Download presentation
Presentation is loading. Please wait.

1
Disease Mapping: A Renewed Opportunity for Epidemiologic Investigation Dan Wartenberg UMDNJ-RW Johnson Medical School, Piscataway, NJ and the Cancer Institute of New Jersey Research supported by: R01 CA92693-02 from the National Cancer Institute U61/ATU272387 from ATSDR (CDC) New Jersey Legislature dan.wartenberg@umdnj.edu
 New Jersey Legislature")
2
Epidemiology and Disease Mapping Disease and Exposure Mapping Descriptive studies: Issues of scale, accuracy, missing data, interpretation Cluster Detection and Disease Surveillance Assessment and Availability of Health Services: Screening, access to care Exposure Assessment: Traffic density and Pesticide Studies Data Linkage Geographical Correlation Studies and Hypothesis Generation The Assessment of Risk from a Point or Local Source Lead poisoning: Linking risk factors, case identification and intervention Data Integration Habitat Suitability for Disease Vectors—Lyme disease, West Nile,… Infection and Cancer: ‘Population Mixing’ and the role of hygiene/SES Novel Epidemiologic Study Designs: Population identification and recruitment Rare Exposures AND Outcomes: Magnetic fields and Childhood leukemia

3
Why has disease mapping growing so rapidly? Development of GIS Geographically indexed relational database Computer program to map and analyze spatial data Increasing availability of georeferenced data Ability to geocode, use GPS Demographics, disease outcomes, environmental quality, health services

4
Disease Mapping

5
The history of disease mapping Several excellent reviews, e.g., Cliff and Haggett (1988) Howe (1989) Walter and Birnie (1991) Lawson et al. (1999) Walter (2000) Bithell (2000)
 Walter (2000) Bithell (2000).")
6
Evolution of Data Displays Univariate mapping Cases (dot or spot maps) Area counts—aggregate to numerators Rates (choropleth maps)—added denominator Adjusted rates—accommodate confounding Smoothed rates—easier interpretation 3-Dimensional plots—alternative displays Multivariate maps Bivariate displays Maps of multivariate analyses (e.g., PCA)
 Area counts—aggregate to numerators Rates (choropleth maps)—added denominator Adjusted rates—accommodate confounding Smoothed rates—easier interpretation 3-Dimensional plots—alternative displays Multivariate maps Bivariate displays Maps of multivariate analyses (e.g., PCA)")
7
Cholera in London, 1849 Dot Map+Marginal Histograms From Cliff and Haggett 1988

8
Thematic and Rate Maps From Cliff and Haggett 1988

9
Three-Dimensional View From Cliff and Haggett 1988

10
Space-Time Maps From Cliff and Haggett 1988

11
Cartograms

12
Effect of Age Adjustment From Monmonier 1997

13
Displaying Multiple Variables

14
Aggregation Bias

15
Rate Instability Rate estimates for areas with small populations often are unstable Previous approaches Smoothing (e.g., empirical Bayes) Can miss important peaks Aggregation of geographic units Need consistent rule to identify grouping criteria Need replicable algorithm for aggregation process Current research is evaluating alternatives
 Can miss important peaks Aggregation of geographic units Need consistent rule to identify grouping criteria Need replicable algorithm for aggregation process Current research is evaluating alternatives")
16
Interactive Mapping Female Childhood Leukemia 1970-1994 (ages 0-19) From Biomedware 2003
 From Biomedware 2003")
17
Disease Clusters

18
Two Cluster Dot Maps Woburn, Ma Toms River, NJ

19
Why study clusters? Public concern Clarify of misconceptions Allay concerns that are unfounded Initiate study when concerns are well founded Encourage Remediation and Prevention Determine if situation is a sentinel of a larger problem Identify unknown exposure situations Facilitate Scientific Discovery Identify new exposure-disease link Identify new carcinogens

