Download presentation
Presentation is loading. Please wait.

1
Fundamentals Of Occlusion
Fahim Vohra SDS 333 Fundamentals Of Fixed Prosthodontics Chap 2, Pg

2
Outline Definitions Mandibular movement
Normal vs Pathological Occlusion Occlusal Interferences Schemes of Occlusion Determinants of Occlusion

3
The Temporo-Mandibular Joints

4
Why Is Occlusion Important ?
Assist in diagnosis Planning in restorative care To minimize failure Ensure predictable outcome by minimising loads on teeth Managing the environment so that we get the minimal amount of surprises (Similar to wearing a car seatbelt), the less the patient has to adapt the better.
, the less the. patient has to adapt the better.")
5
Definitions OCCLUSION
A relationship between the masticatory surfaces of the maxillary and mandibular teeth The relationship between tooth contacts and mandibular movements

6
Centric Occlusion Relationship of the mandible to the maxilla when the teeth are in maximum occlusal contact, irrespective of the position or alignment of the condyle-disk assemblies. The relationship between the maxilla and mandible when the teeth are maximally meshed with the mandible in its most cranial position

7
Centric Relation A relationship of the mandible to the skull where the condyle is in an anteriorly, superiorly braced position along the articular eminence of the glenoid fossa, with the articular disc interposed between the Condyle and eminence.

8
Mandibular Movements a) Horizontal axis
Mandibular movements occur around three axes a) Horizontal axis b) Vertical axis c) Sagittal axis
 Horizontal axis. b) Vertical axis. c) Sagittal axis.")
9
Horizontal Axis (Rotation)
This movement occurs in the sagittal plane when the mandible in centric relation makes a purely rotational opening and closing border movement around the transverse horizontal axis, which extends through both condyles.

10
Vertical axis (Rotation)
This movement occurs in the horizontal plane when the mandible moves into a lateral excursion. The center for this rotation is a vertical axis extending through the rotating or working-side condyle.

11
Balancing side (Non working side)
The side towards which the mandible moves during excursion OR Mandible moving toward the cheek Working side condyle pivots within the socket and is better supported. Balancing side (Non working side) The side opposite to the direction in which the mandible moves OR Mandible moving toward the tongue Balancing side condyle has a downward orbiting path and is more prone to injury or damage.
 The side opposite to the direction in which the mandible moves OR Mandible moving toward the tongue. Balancing side condyle has a downward orbiting path and is more prone to injury or damage.")
12
Condyle has downward path
Balancing Side Condyle has downward path Working Side Condyle pivots Movement direction Mandible and TMJ

13
Sagittal Axis This movement occurs when mandible moves to working side, the condyle on the opposite side (Non working side) travels forward and downwards simultaneously. When viewed in the frontal plane, this produces a downward arc on the non working side, rotating about an anteroposterior (sagittal) axis passing through the other condyle
 travels forward and downwards simultaneously. When viewed in the frontal plane, this produces a downward arc on the non working side, rotating about an anteroposterior (sagittal) axis passing through the other condyle.")
14
Pure Hinge Movement It occurs as the result of the condyles rotating in the lower compartments of the temporomandibular joints within a 10- to 13-degree arc, which creates a 20- to 25-mm separation of the anterior teeth

15
Translation Movement Occurs when the mandible moves forward (protrusion) Teeth, condyles, and rami, all move in the same direction and to the same degree. Occurs within the superior cavity of the joint

16
Maximum Opening (Translation & Rotation)
Occurs in the upper compartment of the joint as the mandible drops down farther . Then the horizontal axis of rotation shifts to the area of the mandibular foramen, as the condyles translate forward and downward while continuing to rotate.

17
Protrusive Position When the mandible slides forward so that the maxillary and mandibular anterior teeth are in an end-to-end relationship, it is in a protrusive position.

