Download presentation
Presentation is loading. Please wait.

1
Assoc. Prof. Chatlert Pongchaiyakul, MD. Division of Endocrinology and Metabolism, Department of Medicine, Faculty of Medicine, KKU, THAILAND Role of ultrasound measurements in fracture risk assessment 2 nd Strong Bone Asia, 2008

2
Diagnosis Osteoporosis : WHO by DXA Treatment - Clinical risk factors - Fracture risk assessment tools

3
Definition of Osteoporosis Skeletal disorder characterized by compromised bone strength leading to an increased risk of fracture Bone strength primarily reflects the integration of bone density and bone quality NIH Consensus Conference, 2000

4
Digital X-ray radiogrammetry (DXR) Radiographic absorptiometry (RA) Single photon absorptiometry (SPA) Single energy X-ray absorptiometry (SXA) Dual photon absorptiometry (DPA) Dual energy X-ray absorptiometry / dual X- ray absorptiometry (DXA) Quantitative computed tomography (QCT) Quantitative ultrasound (QUS) BMD Assessment
 Radiographic absorptiometry (RA) Single photon absorptiometry (SPA) Single energy X-ray absorptiometry (SXA) Dual photon absorptiometry (DPA) Dual energy X-ray absorptiometry / dual X- ray absorptiometry (DXA) Quantitative computed tomography (QCT) Quantitative ultrasound (QUS) BMD Assessment")
5
Digital X-ray radiogrammetry (DXR) Radiographic absorptiometry (RA) Single photon absorptiometry (SPA) Single energy X-ray absorptiometry (SXA) Dual photon absorptiometry (DPA) Dual energy X-ray absorptiometry / dual X- ray absorptiometry (DXA) Quantitative computed tomography (QCT) Quantitative ultrasound (QUS) BMD Assessment
 Radiographic absorptiometry (RA) Single photon absorptiometry (SPA) Single energy X-ray absorptiometry (SXA) Dual photon absorptiometry (DPA) Dual energy X-ray absorptiometry / dual X- ray absorptiometry (DXA) Quantitative computed tomography (QCT) Quantitative ultrasound (QUS) BMD Assessment")
6
10-year probabilities by age and FNBMD T-score Kanis JA, et al. Osteoporos Int 2001;12:989-95.

7
Sites of BMD measure ment Wrist fracture Hip fractur e Vertebr al fracture All fractures Distal radius Femoral neck Lumbar spine 1.7 (1.4- 2.0) 1.4 (1.4- 1.6) 1.5 (1.3- 1.8) 1.8 (1.4- 2.2) 2.6 (2.0- 3.5) 1.6 (1.2- 2.2) 1.7 (1.4- 2.1) 1.8 (1.1- 2.7) 2.3 (1.9- 2.8) 1.4 (1.3- 1.6) 1.6 (1.4- 1.8) 1.5 (1.4- 1.7) Marshall D. BMJ 1996;312:1254-9. Cumming SR. JAMA 2002;288:1889-97 1 SD decrease: Fracture risk increase RR = 1.4-2.6

8
Advantage Gold standard Prediction fracture Monitoring Disadvantage Expensive & Maintenance High costs Limit resource Well-trained technician Not portable BMD by DXA

9
Fracture Rates, Population T-Score Distribution and Number of Fractures in NORA

10
Wainwright SA. J Clin Endocrinol Metab 2005;90(5):2787-93
:")
11
Quantitative Ultrasound Advantage Portable Less expensive and low costs Less time-consuming No radiation No need well-trained technician May predict fracture Disadvantage Not a gold standard Diagnostic performance (High specificity but low sensitivity)
")
12
Types of ultrasound transmission Trabecular transverse transmission: calcaneus (water-based and dry system) Cortical transverse transmission: phalanges Cortical axial transmission: phalanges, metacarpals, radius, tibia
 Cortical transverse transmission: phalanges Cortical axial transmission: phalanges, metacarpals, radius, tibia")
13
Speed of Sound (SOS) Broadband Ultrasound Attenuation (BUA) Stiffness Index (SI) = (0.67 x BUA)+(0.28 x SOS) - 420 Quantitative Ultrasound Index (QUI) = 0.41×(BUA + SOS) – 571 Amplitude dependent speed of sound (AD-SOS) Transmission of Signal Receipt of Signal t (time) w (width) SOS = w/t Quantitative Ultrasound Techniques
 Broadband Ultrasound Attenuation (BUA) Stiffness Index (SI) = (0.67 x BUA)+(0.28 x SOS) Quantitative Ultrasound Index (QUI) = 0.41×(BUA + SOS) – 571 Amplitude dependent speed of sound (AD-SOS) Transmission of Signal Receipt of Signal t (time) w (width) SOS = w/t Quantitative Ultrasound Techniques")
14
Speed of Sound (SOS) Broadband Ultrasound Attenuation (BUA) Stiffness Index (SI) = (0.67 x BUA)+(0.28 x SOS) - 420 Quantitative Ultrasound Index (QUI) = 0.41×(BUA + SOS) – 571 Amplitude dependent speed of sound (AD-SOS) Quantitative Ultrasound Techniques
 Broadband Ultrasound Attenuation (BUA) Stiffness Index (SI) = (0.67 x BUA)+(0.28 x SOS) Quantitative Ultrasound Index (QUI) = 0.41×(BUA + SOS) – 571 Amplitude dependent speed of sound (AD-SOS) Quantitative Ultrasound Techniques")
15
BQ Calcaneus 1 Vertebral body 2 BUASOSBUASOS BV/TV Tb.Th Tb.Sp Tb.N 0.78 0.82 -0.70 0.65 0.79 0.82 -0.75 0.67 0.72 0.52 -0.74 0.73 0.67 0.48 -0.66 0.66 Correlation between QUS parameters and trabecular structure in human cancellous bone QUS can assess bone quality and bone architecture. 1 Hans D. Bone 1995;16:295-300. 2 Nicholson PH. Bone 1998;23:425-31.

