Download presentation
Presentation is loading. Please wait.

1
Affective Disorders

2
Overview What is a affective disorder?
Criteria for specific mood episodes and disorders Pharmacological intervention

3
Introduction The term affective is related to feelings, mood or emotion. Hippocrates first coined the term “melancholia” meaning “unshakable sadness”. Today known as depression So, affective disorder is a group of disorder that are related to mood and mainly include depression, mania and anxiety.

4
What is affective disorder?
Mood is a person’s subjective emotional state Affect is the objective appearance of mood Mood disorders involve a depression or elevation of mood as the primary disturbance Can have other abnormalities such as anxiety.

5
Characterization Affective disorder is mainly characterized by:
Depression Anxiety Mania

6
1. Major depression (Unipolar Depression)
2. Manic depressive illness (Bipolar Depression)
")
7
1. Major Depressive Episode
Depressed mood Anhedonia Decrease or increase in appetite OR significant weight loss or gain Persistently increased or decreased sleep Psychomotor agitation or retardation Fatigue or low energy Feelings of worthlessness or inappropriate guilt Decreased concentration or indecisiveness Recurrent thoughts of death, suicidal ideation, or suicide attempt Five or more symptoms present for ≥ 2 weeks

8
2. Manic depressive illness
(Bipolar Depression) Psychosis is a symptom of mental illnesses characterized by a distorted or non-existent sense of reality. Psychotic disorders have different etiologies, each of which demands a unique treatment approach. Common psychotic disorders include major depression or mania with psychotic features, substance-induced psychosis, dementia with psychotic features, brief psychotic disorder, delusional disorder, schizophrenia.
 Psychosis is a symptom of mental illnesses characterized by a distorted or non-existent sense of reality. Psychotic disorders have different etiologies, each of which demands a unique treatment approach. Common psychotic disorders include major depression or mania with psychotic features, substance-induced psychosis, dementia with psychotic features, brief psychotic disorder, delusional disorder, schizophrenia.")
9
Symptoms of Anxiety Anxiety disorders encompass a constellation of symptoms, and include generalized anxiety disorder, obsessive-compulsive disorder, panic disorder, post-traumatic stress disorder, separation anxiety disorder, social phobia, specific phobias, and acute stress. Symptoms of anxiety also are often associated with depression and other medical conditions. Anxiety is common in MDD and bipolar disorder; however, may be a separate diagnosis.

10
Major Depressive Disorder
Presence of a major depressive episode Episode not better explained by another diagnosis NO HISTORY of mania, hypomania, or mixed episode.

11
Major Depressive Disorder
Lifetime risk: 10%-25% for women 5%-12% for men Family history of MDD increases risk times Up to 20%-25% of patients with major medical comorbidity (CVD, diabetes, cancer) will develop MDD Average age of onset in mid-20’s
 will develop MDD. Average age of onset in mid-20’s.")
12
Major Depressive Disorder: Treatment basics
Medications: Selective serotonin reuptake inhibitors (SSRIs) Tricyclic antidepressants (TCAs) Monoamine oxidase inhibitors (MAOIs) Other: venlafaxine, mirtazapine, nefazodone, bupropion Psychotherapy: Cognitive-behavioral therapy (CBT) Interpersonal therapy (IPT) Psychodynamic psychotherapy (e.g., psychoanalysis) Other Electroconvulsive therapy (ECT) Light therapy – primarily for SAD
 Tricyclic antidepressants (TCAs) Monoamine oxidase inhibitors (MAOIs) Other: venlafaxine, mirtazapine, nefazodone, bupropion. Psychotherapy: Cognitive-behavioral therapy (CBT) Interpersonal therapy (IPT) Psychodynamic psychotherapy (e.g., psychoanalysis) Other. Electroconvulsive therapy (ECT) Light therapy – primarily for SAD.")
13
Major Depressive Disorder: Medications
Treatment choice based on: Severity Side effect profile Risk of overdose Other diagnoses (e.g., anxiety) ?Family history of treatment response If psychosis is present, this must be treated Medications may take up to 6 (8? 12?) weeks to be maximally effective Efficacy 60%-80% overall (50%-60% for each)
 Family history of treatment response. If psychosis is present, this must be treated. Medications may take up to 6 (8 12 ) weeks to be maximally effective. Efficacy 60%-80% overall (50%-60% for each)")
14
Bipolar I Disorder At least one manic or mixed episode
No need for a prior depressive episode

15
General Comments Symptoms cause significant impairment in social and/or occupational functioning. Symptoms do not result from a drug of abuse, medication, other treatment, or general medical condition

16
Manic Episode Elevated (or irritable) mood for >1 week
Three or more of following (four if mood irritable): Grandiosity Decreased need for sleep Flight of ideas, racing thoughts Distractibility Increased goal-directed activity Excessive involvement in pleasurable activities with high risk
: Grandiosity. Decreased need for sleep. Flight of ideas, racing thoughts. Distractibility. Increased goal-directed activity. Excessive involvement in pleasurable activities with high risk.")
17
Causes Norepinephrine and serotonin cause functional deficit at specific nerve cell synapses that is associated with depression On the other hand, excess of these neurotransmitters leading to mania.