20
New Opportunities Rapid response to resident concerns (e.g., SAHSU) Online, real-time display of cancer data, known point sources, other environmental data Space-time pattern of cancer incidence at small scale How many ‘clusters’ are there? Where are the lows as well as the highs, and why? Prioritize potential investigations What warrants follow up? Implementation of prospective surveillance Active vs. Passive approach

21
Exposure Assessment/Estimation

22
An Epidemiologist’s Perspective on Exposure Assessment A tool rather than an end in and of itself User rather than developer Specific uses Conduct otherwise undoable epidemiology Improve scope, focus or interpretability

23
Point and Nonpoint Source Pollution Point source pollution Toxics, birth defects and low birth weight (Geschwind et al. 1992; Stallones et al. 1992; Berry and Bove 1997; Croen et al. 1997) Incinerators and cancer (Gatrell and Dunn 1995) Nonpoint source pollution Drinking Water (Nuckols et al. 1995) Pesticides (Nuckols et al. ) Traffic derived air pollution (English et al. 1999; Ritz et al. (2000, 2002, 2003; Brauer et al. 2003)
 Incinerators and cancer (Gatrell and Dunn 1995) Nonpoint source pollution Drinking Water (Nuckols et al. 1995) Pesticides (Nuckols et al. ) Traffic derived air pollution (English et al. 1999; Ritz et al. (2000, 2002, 2003; Brauer et al. 2003).")
24
Air Pollution from Traffic From Wilhelm and Ritz 2003

25
Data Linkage

26
Map-Based Correlational Studies Various historical efforts New impetus triggered by NCI Atlas (1970s) Compared mortality maps to possible exposures Then validated with traditional epidemiology Bladder cancer and chemical manufacturing Nasal adenocarcinoma and furniture manufacturing Lung cancer and shipyards Oral cancers among women and snuff use Approach reinvigorated in past few years New tools and geocoded databases Despite the ‘Bad Press’ these can be useful Must be careful of limitations of ‘ecologic analysis’
 Compared mortality maps to possible exposures Then validated with traditional epidemiology Bladder cancer and chemical manufacturing Nasal adenocarcinoma and furniture manufacturing Lung cancer and shipyards Oral cancers among women and snuff use Approach reinvigorated in past few years New tools and geocoded databases Despite the ‘Bad Press’ these can be useful Must be careful of limitations of ‘ecologic analysis’")
27
Preventing Childhood Lead Poisoning Screening data readily available Using the GIS screening assessing the impact of targeted screening evaluating predictive equations Are SES, housing age, other factors predictive surveillance combining maps of exposure and disease target educational and remediation programs

28
Preliminary Lead Study Proposed strategy for targeted screening use demographics and local hazards to predict lead poisoning rates map cases validate by comparing cases to predictions and then adjust prediction equation Developed hypothetical model and data Implement appropriate screening/intervention (Wartenberg 1992)
")
29
Childhood Lead Exposure: Advantages of Using a GIS Can expand to nationwide demographic evaluation Can explore prediction models using individual data Can look for other risk factors Can adjust for bias due to spatial autocorrelation Can design/evaluate screening and interventions

30
Population Mapping

31
Magnetic Fields and Childhood Leukemia Do magnetic fields cause cancer? Blue Ribbon panels--possible Combined Analyses of Studies Show Small but consistent elevations of risk A moderate exposure-response gradient Few subjects and “high” exposures