16
Correlations between QUS and DXA measurements Calaneus BMD LS BMD FN BMD total hip BMD QUS calcaneus (BUA, SOS, SI, QUI) 0.58-0.800.3-0.50.7-0.80.5-0.6 He YQ, et al. Osteoporos Int 2000;11:354-60. Greenspan SL, et al. Osteoporos Int 2001;12:391-8. Schneider J, et al. Calcif Tissue Int 2004;74:246-54. Gnudi S, et al.Ultrasound Med Biol 2004;30:357-61.

17
Can QUS be used to diagnose osteoporosis ? The WHO diagnostic classification cannot be applied to T-scores from measurements other than DXA at the femoral neck, total femur, lumbar spine or one-third (33%) radius because those T-scores are not equivalent to T-scores derived by DXA. (good, grade A, worldwide) ISCD 2007: Position Statement Krieg et al. The ISCD 2007 Official Positions. JCD2008;11:163-87
 radius because those T-scores are not equivalent to T-scores derived by DXA. (good, grade A, worldwide) ISCD 2007: Position Statement Krieg et al. The ISCD 2007 Official Positions. JCD2008;11:")
18
Estimate of the average T-score at the age of 65 in women Measurement SitesTechnique T-score at age 65 years Spine Heel Spine Forearm Femoral neck Total hip Heel QCT Lateral DXA Achilles DXA Sahara -2.5 -2.2 -1.5 -1.3 -1.4 -1.2 -0.9 -0.7 Kanis JA. Osteoporos Int 2001; 192-202.

19
Krieg et al. The ISCD 2007 Official Positions. JCD2008;11:163-87

20
Nakak S, Ann Intern Med. 2006;144:832-841. Sensitivity and Specificity for different QUS T-Scores

21
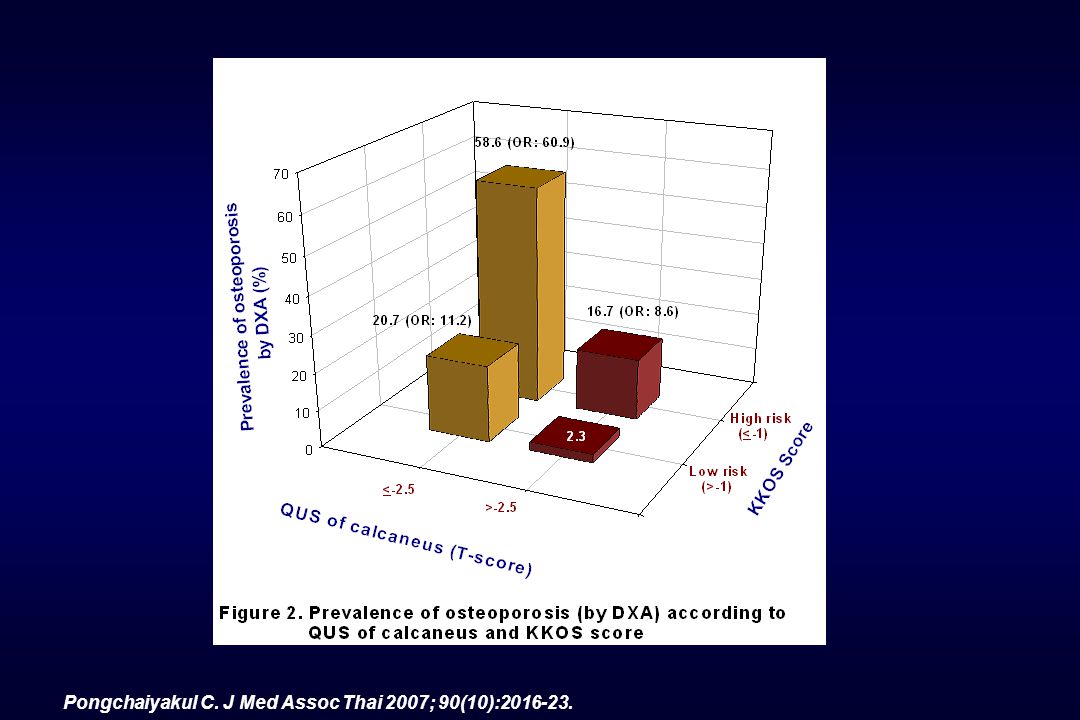
QUS and Osteoporosis prediction

22
Pongchaiyakul C. J Med Assoc Thai 2007; 90(10):2016-23.
:")
24
Female: 70 yr, 50 kg, QUS T-score = -3 SD 486778 ~0.5 48+67+78 =193 193 Pongchaiyakul C, et al. Osteoporos Int 2007;18:525-31.