18
Biogenic Theory of Depression
The precise cause of affective disorders remains elusive. Evidence implicates alterations in the firing patterns of a subset of biogenic amines in the CNS, Norepinephrine (NE) and Serotonin (5-HT). Activity of NE and 5 -HT systems.
 and Serotonin (5-HT). Activity of NE and 5 -HT systems.")
19
Amine neurotransmitters are either degraded (metab)
or reuptaken MAO Mito COMT

20
The purpose of antidepressants is the increase the [neurotransmitters] in the synapse
![The purpose of antidepressants is the increase the [neurotransmitters] in the synapse](http://slideplayer.com/slide/4142279/13/images/20/The+purpose+of+antidepressants+is+the+increase+the+%5Bneurotransmitters%5D+in+the+synapse.jpg "The purpose of antidepressants is the increase the [neurotransmitters] in the synapse")
21
Depression and Mania Monoamine Theory of Mental Depression
Depression is linked to low levels of norepinephrine and/or serotonin. Mania is linked to high levels of norepinephrine and/or serotonin. Bipolar mood disorder is alternating cycles of depression and mania. Learning Outcomes 14.1 Identify the different types of depression and the importance of neurotransmitter function in the cause and treatment of depression. In some cases of depression, there are alternate periods of hyperexcitability and elation known as mania. Individuals who experience these alternating cycles of depression and mania are classified as manic depressive. Another term for this condition is bipolar mood disorder. Low levels of norepinephrine and/or serotonin are associated with mental depression, while high levels of norepinephrine and/or serotonin may be involved in mania. This concept involving norepinephrine and serotonin is known as the Monoamine Theory of Mental Depression.

22
Drugs Used to Treat Depression
Drugs that increase the level of norepinephrine and serotonin are used in the treatment of depression. Major antidepressant drug classes: Serotonin reuptake inhibitors (SSRIs) Atypical SSRIs Tricyclic antidepressants (TCAs) Monoamine oxidase inhibitors (MAOIs) Learning Outcomes 14.1 Identify the different types of depression and the importance of neurotransmitter function in the cause and treatment of depression. Drugs that can increase the level of norepinephrine or serotonin in the brain are useful in the treatment of mental depression. They are referred to as antidepressants, or mood elevators. The major antidepressant drug classes include the selective serotonin reuptake inhibitors (SSRIs), atypical SSRIs, tricyclic antidepressants (TCAs), and monoamine oxidase inhibitors (MAOIs).
 Atypical SSRIs. Tricyclic antidepressants (TCAs) Monoamine oxidase inhibitors (MAOIs) Learning Outcomes Identify the different types of depression and the importance of neurotransmitter function in the cause and treatment of depression. Drugs that can increase the level of norepinephrine or serotonin in the brain are useful in the treatment of mental depression. They are referred to as antidepressants, or mood elevators. The major antidepressant drug classes include the selective serotonin reuptake inhibitors (SSRIs), atypical SSRIs, tricyclic antidepressants (TCAs), and monoamine oxidase inhibitors (MAOIs).")
23
TREATMENT FOR DEPRESSION
Psychotherapy Electroconvulsive therapy Natural alternatives Medication SSRIs MAOIs TCAs SNRIs NDRIs TeCAs Psycotherapy/talk therapy – especially useful when combined with meds. Goal is to teach good coping skills for every day stressors ECT – electric shock is applied to scalp through electrodes, results in seizure in the brain. Fast and effecitve in patients with depression or suicidal thoughts (good for suicide bc doesn’t have the same delayed onset as meds). Usually given up to three times a week for two to four weeks Natural alternatives – St. John’s wort (sold in teas and tablets, and in diet pills) not good for severe depression but can help mild depression
. Usually given up to three times a week for two to four weeks. Natural alternatives – St. John’s wort (sold in teas and tablets, and in diet pills) not good for severe depression but can help mild depression.")
24
NEUROTRANSMITTERS AND THE CATECHOLAMINE HYPOTHESIS
Neurotransmitters pass along signal Smaller amount of neurotransmitters causes depression SYNAPSE: Neurotransmitter passes along synapse from inside storage vesicles through transporters in the presynaptic cell to receptors in the post synaptic cell. Monoamine hypohtesis suggests that small amount of neurotransmitter causes depression