18
Bennett Movement It is defined as “the bodily lateral movement/ lateral shift of mandible resulting from movements of condyles along lateral inclines of mandibular fossa during lateral jaw movement” Dr Norman Bennett

19
Bennett Angle The angle formed between the sagittal plane and the average path of advancing condyle as viewed in the horizontal plane during lateral mandibular movements. Average range is degree BSC WSC Bennett angle Sagittal plane

20
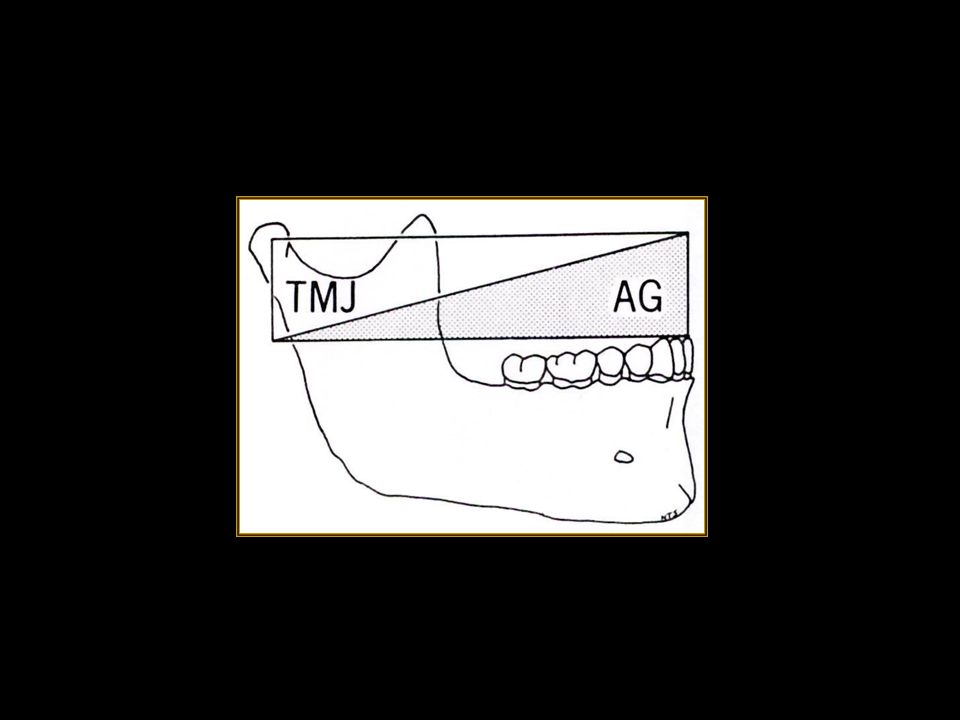
Posterior Determinant of Occlusion
TMJ – Temporomandibular Joint Bony surfaces The dentist has no control on the posterior determinants i.e. TMJ

21
Anterior Determinant of Occlusion
Teeth Incisors Canines Premolars Molars

22
Anterior Determinants Of Occlusion
Posterior teeth Provide vertical stops Guide mandible to CO Anterior teeth Guide mandible in protrusive, retrusive and lateral excursions The closer the tooth located to a determinant , more it will be influenced by it.

24
Occlusal Interferences
Interferences are undesirable occlusal contacts that may produce mandibular deviation during closure to maximum intercuspation or may hinder smooth passage to and from the intercuspal position . These can be of following types Centric Working Non working Protrusive

25
Centric Interferences
It is a premature contact that occurs when the mandible closes with the condyles in their optimum position in the glenoid fossae (CR) . It will cause deflection of the mandible in a posterior, anterior, and/or lateral direction
 . It will cause deflection of the mandible in a posterior, anterior, and/or lateral direction.")
26
Working Side Interference
It occurs when there is contact between the maxillary and mandibular posterior teeth on the same side of the arches as the direction in which the mandible has moved. If that contact is heavy enough to dis-occlude anterior teeth, it is an interference .

27
Non-Working Side Interference
It is an occlusal contact between maxillary and mandibular teeth on the side of the arches opposite the direction in which the mandible has moved in a lateral excursion . It has the potential for damaging the teeth, PDL, MOM and TMJ due to changes in the mandibular leverage, the placement of forces outside the long axes of teeth and disruption of normal muscle function.

