Why is it harder for a stimulant abuser to enter the treatment system? What does it mean to say someone is motivated to do treatment? How can we compete with the pull of drugs like methamphetamine?

9
Methamphetamine Withdrawal
Depression Difficulty Concentrating Severe Cravings Paranoia Exhaustion Confused

10
How Stimulants Effect the Willingness to Enter Treatment
Methamphetamine does NOT make you sick; therefore, the drug use is not the problem. Methamphetamine allows long periods of no drug use; certainly the drug is not the problem.

11
What Research Tells Us about Addiction
People with drug and alcohol dependencies do not have unique personalities

12
What Research Tells Us about Denial
People with dependencies show no higher level of denial than the normal population Measures of denial are not clearly related to treatment or outcome

13
What Research Tells Us about Treatment
Patient drug use, compliance, and outcome are powerfully influenced by therapist characteristics and environment Direct confrontation yields poorer compliance and outcomes

14
Assumptions in Working with Mandated Clients

15
Assumptions in Working with Mandated Clients
The stick is enough. There is no need for a carrot.

16
Assumptions in Working with Mandated Clients
Clients are either motivated or not. If they are not, there is little we can do.

17
Assumptions in Working with Mandated Clients
People change only when they have to. The first and most important step in recovery is to admit and accept the fact that you have the disease of addiction.

18
Assumptions in Working with Mandated Clients
Someone who continues to use is “in denial.” The best way to “break through” the denial is direct confrontation.

19
Motivational Goals Increase Motivation Decrease Resistance
Increase retention Better outcomes

20
Four Principles of Motivational Interviewing
1. Express empathy 2. Develop discrepancy 3. Avoid argumentation 4. Support self-efficacy

21
1. Express Empathy Acceptance facilitates change
Skillful reflective listening is fundamental Ambivalence is normal

22
2. Develop Discrepancy Awareness of consequences is important
Discrepancy between behaviors and goals motivates change Have the client present reasons for change

23
3. Avoid Argumentation Resistance is signal to change strategies
Labeling is unnecessary Shift perceptions Clients attitudes shaped by their words, not yours

24
4. Support Self-Efficacy
Belief that change is possible is important motivator Client is responsible for choosing and carrying out actions to change There is hope in the range of alternative approaches available

25
MATRIX MODEL TREATMENT
INFORMATION/EDUCATION

26
Triggers & Cravings Slide 1 Introduction:
Understanding and dealing with triggers and cravings is critically important in order to understand the seemingly irrational behavior of the active addict/alcoholic, and to begin the first steps in recovery. Triggers cause cravings, and cravings lead to using or drinking. Common sense would suggest that being around people, places, or situations that have resulted in past use, might increase the chances of using/drinking again. The additional influence that these triggers have upon the brain makes the advice to avoid triggers more than just a good idea; there is no other way to reliably avoid cravings and relapse. This lecture describes the development of the craving process with regard to the underlying effects drugs and alcohol have upon the brain. Our hope is that an understanding of this process will allow both patients and families to view the addiction in a new and more understandable way as well as to see what is behind much of the advice given to patients early in treatment.

27
Slide 3: Brain regions and neuronal pathways
Certain parts of the brain govern specific functions. Point to areas such as the sensory (orange), motor (blue) and visual cortex (yellow) to highlight their specific functions. Point to the cerebellum (pink) for coordination and to the hippocampus (green) for memory. Indicate that nerve cells or neurons connect one area to another via pathways to send and integrate information. The distances that neurons extend can be short or long. For example; point to the reward pathway (orange). Explain that this pathway is activated when a person receives positive reinforcement for certain behaviors ("reward"). Indicate that you will explain how this happens when a person takes an addictive drug. As another example, point to the thalamus (magenta). This structure receives information about pain coming from the body (magenta line within the spinal cord), and passes the information up to the cortex. Tell the audience that you can look at this in more detail.
, motor (blue) and visual cortex (yellow) to highlight their specific functions. Point to the cerebellum (pink) for coordination and to the hippocampus (green) for memory. Indicate that nerve cells or neurons connect one area to another via pathways to send and integrate information. The distances that neurons extend can be short or long. For example; point to the reward pathway (orange). Explain that this pathway is activated when a person receives positive reinforcement for certain behaviors ( reward ). Indicate that you will explain how this happens when a person takes an addictive drug. As another example, point to the thalamus (magenta). This structure receives information about pain coming from the body (magenta line within the spinal cord), and passes the information up to the cortex. Tell the audience that you can look at this in more detail.")
28
Trigger Definition A trigger is a stimulus which has been repeatedly associated with the preparation for, anticipation of or the use of drugs and/or alcohol. These stimuli include people, things, places, times of day, and emotional states. Slide 2 Definition of a trigger.