25
MONOAMINE OXIDASE (MAO) AND DEPRESSION
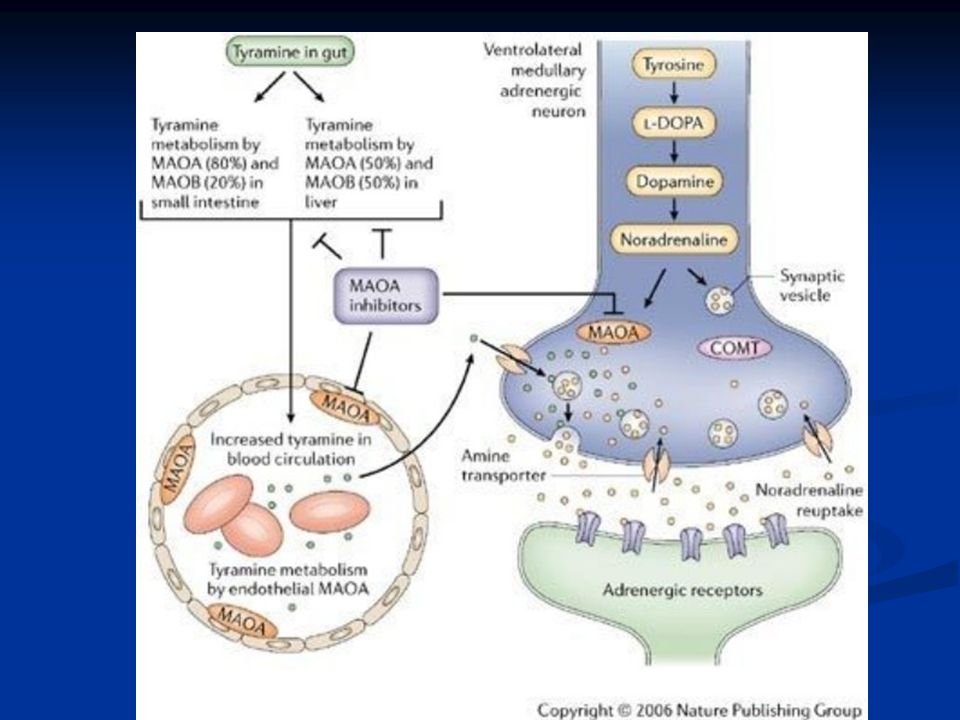
MAO catalyze deamination of intracellular monoamines MAO-A oxidizes epinephrine, norepinephrine, serotonin MAO-B oxidizes phenylethylamine Both oxidize dopamine nonpreferentially MAO transporters reuptake extracellular monoamine

26
MONOAMINE OXIDASE INHIBITORS (MAOIS)
History Isoniazid Iproniazid Isoniazid Both early drugs developed in sixties for anti tuberculosis but found to have antidepressant effects, got off market due to toxicity Iproniazid

27
MAOIs New antidepressant introduced but withdrawn due to liver toxicity, however, increased interest on hydrazines and hydrazides for antidepressants Iproniazide Antitubercular but CNS stimulant Which later shown to be MAOI resulting in NE & 5-HT Isoniazide Antitubercular but too polar hydrazines Thus MAOIs based on the hydrazine molecule have been extensively studied. Hydrazine, itself, has no MAOI activity Must have a free amino at one end to be active; a protonatable terminal N is necessary; those without a terminal N are prodrugs and must be bioactivated Must have at least one free hydrogen on each nitrogen

28
Monoamine Oxidase Monoamine oxidase (MAO) is an enzyme found in adrenergic and serotonergic nerve endings. Normal function of MAO is to break down norepinephrine and serotonin. In mental depression, there appears to be a decrease in the levels of brain norepinephrine and serotonin. Learning Outcomes 14.5 Explain the mechanism of action of the MAO inhibitors and describe the adverse effects and dietary restrictions relating to these drugs. Monoamine oxidase (MAO) is an enzyme found in most body cells but particularly in the adrenergic and serotonergic nerve endings. The normal function of MAO is to break down norepinephrine and serotonin into metabolites that are then excreted by the kidneys. MAO prevents the buildup of excessive levels of norepinephrine and serotonin in the brain and other body tissue. In mental depression, there appears to be an abnormal decrease in the levels of brain norepinephrine and serotonin. Drugs that inhibit, or block, MAO are called appropriately MAO inhibitors. By inhibiting MAO, these drugs decrease the amounts of norepinephrine and serotonin that are destroyed. Consequently, the MAO inhibitors permit the levels of norepinephrine and serotonin in the brain to increase.
 is an enzyme found in most body cells but particularly in the adrenergic and serotonergic nerve endings. The normal function of MAO is to break down norepinephrine and serotonin into metabolites that are then excreted by the kidneys. MAO prevents the buildup of excessive levels of norepinephrine and serotonin in the brain and other body tissue. In mental depression, there appears to be an abnormal decrease in the levels of brain norepinephrine and serotonin. Drugs that inhibit, or block, MAO are called appropriately MAO inhibitors. By inhibiting MAO, these drugs decrease the amounts of norepinephrine and serotonin that are destroyed. Consequently, the MAO inhibitors permit the levels of norepinephrine and serotonin in the brain to increase.")
29
Monoamine Oxidase Inhibitors
Consequently, the MAO inhibitors permit the levels of NE and serotonin in the brain to increase. They have many drug interactions; caution must be exercised with use of other drugs. Learning Outcomes 14.5 Explain the mechanism of action of the MAO inhibitors and describe the adverse effects and dietary restrictions relating to these drugs. In mental depression, there appears to be an abnormal decrease in the levels of brain norepinephrine and serotonin. Drugs that inhibit, or block, MAO are called appropriately MAO inhibitors. By inhibiting MAO, these drugs decrease the amounts of norepinephrine and serotonin that are destroyed. Consequently, the MAO inhibitors permit the levels of norepinephrine and serotonin in the brain to increase. The MAO inhibitors are involved in many drug interactions. Caution must be exercised if other drugs, especially other antidepressants, are administered during administration of MAO inhibitors and while MAO inhibitors remain in the system. Serious drug interactions can occur.