32
Rare Exposure, Rare Disease Proximity to high voltage transmission lines Background exposure ~1 mG Exposure over 10 mG are very rare Most studies have low exposure (0-5 mG) Homes close to high voltage lines can be 50 mG Childhood leukemia rare (1 in 30,000 per year) Proximity to high voltage lines rare (<2%) Following Feychting and Ahlbom (1993), design nested case control study in US, we don’t have the luxury of a population registry
 Homes close to high voltage lines can be 50 mG Childhood leukemia rare (1 in 30,000 per year) Proximity to high voltage lines rare (<2%) Following Feychting and Ahlbom (1993), design nested case control study in US, we don’t have the luxury of a population registry")
33
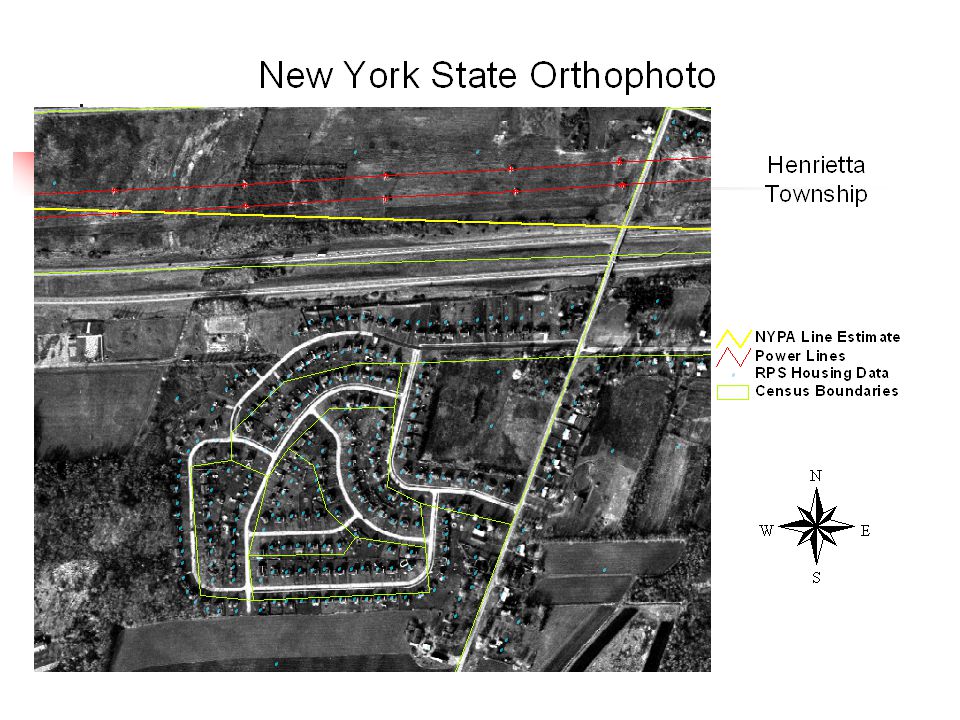
NYS Power Lines Mapping Study Geolocated all 345 + kV power lines Overlaid on Residential Data digital orthophotographs US Census data NYS RPS data Goals Estimate population exposures near lines Assess risk among most highly exposed

34
High Voltage Electric Power Transmission Lines in NY

35
Exposure Buffer Areas From Monmonier 1991

37
Case Location Problems Map NYS childhood leukemia cases 1976-1994 2.3% of population inside buffer Reasons for Uncoded Missing address Not in Tiger Files No house number Rural Delivery only P.O Box

38
Preliminary Results Age Relative Risk (95% CI) [n] Group 0-1000 ft 0-2000 ft 0-4 0.52 (0.17, 1.62)[3] 0.46 (0.19, 1.10)[5] 0-14 0.36 (0.13, 0.96)[4] 0.51 (0.28, 0.93)[7] 0-19 0.38 (0.16, 0.91)[5] 0.47 (0.27, 0.83)[7] Conclusions Method works well Substantive results inconclusive (too small n) Need to conduct study in more densely populated state
![Preliminary Results Age Relative Risk (95% CI) [n] Group ft ft (0.17, 1.62)[3] 0.46 (0.19, 1.10)[5] (0.13, 0.96)[4] 0.51 (0.28, 0.93)[7] (0.16, 0.91)[5] 0.47 (0.27, 0.83)[7] Conclusions Method works well Substantive results inconclusive (too small n) Need to conduct study in more densely populated state](http://images.slideplayer.com/13/4147546/slides/slide_38.jpg "Preliminary Results Age Relative Risk (95% CI) [n] Group ft ft (0.17, 1.62)[3] 0.46 (0.19, 1.10)[5] (0.13, 0.96)[4] 0.51 (0.28, 0.93)[7] (0.16, 0.91)[5] 0.47 (0.27, 0.83)[7] Conclusions Method works well Substantive results inconclusive (too small n) Need to conduct study in more densely populated state")
39
Data Integration