29
Triggers and Cravings Pavlov’s Dog Slide 9
Pavlov would feed dogs and ring a bell at the same time. The dogs would see and smell the food which would then stimulate, or trigger, their lower brains ( the autonomic nervous systems) causing the dogs to produce saliva and secrete gastric fluids in anticipation of digestion. In a relatively short amount of time, Pavlov and his colleagues would ring the bell without the presence of food, and the dogs would still produce saliva and gastric fluid as if food were present. The dogs connected the sound of the bell, the trigger, with anticipation of eating, and responded involuntarily physically to the powerful trigger, or stimulus, of the bell. Once a dog has been conditioned in this way, no matter how smart or well-trained the dog is, a dog will continue to produce fluids at the sound of the bell. He has no choice. The human brain responds in exactly the same way to the conditioned drugs and alcohol triggers that produce cravings. Drugs and alcohol produce changes in the brain, which result in feelings of pleasure. When triggers cause a person to experience cravings, the brain responds as if the actual chemicals are taken into the system. In other words, the brain is “drooling” in reaction to these triggers. This reaction occurs whether or not the person intends to use. The only way that Pavlov’s dog can avoid drooling is by avoiding the bell. The chemically dependent person can also avoid his or her brain’s reaction by avoiding triggers. Pavlov’s Dog
 causing the dogs to produce saliva and secrete gastric fluids in anticipation of digestion. In a relatively short amount of time, Pavlov and his colleagues would ring the bell without the presence of food, and the dogs would still produce saliva and gastric fluid as if food were present. The dogs connected the sound of the bell, the trigger, with anticipation of eating, and responded involuntarily physically to the powerful trigger, or stimulus, of the bell. Once a dog has been conditioned in this way, no matter how smart or well-trained the dog is, a dog will continue to produce fluids at the sound of the bell. He has no choice. The human brain responds in exactly the same way to the conditioned drugs and alcohol triggers that produce cravings. Drugs and alcohol produce changes in the brain, which result in feelings of pleasure. When triggers cause a person to experience cravings, the brain responds as if the actual chemicals are taken into the system. In other words, the brain is drooling in reaction to these triggers. This reaction occurs whether or not the person intends to use. The only way that Pavlov’s dog can avoid drooling is by avoiding the bell. The chemically dependent person can also avoid his or her brain’s reaction by avoiding triggers. Pavlov’s Dog.")
30
Cognitive Process During Addiction
Introductory Phase Relief From Depression Anxiety Loneliness Insomnia Euphoria Increased Status Increased Energy Increased Sexual/Social Confidence Increased Work Output Increased Thinking Ability May Be Illegal May Be Expensive Hangover/Feeling Ill May Miss Work AOD Slide 12 Alcohol and other drug (AOD) use is relatively infrequent during the Introductory Phase of the cognitive process of addiction. It may be limited to a few times a year, by chance or on special occasions. The positives of AOD use seem to outweigh the negatives.
 use is relatively infrequent during the Introductory Phase of the cognitive process of addiction. It may be limited to a few times a year, by chance or on special occasions. The positives of AOD use seem to outweigh the negatives.")
31
Conditioning Process During Addiction
Introductory Phase Strength of Conditioned Connection Mild Triggers Parties Special Occasions Responses Pleasant Thoughts about AOD No Physiological Response Infrequent Use Slide 13 Unknowingly, the AOD user is conditioning his brain every time a dose of his/her drug of choice is ingested. There is no automatic limbic response associating people, places or times with AOD use.

32
Development of Obsessive Thinking Introductory Phase
Sports Food School TV Girlfriend Hobbies Job AOD Family Exercise Parties Slide 14 During this Introductory Phase, AOD use is one small component of a person’s overall thought process.