30
Monoamine Oxidase Inhibitor
Disadvantages of MOAIs: Dietary restrictions—tyramine Wine, beer, herring, certain cheeses Adverse effects: Dry mouth, urinary retention, constipation, blurred vision, hypotension, weight gain, sexual dysfunction, liver damage that may be fatal CNS: restlessness, dizziness, insomnia, tremors, seizures, (intensified with over dosage) Learning Outcomes 14.5 Explain the mechanism of action of the MAO inhibitors and describe the adverse effects and dietary restrictions relating to these drugs. One of the main disadvantages of MAO inhibitor therapy is the dietary restrictions. Many foods contain a substance known as tyramine, which causes the release of norepinephrine. When MAO is inhibited, tyramine may produce a massive release of norepinephrine, which can result in serious consequences, such as hypertensive crisis or cerebral stroke. Foods that normally contain tyramine include wine, beer, herring, and certain cheeses. In addition, certain sympathetic drugs used in the treatment of cold symptoms (decongestants and bronchodilators) interact with the MAO inhibitors. Common adverse effects include dry mouth, urinary retention, constipation, blurred vision, hypotension, weight gain, and sexual dysfunction. A variety of CNS disturbances including restlessness, dizziness, insomnia, tremors, and seizures may occur. These effects are intensified with overdosage. In addition, they can produce a type of liver damage that may be fatal.
 Learning Outcomes Explain the mechanism of action of the MAO inhibitors and describe the adverse effects and dietary restrictions relating to these drugs. One of the main disadvantages of MAO inhibitor therapy is the dietary restrictions. Many foods contain a substance known as tyramine, which causes the release of norepinephrine. When MAO is inhibited, tyramine may produce a massive release of norepinephrine, which can result in serious consequences, such as hypertensive crisis or cerebral stroke. Foods that normally contain tyramine include wine, beer, herring, and certain cheeses. In addition, certain sympathetic drugs used in the treatment of cold symptoms (decongestants and bronchodilators) interact with the MAO inhibitors. Common adverse effects include dry mouth, urinary retention, constipation, blurred vision, hypotension, weight gain, and sexual dysfunction. A variety of CNS disturbances including restlessness, dizziness, insomnia, tremors, and seizures may occur. These effects are intensified with overdosage. In addition, they can produce a type of liver damage that may be fatal.")
31
Monoamine Oxidase Inhibitor
Learning Outcomes 14.5 Explain the mechanism of action of the MAO inhibitors and describe the adverse effects and dietary restrictions relating to these drugs. One of the main disadvantages of MAO inhibitor therapy is the dietary restrictions. Many foods contain a substance known as tyramine, which causes the release of norepinephrine. When MAO is inhibited, tyramine may produce a massive release of norepinephrine, which can result in serious consequences, such as hypertensive crisis or cerebral stroke. Foods that normally contain tyramine include wine, beer, herring, and certain cheeses. In addition, certain sympathetic drugs used in the treatment of cold symptoms (decongestants and bronchodilators) interact with the MAO inhibitors. Common adverse effects include dry mouth, urinary retention, constipation, blurred vision, hypotension, weight gain, and sexual dysfunction. A variety of CNS disturbances including restlessness, dizziness, insomnia, tremors, and seizures may occur. These effects are intensified with overdosage. In addition, they can produce a type of liver damage that may be fatal.
 interact with the MAO inhibitors. Common adverse effects include dry mouth, urinary retention, constipation, blurred vision, hypotension, weight gain, and sexual dysfunction. A variety of CNS disturbances including restlessness, dizziness, insomnia, tremors, and seizures may occur. These effects are intensified with overdosage. In addition, they can produce a type of liver damage that may be fatal.")
32
MAO Inhibitors (nonselective)
MAOIS ON THE MARKET MAO Inhibitors (nonselective) Phenelzine (Nardil) Tranylcypromine (Parnate) Isocarboxazid (Marplan) MAO-B Inhibitors (selective for MAO-B) Selegiline (Emsam) Phenelzine – major depression Tranylcypromine – major depression Isocarboxazid – major depression Selegiline – comeback of MAOI (MAO-B inhibitor, more selective, loses selectivity at high doses) because no side effects from diet. Used primarily for treatment for Parkinson’s disease (also approved for major depression) – shows significant improvenemnt when taken with L-DOPA
 Phenelzine (Nardil) Tranylcypromine (Parnate) Isocarboxazid (Marplan) MAO-B Inhibitors (selective for MAO-B) Selegiline (Emsam) Phenelzine – major depression. Tranylcypromine – major depression. Isocarboxazid – major depression. Selegiline – comeback of MAOI (MAO-B inhibitor, more selective, loses selectivity at high doses) because no side effects from diet. Used primarily for treatment for Parkinson’s disease (also approved for major depression) – shows significant improvenemnt when taken with L-DOPA.")
33
MAOIS MECHANISM OF ACTION
MAO contains a cysteinyl-linked flavin MAOIs covalently bind to N-5 of the flavin residue of the enzyme MAOIs bind to the N-5 of the flavin residue if MAO, which prevents MAO from catalyzing the oxidative deamination of the monoamine, increasing their intracellular concentration so more can be released.