26
Can QUS be used for fracture risk assessment? The only validated skeletal site for the clinical use of QUS in osteoporosis management is the “heel”. (good, grade A, Worldwide) Heel QUS predicted fragility fracture in postmenopausal women (hip, vertebral, and global fracture risk) and men >65 yr (hip and all non-verterbral fractures), independently of central DXA BMD. (good, grade A, Worldwide) Krieg et al. The ISCD 2007 Official Positions. JCD2008;11:163-87 ISCD 2007: Position Statement
 Heel QUS predicted fragility fracture in postmenopausal women (hip, vertebral, and global fracture risk) and men >65 yr (hip and all non-verterbral fractures), independently of central DXA BMD. (good, grade A, Worldwide) Krieg et al. The ISCD 2007 Official Positions. JCD2008;11: ISCD 2007: Position Statement.")
27
BUA SOS FN-BMD 1 2 3 4 0 Relative risk for hip fractures EPIDOS study BUA SOS FN-BMD 1 2 3 4 0 Relative risk for hip fractures SOF study BUA Cal-BMD FN-BMD 1.5 2.0 1.0 Relative risk for non-spinal fractures SOF study EPIDOS: Hans D. Lancet 1996;348:511-4. SOF: Bauer DC. Arch Int Med 1997;157:629-34.

28
Major cross-sectional studies of QUS in hip fracture prediction Krieg et al. JCD2008;11:163-87

29
Major cross-sectional studies of QUS in vertebral fracture prediction Krieg et al. JCD2008;11:163-87

30
Summary of prospective studies of QUS in osteoporotic fracture prediction Krieg et al. JCD2008;11:163-87

31
QUS and Fracture Prediction by Devices and by Types of Fractures

32
Krieg et al. JCD2008;11:163-87 QUS and Fracture Prediction by Devices and by Types of Fractures

33
Krieg et al. JCD2008;11:163-87

34
Site of fracture QUS parameter Site of measurement RR (95%CI) Any site Non-spinal Hip BUA SOS QUI BUA SOS QUI BUA SOS QUI Calcaneus All sites Calcaneus All sites Calcaneus 1.74 (1.38-2.21) 1.73 (1.38-2.17) 1.71 (1.28-2.29) 1.66 (1.39-1.99) - 1.23 (1.10-1.38) - 1.43 (1.22-1.67) 1.90 (1.47-2.45) 1.71 (1.21-2.42) 1.94 (1.46-2.59) Martin F. J Bone Miner Res 2006;21:1126–35. RR AND 95% CI OF LOW-ENERGY TRAUMA FRACTURES FOR 1 SD DECREASE IN THE QUS PARAMETERS IN WOMEN

35
Gradient of risk (RR/SD) for BUA and SOS in women with and without adjustment for BMD VariablesOutcome fracture Without BMDWith BMD RR/SD95%CIRR/SD95%CI BUA BUA BUA SOS Peripheral BMD Any Osteoporotic Hip Hip Any Osteoporotic Hip 1.40 1.72 1.51 1.30 1.35 1.30 1.25-1.58 1.26-1.56 1.52-1.95 1.33-1.71 1.22-1.39 1.25-1.45 1.15-1.48 1.22 1.20 1.40 1.24 1.06-1.41 1.06-1.36 1.22-1.61 1.09-1.40 Johnell O, Kanis JA. WHO. Geneva 2007. (www.who.int/chp/topics/rheumatic/en/index.html)

36
Case-finding strategy if DXA is not available Postmenopausal women CRFs + Heel QUS assessment Medium probability of fracture Low probability of fracture High probability of fracture Central DXA assessment according to WHO criteria Primary prevention Treatment initiation

37
Osteoporosis & Fracture: Burden in Asian population BMD by DXA: gold standard.. but have some limitations QUS: alternative method… - inexpensive, portable, radiation-free - proven to predict hip fractures and all osteoporotic fractures - different technologies - need specific guideline Conclusion

38
Strong Bone Asia

Similar presentations




 Translate into A Compression Fracture? S.L.>")
![2010 Guidelines Papaioannou A, et al. CMAJ 2010 Oct 12. [Epub ahead of print]. 2010 Clinical Practice Guidelines for the Diagnosis and Management of Osteoporosis.](/12/3477401/big_thumb.jpg "2010 Guidelines Papaioannou A, et al. CMAJ 2010 Oct 12. [Epub ahead of print]. 2010 Clinical Practice Guidelines for the Diagnosis and Management of Osteoporosis.>")

>")




 bone absorptiometry in clinical investigation CEPEM Centro de Estudos e Pesquisas da Mulher - Rio.>")




 This is the gold standard in Osteoporosis diagnosis. Reported as.>")