33
Development of Craving Response
Introductory Phase Entering Using Site Use of AODs AOD Effects Heart/Pulse Rate Respiration Adrenaline Energy Taste Slide 15 Craving response is the combined experiences of AOD triggers activating the limbic system and the continuing AOD thoughts associated with these triggers. During this Introductory Phase, the limbic system is activated directly AODs, and depending upon whether the substance is a stimulant or a depressant, results in the increase or decrease of physiological arousal.

34
Cognitive Process During Addiction
Abuse Phase Vocational Disruption Relationship Concerns Financial Problems Beginnings of Physiological Dependence Depression Relief Confidence Boost Boredom Relief Sexual Enhancement Social Lubricant Slide 16 During the Maintenance Phase of the cognitive process during addiction, the frequency of AOD use increases, to perhaps, monthly or weekly. In terms of effects and negative consequences, the scales are beginning to lean more in the negative direction.

35
Abuse Phase Conditioning Process During Addiction
Strength of Conditioned Connection Triggers Parties Friday Nights Friends Concerts Alcohol “Good Times” Sexual Situations Responses Thoughts of AOD Eager Anticipation of AOD Use Mild Physiological Arousal Cravings Occur as Use Approaches Occasional Use Moderate Slide 17 Conditioning has begun. The people, places and things associated with AOD use have become triggers. Exposure to these triggers causes thoughts about AOD use. These thoughts originating in the brain are mild physiological reactions producing drives to find and use AODs.

36
Development of Obsessive Thinking
Abuse Phase AOD Food School TV Girlfriend Hobbies Job Family Exercise Parties Slide 18 Thoughts of AOD use begin to occur more frequently.

37
Development of Craving Response Physiological Response
Abuse Phase Entering Using Site Physiological Response Use of AODs AOD Effects Heart Rate Breathing Effects Adrenaline Effects Energy Taste Heart Blood Pressure Energy Slide 19 A mild physiological arousal occurs in situations closely associated with AOD use. As the person encounters AOD triggers, the limbic system is activated and AOD cravings occur. When drugs and/or alcohol are finally ingested, a concurrent physiological state (arousal or quiescence in relation to the properties of the drug ingested) will usually occur.
 will usually occur.")
38
Cognitive Process During Addiction
Addiction Phase Social Currency Occasional Euphoria Relief From Lethargy Relief From Stress Nose Bleeds Infections Relationship Disruption Family Distress Impending Job Loss Slide 20 During the Disenchantment Phase of the cognitive process of a developing addiction, the scales tip from the positive to the negative. The consequences of AOD use are severe and the user’s life begins to become unmanageable. At this point the cortical rational decision is to stop using, but the cortex is not in control any longer. Thinking, evaluating, and decision making appear to be happening, but behavior is contradictory. The user may sincerely resolve to quit using, and yet, may find himself out of control at the first thought of AODs, the first encounter with a fellow user, or at the availability of cash or other potent triggers.

39
Addiction Phase Conditioning Process During Addiction
Strength of Conditioned Connection Triggers Weekends All Friends Stress Boredom Anxiety After Work Loneliness Responses Continual Thoughts of AOD Strong Physiological Arousal Psychological Dependency Strong Cravings Frequent Use STRONG Slide 21 It is usually at this point that a person crosses the line into addiction. Despite the negative consequences of continued AOD use the addiction is evidenced by the loss of rational control. Triggers in this phase produce a powerful physiological response that drives the user to acquire and use AODs. The higher rational brain is observing that it makes to use anymore.

40
Development of Obsessive Thinking
Addiction Phase AOD Food TV Girlfriend Job Family Parties Slide 22 During the Disenchantment Phase, the frequency of AOD thinking increases, which begins to crowd out thoughts of other aspects in life.