35
MAOIS SIDE EFFECTS Drowsiness/Fatigue Sleep disturbances Constipation
Muscle twitching Nausea Weight gain Diarrhea Blurred vision Dizziness Headache Low blood pressure Increased appetite Lightheadedness, Restlessness Decreased urine output Shakiness Weakness Decreased sexual function Increased sweating Bold ones are most common

36
MAOIS SIDE EFFECTS Side effects have put MAOIs in the second or third line of defense despite superior efficacy MAO-A inhibitors interfere with breakdown of tyramine High tyramine levels cause hypertensive crisis (the “cheese effect”) Can be controlled with restricted diet MAOIs interact with certain drugs Serotonin syndrome (muscle rigidity, fever, seizures) Pain medications and SSRIs must be avoided Major side effects have kept MAOI use limitied HUGE PITFALL IS DIETARY RESTRICTION Must avoid foods with high levels of tyramine like avocados, bananas, aged cheese, certain meats and wines This is however not seen with selegiline because that is a MAO-B inhibitor, and since tyramine displaces NOREPINEPHRINE from storage vesicles, it effects MAO-A more Serotonin syndrome is caused by drug interactions with herbal weight loss supplement (St John’s wort) and SSRIs and Pain meds like tramadol and meperidine
 Can be controlled with restricted diet. MAOIs interact with certain drugs. Serotonin syndrome (muscle rigidity, fever, seizures) Pain medications and SSRIs must be avoided. Major side effects have kept MAOI use limitied. HUGE PITFALL IS DIETARY RESTRICTION. Must avoid foods with high levels of tyramine like avocados, bananas, aged cheese, certain meats and wines. This is however not seen with selegiline because that is a MAO-B inhibitor, and since tyramine displaces NOREPINEPHRINE from storage vesicles, it effects MAO-A more. Serotonin syndrome is caused by drug interactions with herbal weight loss supplement (St John’s wort) and SSRIs and Pain meds like tramadol and meperidine.")
37
THE RECEPTOR SENSITIVITY HYPOTHESIS
Supersensitivity and up-regulation of post-synaptic receptors leads to depression Suicidal and depressed patients have increased 5HT-α2 receptors

38
Tricyclic Antidepressants
Drugs that block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings Produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blocking effects Learning Outcomes 14.4 Describe the mechanism of action and the adverse effects profile of the tricyclic antidepressants (TCAs). Tricyclic antidepressant drugs (TCAs or tricyclics) are so named because of the characteristic triple ring structure that they possess. The main action of the tricyclics and related antidepressant drugs is to block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings. The tricyclics and related drugs produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blockade.
. Tricyclic antidepressant drugs (TCAs or tricyclics) are so named because of the characteristic triple ring structure that they possess. The main action of the tricyclics and related antidepressant drugs is to block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings. The tricyclics and related drugs produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blockade.")
39
Tricyclic Antidepressants
Learning Outcomes 14.4 Describe the mechanism of action and the adverse effects profile of the tricyclic antidepressants (TCAs). Tricyclic antidepressant drugs (TCAs or tricyclics) are so named because of the characteristic triple ring structure that they possess. The main action of the tricyclics and related antidepressant drugs is to block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings. The tricyclics and related drugs produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blockade.
. Tricyclic antidepressant drugs (TCAs or tricyclics) are so named because of the characteristic triple ring structure that they possess. The main action of the tricyclics and related antidepressant drugs is to block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings. The tricyclics and related drugs produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blockade.")
40
Tricyclic Antidepressants
TCAs with a tertiary-amine side chain, including amitriptyline, doxepin, and imipramine, inhibit both norepinephrine and serotonin uptake. Clomipramine is somewhat selective for inhibition of serotonin uptake. Chemical modification of the TCA structure led to the earliest SSRI zimelidine. Imipramine has a phenothiazine-like structure (unlike the phenothiazines) had limited efficacy in schizophrenic patients, but improved symptoms of depression. Imipramine and related TCAs became the mainstay of drug treatment of depression until the later development of the SSRIs Learning Outcomes 14.4 Describe the mechanism of action and the adverse effects profile of the tricyclic antidepressants (TCAs). Tricyclic antidepressant drugs (TCAs or tricyclics) are so named because of the characteristic triple ring structure that they possess. The main action of the tricyclics and related antidepressant drugs is to block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings. The tricyclics and related drugs produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blockade.
 had limited efficacy in schizophrenic patients, but improved symptoms of depression. Imipramine and related TCAs became the mainstay of drug treatment of depression until the later development of the SSRIs. Learning Outcomes Describe the mechanism of action and the adverse effects profile of the tricyclic antidepressants (TCAs). Tricyclic antidepressant drugs (TCAs or tricyclics) are so named because of the characteristic triple ring structure that they possess. The main action of the tricyclics and related antidepressant drugs is to block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings. The tricyclics and related drugs produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blockade.")
41
Tricyclic Antidepressants
TCAs with a tertiary-amine side chain, including amitriptyline, doxepin, and imipramine, inhibit both norepinephrine and serotonin uptake. Clomipramine is somewhat selective for inhibition of serotonin uptake. Chemical modification of the TCA structure led to the earliest SSRI zimelidine which, while effective, was withdrawn from the market due to serious adverse effects. One of the compounds, imipramine, which has a phenothiazine-like structure, modified behavior in animal models. Unlike the phenothiazines, imipramine had limited efficacy in schizophrenic patients, but improved symptoms of depression. Imipramine and related TCAs became the mainstay of drug treatment of depression until the later development of the SSRIs Fluoxetine and fluvoxamine were the first widely used SSRIs. At the same time, selective inhibitors of norepinephrine reuptake entered clinical development; while not approved for use in the U.S. for the treatment of depression, one norepinephrine reuptake inhibitor, atomoxetine, is used for the treatment of attention deficit hyperactivity disorder. Subsequent drug development efforts focused on serotonin and norepinephrine reuptake inhibitors (SNRIs), resulting in venlafaxine and duloxetine, which lack the complex receptor pharmacology exhibited by the TCAs Learning Outcomes 14.4 Describe the mechanism of action and the adverse effects profile of the tricyclic antidepressants (TCAs). Tricyclic antidepressant drugs (TCAs or tricyclics) are so named because of the characteristic triple ring structure that they possess. The main action of the tricyclics and related antidepressant drugs is to block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings. The tricyclics and related drugs produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blockade.
, resulting in venlafaxine and duloxetine, which lack the complex receptor pharmacology exhibited by the TCAs. Learning Outcomes Describe the mechanism of action and the adverse effects profile of the tricyclic antidepressants (TCAs). Tricyclic antidepressant drugs (TCAs or tricyclics) are so named because of the characteristic triple ring structure that they possess. The main action of the tricyclics and related antidepressant drugs is to block the reuptake of norepinephrine and serotonin back into the neuronal nerve endings. The tricyclics and related drugs produce varying degrees of sedation, anticholinergic effects, and alpha-adrenergic blockade.")
42
TRICYCLIC ANTIDEPRESSANTS (TCAS)
Imipramine was first tried as an antipsychoti drug for schizophrenia, proved to be insufficient but proved to have antidepressant qualities, in the 50s around the same time as MAOIs. Imipramine is very good for severe depression, but it’s almost too good – also causes hypomania and mania Imipramine was first tried as an antipsychoti drug for schizophrenia, proved to be insufficient but proved to have antidepressant qualities, in the 50s around the same time as MAOIs. Imipramine is very good for severe depression, but it’s almost too good – also causes hypomania and mania Imipramine