40
Introduction to Lyme Disease Natural History Bacterium Borrelia bugdorferi transmitted by ticks of genus Ixodes Small mammals are reservoir Prime habitat is damp wooded areas Barbour et al. 2001 Used Fire Model as proxy for I. scapularis vegetation type, density, and ground moisture influence off-host survival, deer host presence Used seroprevalence in dogs as surrogate for human risk Combined to predict overall human risk

41
Lyme Disease Risk Lyme Disease Risk based on co-Kriging Habitat Suitability and Seroprevalence Data in Dogs

42
Lyme Disease in NE US Estimated Tick Establishment

43
Childhood Leukemia and Clusters Observed cluster of childhood cancer in Seascale, UK near nuclear power station Few causes known of childhood leukemia Government concerned (much publicity) Commissioned series of studies Results suggest only risk was paternal exposure Seemed contrary to radiation risk Others sought alternative explanation
 Commissioned series of studies Results suggest only risk was paternal exposure Seemed contrary to radiation risk Others sought alternative explanation")
44
Hypotheses Kinlen—Population Mixing Children from isolated populations, with decreased exposure to infections, when exposed to others from regions of greater population density are at increased risk of leukemia, likely due to viral etiology Greaves—SES and Hygiene Delay of exposure to infections from infancy to each childhood, such as due to improvements in socioeconomic status and hygiene, puts children at increased risk of leukemia and lymphomas.

45
Evaluations of Hypotheses Several studies in UK, generally supportive Few in other countries, mixed This study: Analysis of SEER Data Use data from states with rural counties Test hypothesis for rates of ALL Compare rates by Size of population change Size of income Compare to pattern of CNS cancers as reference (to control for methodology)
")
46
Results for IA, NM, UT Percentage Change in Population Size >0%-10%>10%-20%>20% Base Case ALL 1.7 (0.8-3.5)2.1 (1.2-3.9)2.5 (1.4-4.5) CNS 1.1 (0.5-2.4)1.3 (0.7-2.4)0.6 (0.3-1.6) Birth Location=Any State ALL1.6 (1.0-2.5)1.3 (0.8-2.0)1.4 (0.9-2.3) CNS1.3 (0.7-2.3)1.2 (0.7-2.1)0.9 (0.5-1.7) Income $22,001-$25,500$25,501-$27,500>$27,500 ALL1.3 (0.8-2.1)0.8 (0.5-1.3)0.9 (0.6-1.3) CNS0.9 (0.5-1.9)1.1 (0.6-2.0)1.3 (0.8-2.3) (with D. Schneider and S. Brown)
.")
47
The Future

48
Epidemiologic Prospects—1 Improved descriptive studies Improved cluster identification and response Rapid response, not limited by geopolitical boundaries correlate with possible environmental exposures prospective surveillance Improved exposure assessment Use of geographic models and indices proximity/dispersion from point/non-point sources (e.g., dump sites, stacks) (e.g., wind, groundwater models) adjustments for spatial autocorrelation (e.g., time, space series)
 (e.g., wind, groundwater models) adjustments for spatial autocorrelation (e.g., time, space series)")
49
Epidemiologic Prospects—2 New Data Linkages and Hypotheses Correlation analyses Improved Data Integration Habitat identification for risk prediction Lyme disease, cholera, West Nile disease Complex analyses (multivariate assessment) New investigation strategies Population identification and recruitment (controls?) Nested case control studies Hypothesis generation
 New investigation strategies Population identification and recruitment (controls ) Nested case control studies Hypothesis generation")
50
Epidemiologic Prospects—3 Environmental Justice Investigations transcend geopolitical boundaries conduct multi-site studies for similar communities Improved public communication maps communicate more clearly than numbers or words this is a double edged sword

Similar presentations







 Betty C. Jung, RN, MPH, CHES.>")