41
Development of Craving Response
Addiction Phase Thinking of Using Mild Physiological Response Entering Using Site Heart Rate Breathing Rate Energy Adrenaline Effects Powerful Physiological Response Use of AODs AOD Effects Slide 23 In this phase, the craving response is a powerful event. The person feels an overpowering physical reaction in situations further and further removed from the drugs themselves. The craving response is almost as powerful as the actual AOD’s physical reaction. Heart Rate Breathing Rate Energy Adrenaline Effects Heart Blood Pressure Energy

42
Cognitive Process During Addiction Severe Dependency Phase
Relief From Fatigue Relief From Stress Relief From Depression Weight Loss Paranoia Loss of Family Seizures Severe Depression Unemployment Bankruptcy Slide 24 In the Disaster Phase, the AOD use is often robotic and automatic. There is no rational restraint upon the drug use; it makes no sense at all. The user’s behavior in the phase is much like the behavior of addicted laboratory animals that use drugs until they die.

43
Conditioning Process During Addiction Severe Dependency Phase
Strength of Conditioned Connection OVERPOWERING Responses Obsessive Thoughts About AOD Powerful Autonomic Response Powerful Physiological Dependence Automatic Use Triggers Any Emotion Day Night Work Non-Work Slide 25 Here the person is either using daily or in binges, which most likely will be interrupted by physical collapse, hospitalization, or arrest. The constant powerful craving from the limbic system and/or severe physiological dependency overwhelms the cortex.

44
Development of Obsessive Thinking Severe Dependency Phase
AOD Slide 26 Thoughts of AODs dominate the user’s consciousness.

45
Development of Craving Response
Severe Dependency Phase Thoughts of AOD Using Place Powerful Physiological Response Heart Rate Breathing Rate Energy Adrenaline Effects Slide 27 In the Disaster Phase, the craving can often be compared to actual AOD effects, and in some cases, these powerful effects may be the result of merely thinking about certain drugs.

46
IMPLEMENTING MATRIX MODEL OUTPATIENT TREATMENT

47
MATRIX TREATMENT MODEL Different from Residential Treatment
Less confrontational Progresses more slowly Focus is on present “Core Issues” not immediately addressed Allegiance is to therapist (vs. group)
")
48
MATRIX TREATMENT MODEL Different from Residential Treatment
Nonjudgmental attitude is basis of client-therapist bond Change recommendations based on scientific data Changes incorporated immediately into lifestyle

49
MATRIX TREATMENT MODEL Different from General Therapy
Focus on behavior vs. feelings Visit frequency results in strong transference Transference is encouraged Transference is utilized Goal is stability (vs. emotional catharsis)
")
50
MATRIX TREATMENT MODEL Different from General Therapy
Focus is on abstinence Bottom line is always continued abstinence Therapist frequently pursues less motivated clients The behavior is more important than the reason behind it

51
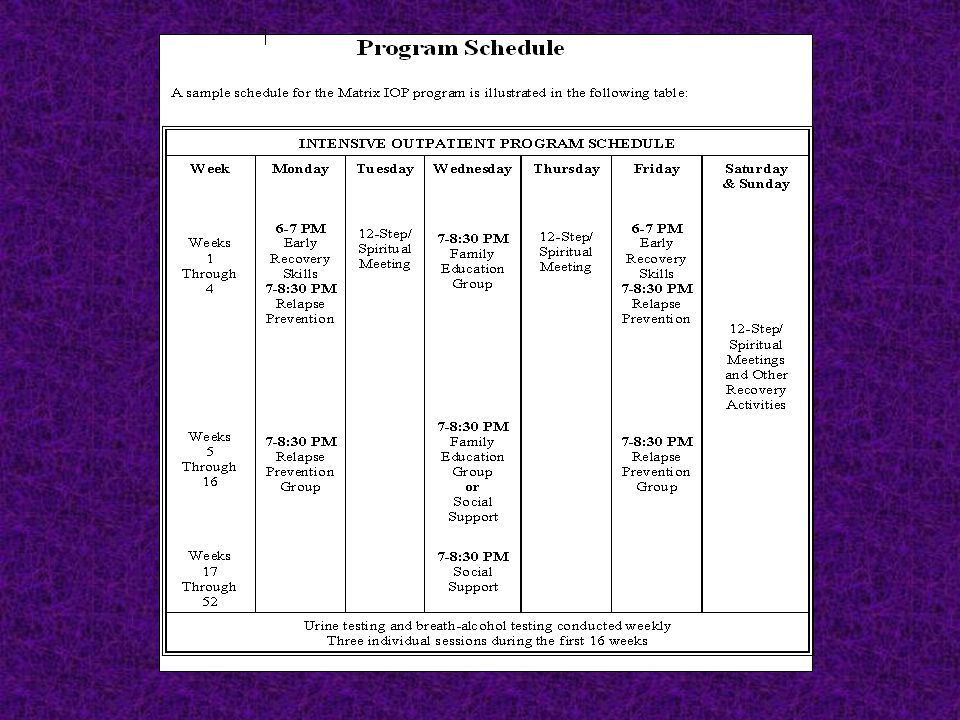
Treatment Components of the Matrix Model
Individual Sessions Early Recovery Groups Relapse Prevention Groups Family Education Group 12-Step Meetings Social Support Groups Relapse Analysis Urine Testing MATRIX