43
TCAS MECHANISM OF ACTION
TCAs inhibit serotonin, norepinephrine, and dopamine transporters, slowing reuptake TCAs also allow for the downregulation of post-synaptic receptors All TCAs and SSRIs contain an essential amino group that appears to interact with Asp-98 in hSERT Less selective in which cells they target, will prevent serotonin, norepinephrine, and dopamine reuptake

44
TCAS MECHANISM OF ACTION
Less selective in which cells they target, will prevent serotonin, norepinephrine, and dopamine reuptake

45
TCAS SIDE EFFECTS Muscarinic M1 receptor antagonism - anticholinergic effects including dry mouth, blurred vision, constipation, urinary retention and impotence Histamine H1 receptor antagonism - sedation and weight gain Adrenergic α receptor antagonism - postural hypotension Direct membrane effects - reduced seizure threshold, arrhythmia Serotonin 5-HT2 receptor antagonism - weight gain (and reduced anxiety)
")
46
SELECTIVE SEROTONIN REUPTAKE INHIBITORS
Most commonly prescribed class Current drugs Mechanism of action Side effects Serotonin Also first rationally designed drug class, up until the 70s the antidepressants were sort of found by accident Serotonin is also referred to as 5-hydroxytryptamine

47
Selective Serotonin Reuptake Inhibitors
SSRIs were introduced from including fluoxetine, paroxetine, sertraline, citalopram, escitalopram, and fluvoxamine. The FDA has approved fluvoxamine for treatment of obsessive-compulsive disorder and social anxiety disorder, but not depression. Citalopram is labeled for use in premenstrual dysphoric disorder. All of the SSRIs show a clear improvement in safety margin compared to the TCAs and are much safer in overdose. Learning Outcomes 14.2 Describe the mechanism of action and adverse effects profile of the selective serotonin reuptake inhibitors (SSRIs). The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.
. The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.")
48
Selective Serotonin Reuptake Inhibitors
The SSRIs are effective in treating major depression. In typical studies SSRI treatment results in ~ 35% of patients enjoying a remission, SSRIs also are anxiolytics with demonstrated efficacy in the treatment of generalized anxiety, panic, social anxiety, and OCD. Sertraline and paroxetine also have been approved for the treatment of posttraumatic stress disorder (PTSD). Learning Outcomes as defined by a Hamilton Depression Rating Score < 7, indicative of a complete resolution of symptoms, compared to 25% of patients who experience a remission with placebo treatment (Rush et al., 2006). 14.2 Describe the mechanism of action and adverse effects profile of the selective serotonin reuptake inhibitors (SSRIs). The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.
. Learning Outcomes. as defined by a Hamilton Depression Rating Score < 7, indicative of a complete resolution of symptoms, compared to 25% of patients who experience a remission with placebo treatment (Rush et al., 2006) Describe the mechanism of action and adverse effects profile of the selective serotonin reuptake inhibitors (SSRIs). The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.")
49
Selective Serotonin Reuptake Inhibitors
SSRIs block the reuptake of serotonin back into the serotonergic nerve endings. This increases the serotonin available to work on the system. SSRIs are relatively selective, that is, 10-fold or more, for inhibition of SERT relative to NET. SSRIs are the preferred treatment for major depression and effective for PTSD and OCD. Learning Outcomes 14.2 Describe the mechanism of action and adverse effects profile of the selective serotonin reuptake inhibitors (SSRIs). The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.
. The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.")
50
Selective Serotonin Reuptake Inhibitors
SSRI treatment causes stimulation of 5-HT1A and 5-HT7 autoreceptors on cell bodies in the raphe nucleus and of 5-HT1D autoreceptors on serotonergic terminals. With repeated treatment with SSRIs, there is a gradual down-regulation and desensitization of these autoreceptor mechanisms. In addition, down-regulation of postsynaptic 5-HT2A receptors may contribute to antidepressant efficacy directly or by influencing the function of noradrenergic and other neurons via serotonergic heteroreceptors.