28
Protrusive Interference
It is a premature contact occurring between the mesial aspects of mandibular posterior teeth and the distal aspects of maxillary posterior teeth . The proximity of the teeth to the muscles and the oblique forces make them potentially destructive. They also interfere with the patient's ability to incise properly

29
Ideal vs Pathologic Occlusion

30
Ideal Occlusion An ideal occlusion should provide comfort and function in a predictable way. 1) Ideal occlusion at tooth level Cusp tip to fossa or cusp to marginal ridge contact – i.e no incline contacts 2) Ideal occlusion at articulatory system level Posterior stability, Anterior guidance, Lack of posterior interferences. 3) Ideal occlusion at patient level Within the adaptability of the rest of the articulatory system.
 Ideal occlusion at articulatory system level. Posterior stability, Anterior guidance, Lack of posterior interferences. 3) Ideal occlusion at patient level. Within the adaptability of the rest of the articulatory system.")
31
Features Of Ideal Occlusion
Anterior Guidance: In lateral excursions of the mandible, working-side contacts (preferably on the canines) disocclude or separate the nonworking teeth instantly. In protrusive excursions, anterior tooth contacts will disocclude the posterior teeth.
 disocclude or separate the nonworking teeth instantly. In protrusive excursions, anterior tooth contacts will disocclude the posterior teeth.")
32
Protrusive Guidance Excursive Guidance

33
Features Of Ideal Occlusion
B) Posterior stability: Enough posterior teeth in each arch with solid and stable contacts in appropriate positions to evenly distribute loads and to allow the mandible to close in a reproducible CO. Posterior teeth contact more heavily than anterior teeth It is enhanced by tall cusp – deep fossa Maintains teeth position CO or ICP is easily reproduced Increased masticatory function Signs of lack of PS, drifting, fremitus, fractured rest, mobility & wear
 Posterior stability: Enough posterior teeth in each arch with solid and stable. contacts in appropriate positions to evenly distribute loads and. to allow the mandible to close in a reproducible CO. Posterior. teeth contact more heavily than anterior teeth. It is enhanced by tall cusp – deep fossa. Maintains teeth position. CO or ICP is easily reproduced. Increased masticatory function. Signs of lack of PS, drifting, fremitus, fractured rest, mobility & wear.")
34
Lack Of Posterior Stability

35
Features Of Ideal Occlusion
C) Absence of posterior interferences The non-working side
 Absence of posterior interferences. The non-working side.")
36
Features Of Ideal Occlusion
D) Centric Occlusion is achieved at centric relation position E) Occlusal loads are axially transmitted through the teeth
 Centric Occlusion is achieved at centric. relation position. E) Occlusal loads are axially transmitted through. the teeth.")
37
Organization Of Occlusion
There are three recognized concepts that describe how teeth should contact in various mandibular positions Bilateral balanced occlusion Unilateral Balanced occlusion (Group function) 3. Mutually protected occlusion (Canine protected)
 3. Mutually protected occlusion. (Canine protected)")
38
Bilateral Balanced Occlusion
It dictates that a maximum number of teeth should contact in all excursive positions of the mandible. Use for complete denture occlusal scheme as contacts on non-working side prevent tipping of the denture Not used for fixed prosthodontics, as very difficult to achieve

39
Unilateral Balanced Occlusion
Also called group function It requires teeth on the working side to be in contact in lateral excursion and teeth on the non-working side are free of any contact. Avoids destructive , oblique forces on the non-working side. Prevents wear of maxillary palatal and mandibular buccal cusps

40
Mutually Protected Occlusion
Also called canine protected occlusion Anterior teeth overlap prevents the posterior teeth from making any contact on either the working or the nonworking sides during mandibular excursions. Anterior teeth bear all the load and the posterior teeth are dis-occluded during excursions. Protecting the posterior teeth In CO, posterior teeth direct forces through their long axis and anterior teeth are slightly in or out of contact. Protecting the anterior teeth.

41
Guidance Describes the influenced path the mandible
takes as a result of the contacting surfaces of the teeth. Depending on the contact and shape of the teeth they should be in harmony

42
Protrusive Guidance Influenced path the mandible takes as a
result of a forward thrust

43
Lateral Guidance Canine
Describes the way in which lateral excursions are affected by tooth to tooth contacts involving the canine teeth only resulting in disclusion of the posterior teeth

44
Lateral Guidance Group function
When lateral excursions are guided by more than one tooth other than the canines

45
Hanau’s Quint By modifying the following five factors, a scheme of occlusion can be developed that will suit a particular patient best. 1. Condylar guidance 2. Incisal guidance 3. Occlusal plane orientation 4. Compensating curves 5. Height of the Cusp Except for the condylar guidance, all other factors can be modified during the fabrication of a prosthesis and the anterior guidance plays a predominant role.