52
MATRIX MODEL OF OUTPATIENT TREATMENT
Organizing Principles of Matrix Treatment Create explicit structure and expectations Establish positive, collaborative relationship with patient Teach information and cognitive-behavioral concepts Positively reinforce positive behavior change

53
MATRIX MODEL OF OUTPATIENT TREATMENT
Organizing Principles of Matrix Treatment (cont.) Provide corrective feedback when necessary Educate family regarding stimulant abuse recovery Introduce and encourage self-help participation Use urinalysis to monitor drug use
 Provide corrective feedback when necessary. Educate family regarding stimulant abuse recovery. Introduce and encourage self-help participation. Use urinalysis to monitor drug use.")
54
COMPONENTS OF THE MATRIX MODEL Groups
Early Recovery Relapse Prevention Family Education Lectures

55
COMPONENTS OF THE MATRIX MODEL Other
Social Support Conjoint Sessions Urine Testing Relapse Analysis

57
EARLY RECOVERY GROUP Goals
To provide structured place for new patients to learn about recovery skills and self-help programs. Introduce patients to basic tools of recovery. To introduce outside involvement and create an expectation of participation as part of Matrix treatment.

58
EARLY RECOVERY GROUP Goals
Help patients adjust to participating in groups at Matrix and outside. Allow the patient co-leader to provide a model for gaining initial abstinence. Provide the patient co-leader with increased self-esteem and reinforce his or her progress.

59
EARLY RECOVERY GROUP Topics Scheduling and Calendars Triggers
Questionnaires and Chart 12 Step Introduction Alcohol Issues Thoughts Emotions and Behaviors KISS (and other 12-step slogans)
")
60
RELAPSE PREVENTION GROUP
Goals To allow clients to interact with other people in recovery. To present specific relapse prevention material. To allow co-leader to share long term sobriety experience.

61
RELAPSE PREVENTION GROUP
Goals (continued) To produce some groups cohesion among clients To allow group leader to witness interpersonal interaction of clients. To allow clients to benefit from participating in a long-term group experience.
 To produce some groups cohesion among clients. To allow group leader to witness interpersonal interaction of clients. To allow clients to benefit from participating in a long-term group experience.")
62
RELAPSE PREVENTION GROUP Sample Topics
Alcohol -The Legal Drug Boredom Avoiding Relapse Drift/Mooring Lines Guilt and Shame Motivation for Recovery Truthfulness Work and Recovery Staying Busy Relapse Prevention Dealing with Feelings Total Abstinence Sex and Recovery Trust Be Smart; Not Strong Defining Spirituality Relapse Justification Reducing Stress Managing Anger Compulsive Behaviors Repairing Relationships

63
MATRIX MODEL FAMILY INVOLVEMENT
Family Education Family Support Groups Conjoint Sessions Encouraging Family to Get Assistance Encouraging Family to Support Sobriety

64
MATRIX MODEL SELF-HELP GROUPS
Source of Support and Camaraderie Source of Spiritual Strength Source of New Activities and Friends Lifelong Support System Multiple Forms of 12-Step Groups Alternative to 12-Step Groups

65
MATRIX MODEL URINALYSIS AND BREATH TESTING
Method for Monitoring Treatment Progress Treatment Accountability Assistance for Patient Reduce Arguments and Capriciousness Provides Data for Family or Employer

66
Web site matrixinstitute.org or ahndrea@matrixinstitute.org

Similar presentations