51
SSRI: Pharmacokinetics
All of the SSRIs are orally active and possess elimination half-lives consistent with once-daily dosing . In the case of fluoxetine, the combined action of the parent and the desmethyl metabolite norfluoxetine allows for a once weekly formulation (PROZAC WEEKLY). CYP2D6 is involved in the metabolism of most SSRIs and the SSRIs are at least moderately potent inhibitors of this isoenzyme. .
. CYP2D6 is involved in the metabolism of most SSRIs and the SSRIs are at least moderately potent inhibitors of this isoenzyme. .")
52
Selective Serotonin Reuptake Inhibitors
This creates a significant potential for drug interaction for post-menopausal women taking the breast cancer drug and estrogen antagonist, tamoxifen . The parent molecule is converted to a more active metabolite by CYP2D6. SSRIs may inhibit this activation and diminish the therapeutic activity of tamoxifen. Since venlafaxine and desvenlafaxine are weak inhibitors of CYP2D6, these antidepressants are not contraindicated in this clinical situation. However, care should be used in combining SSRIs with drugs that are metabolized by CYPs 1A2, 2D6, 2C9, and 3A4 (e.g., warfarin, tricyclic antidepressants, paclitaxel).
.")
53
Selective Serotonin Reuptake Inhibitors
Adverse effects: GI disturbances Dry mouth Sexual dysfunction Headache Nervousness Insomnia Tremors Learning Outcomes 14.2 Describe the mechanism of action and adverse effects profile of the selective serotonin reuptake inhibitors (SSRIs). The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.
. The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.")
54
Selective Serotonin Reuptake Inhibitors
The SSRIs, unlike the TCAs, do not cause major cardiovascular side effects. The SSRIs are generally free of antimuscarinic side effects (dry mouth, urinary retention, confusion), Do not block histamine or adrenergic receptors, and are not sedating. Learning Outcomes The favorable side effect profile of the SSRIs may lead to better patient compliance compared to that for the TCAs.
, Do not block histamine or adrenergic receptors, and are not sedating. Learning Outcomes. The favorable side effect profile of the SSRIs may lead to better patient compliance compared to that for the TCAs.")
55
Selective Serotonin Reuptake Inhibitors
Excessive stimulation of brain 5-HT2 receptors may result in insomnia, increased anxiety, irritability, and decreased libido, worsening prominent depressive symptoms. Excess activity at spinal 5-HT2 receptors causes sexual side effects including erectile dysfunction, and ejaculatory delay. Learning Outcomes The favorable side effect profile of the SSRIs may lead to better patient compliance compared to that for the TCAs.

56
Selective Serotonin Reuptake Inhibitors
Stimulation of 5-HT3 receptors in the CNS and periphery contributes to GI effects- nausea, diarrhea and emesis. Learning Outcomes The favorable side effect profile of the SSRIs may lead to better patient compliance compared to that for the TCAs.

57
Selective Serotonin Reuptake Inhibitors
Learning Outcomes 14.2 Describe the mechanism of action and adverse effects profile of the selective serotonin reuptake inhibitors (SSRIs). The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.
. The SSRIs are a group of drugs that have a very selective action to block the reuptake of serotonin (5HT) back into the serotonergic nerve endings. This action increases the concentration of 5HT in the synaptic cleft, which results in increased stimulation of serotonin receptors. The increase in 5HT activity in the limbic and cerebral cortical areas of the brain is believed to contribute to the antidepressant effect. The SSRIs have become preferred therapy for treatment of major depression. SSRIs are also effective in the treatment of most anxiety disorders such as posttraumatic stress disorder (PTSD) and obsessive-compulsive disorder (OCD). All the SSRIs listed cause GI disturbances including nausea, diarrhea, dry mouth, and anorexia. SSRIs also have been associated with sexual dysfunction, most commonly reduced sexual interest and delayed orgasm. Other CNS effects include headache, nervousness, insomnia, and tremors.")
58
Atypical SSRIs They block reuptake of serotonin and act on other neurotransmitters and receptors as well. (NE and/or Dopamine) Like the SSRIs, they have little effect in blocking cholinergic, adrenergic, or histamine receptors. Learning Outcomes 14.3 Explain the major difference between the SSRIs and the atypical SSRI antidepressants. The atypical SSRI antidepressant drugs block reuptake of serotonin like the SSRIs but have additional actions on other neurotransmitters and receptors. The atypical drugs affect serotonin and other neurotransmitters such as norepinephrine and dopamine.