46
Anterior Guidance Guidance produced by the teeth themselves and not the temporomandibular joint (can be on any tooth) The influence of contacting surfaces of anterior teeth on mandibular movements. The influence of contacting surfaces of the guide pin and anterior guide table on articulator movements. The fabrication of a relationship of the anterior teeth preventing the posterior tooth contact in all eccentric mandibular movements.

47
Effects Of Anatomic Determinants Of Occlusion

48
Protrusive Incisal Path
The track of the incisal edges of the mandibular teeth from maximum intercuspation to edge-to-edge occlusion.

49
Protrusive Incisal Path Angle
The angle formed by the protrusive incisal path and the horizontal reference plane is the protrusive incisal path inclination. It ranges from 50 – 70 degrees and is often 5-10º steeper than the sagittal condylar guidance.

50
Incisal Guide Angle The angle formed with the horizontal plane of occlusion and a line in the sagittal plane between the incisal edges of maxillary & mandibular central incisors when the teeth are in maximum intercuspation. The angle formed in the sagittal plane between the horizontal plane and the slope of the incisal guide table.

51
Importance of Anterior Guidance
Opening and closing of the mandible is simply a rotation of the condyles in the articular fossae.

52
Importance of Anterior Guidance
As anterior guidance is normally steeper than the condylar guidance, the anterior teeth guide the mandible downwards during protrusive or lateral movement and ..

53
Importance of Anterior Guidance
(during protrusive movement) .. produces dis-occlusion or separation of the posterior teeth.
 .. produces dis-occlusion or separation of the posterior teeth.")
54
Importance of Anterior Guidance (during lateral movement)
C.G.O Group Function W.S N.W.S

55
Importance of Anterior Guidance
Anterior guidance is linked to the combination of horizontal & vertical overlap of the anterior teeth and can affect the occlusal surface morphology of the posterior teeth.

56
Inter-relationship with Vertical & Horizontal Overlap of the Anterior teeth
Anterior guidance can be made steeper by either increasing the vertical overlap (overbite) ‘A-B’, or by reducing the horizontal overlap (over jet) ‘C-A’ of the anterior teeth. Anterior guidance can be made shallow by either decreasing the overbite ‘B-A’ or increasing the over jet ‘A-C’ of the ant. teeth.
 ‘A-B’, or by reducing the horizontal overlap (over jet) ‘C-A’ of the anterior teeth. Anterior guidance can be made shallow by either decreasing the overbite ‘B-A’ or increasing the over jet ‘A-C’ of the ant. teeth.")
57
Condylar Guidance & Posterior tooth Morphology (without considering the role of A.G.)
Shallow condylar guidance normally requires shallow cusp angle or short cusp height and steeper condylar guidance requires steep cusp angle or longer cusp height.

58
‘side shift +’ ‘No side shift’
Condylar side-shift & Posterior tooth Morphology (without considering the role of A.G.) ‘side shift +’ ‘No side shift’ Similarly, in the presence of an immediate lateral side shift during lateral movement (Bennett’s movement) the cusp height and cusp angle should be shallow.
 ‘side shift +’ ‘No side shift’ Similarly, in the presence of an immediate lateral side shift during lateral movement (Bennett’s movement) the cusp height and cusp angle should be shallow.")
59
Influence of Anterior Guidance on Posterior tooth Morphology

60
Influence A.G. on Posterior tooth Morphology (Effect of Overbite)
Greater overbite produces more disocclusion hence permits longer cusp height Less overbite – less disocclusion – shorter Cusp height.

61
Influence of A.G. on Posterior tooth Morphology (Effect of Over jet)
Greater over jet necessitates shorter cusp height. Less over jet allows for long cusp height.

62
Influence of A.G. on Posterior tooth Morphology
Summarizing, greater anterior guidance allows posterior teeth to have longer cusp height & smaller anterior guidance requires posterior teeth to have shorter cusp height.

63
Influence of A.G. on Posterior tooth Morphology
By increasing the anterior guidance angle to compensate for inadequate or shallow condylar guidance, it is possible to increase the cusp height of the posterior teeth.

64
Influence of A.G. on Posterior tooth Morphology
Similarly, increasing the anterior guidance will permit lengthening of the cusp that otherwise have to be shorter in the presence of pronounced immediate lateral translation of the condyles.

65
THANK YOU

Similar presentations