59
Atypical SSRIs Learning Outcomes
14.3 Explain the major difference between the SSRIs and the atypical SSRI antidepressants. The atypical SSRI antidepressant drugs block reuptake of serotonin like the SSRIs but have additional actions on other neurotransmitters and receptors. The atypical drugs affect serotonin and other neurotransmitters such as norepinephrine and dopamine.

60
Atypical SSRIs:Bupropion
Appears to act via multiple mechanisms: enhances noradrenergic and dopaminergic neurotransmission via reuptake inhibition Also involve the presynaptic release of NE and DA . Indicated for depression, prevention of seasonal depressive disorder, and as a smoking cessation treatment . Improve symptoms of attention deficit hyperactivity disorder (ADHD). Used in combination with SSRIs to obtain a greater antidepressant response. Bupropion has effects on sleep EEG that are opposite those of most antidepressant drugs. Dapoxetine: Premature Ejaculation Escitalopram: Major depression and various other anxiety disorders Fluxoetine: Major depression, OCD, bulimia, etc Fluvoxamine: OCD Paroxetine: Major depression or anxiety Sertraline: Major depression or anxiety Zimelidine had neurological problems like Guillan Barre Indalpine had problems with fetal low WBC
. Used in combination with SSRIs to obtain a greater antidepressant response. Bupropion has effects on sleep EEG that are opposite those of most antidepressant drugs. Dapoxetine: Premature Ejaculation. Escitalopram: Major depression and various other anxiety disorders. Fluxoetine: Major depression, OCD, bulimia, etc. Fluvoxamine: OCD. Paroxetine: Major depression or anxiety. Sertraline: Major depression or anxiety. Zimelidine had neurological problems like Guillan Barre. Indalpine had problems with fetal low WBC.")
61
Atypical SSRIs:Bupropion
The terminal phase of bupropion elimination has a t1/2 of 21 hours. The elimination involves both hepatic and renal routes. Decreased dose should also be made in cases of renal impairment. More trade names once patent is over but I kept original trade names Citalopram: Major depression Dapoxetine: Premature Ejaculation Escitalopram: Major depression and various other anxiety disorders Fluxoetine: Major depression, OCD, bulimia, etc Fluvoxamine: OCD Paroxetine: Major depression or anxiety Sertraline: Major depression or anxiety Zimelidine had neurological problems like Guillan Barre Indalpine had problems with fetal low WBC

62
Atypical SSRIs:Bupropion
Adverse effects: At doses higher than that recommended for depression (450 mg/day), the risk of seizures increases significantly. The use of extended release formulations often blunts the maximum concentration observed after dosing. and minimizes the chance of reaching drug levels associated with an increased risk of seizures.
, the risk of seizures increases significantly. The use of extended release formulations often blunts the maximum concentration observed after dosing. and minimizes the chance of reaching drug levels associated with an increased risk of seizures.")
63
Atypical SSRIs:Bupropion
Drug interaction: The major route of metabolism is CYP2B6. Does not appear to be metabolised by CYP2D6 and this drug is frequently administered with SSRIs. However, the potential for interactions with drugs metabolized by CYP2D6 should be kept in mind until the safety of the combination is firmly established.

64
Drug interaction : Selective Serotonin Reuptake Inhibitors
Paroxetine, fluoxetine are potent inhibitors of CYP2D6. This inhibition can result in disproportionate increases in plasma concentrations of drugs metabolized by CYP2D6. A prominent interaction is the increase in TCA exposure that may be observed during co-administration of TCAs and SSRIs. Most antidepressants, including the SSRIs, exhibit drug-drug interactions based on their routes of metabolism CYPs.

65
Drug interaction : Selective Serotonin Reuptake Inhibitors
MAOIs enhance the effects of SSRIs due to inhibition of serotonin metabolism. Administration of these drugs together can produce synergistic increases in extracellular brain serotonin, leading to the serotonin syndrome. Other drugs that may induce the serotonin syndrome include: methylenedioxymethamphetamine. Another important drug-drug interaction with SSRIs occurs via a pharmacodynamic mechanism

66
Drug interaction : Selective Serotonin Reuptake Inhibitors
SSRIs should not be started until at least 14 days following discontinuation of treatment with an MAOI. For all SSRIs, 14 days should pass prior to beginning treatment with an MAOI following the end of treatment with an SSRI. Exception: fluoxetine. MAOIs bind irreversibly to MAO and block the enzymatic metabolism of monoaminergic neurotransmitters. this allows for synthesis of new MAO. Since the active metabolite norfluoxetine has a t1/2 of 1-2 weeks, at least 5 weeks should pass between stopping fluoxetine and beginning an MAOI.

67
Atypical SSRIs:Bupropion
Drug interaction: The major route of metabolism is CYP2B6. Does not appear to be metabolised by CYP2D6 and this drug is frequently administered with SSRIs. However, the potential for interactions with drugs metabolized by CYP2D6 should be kept in mind until the safety of the combination is firmly established.

68
Atypical SSRIs:Bupropion
Drug interaction: The major route of metabolism is CYP2B6. Does not appear to be metabolised by CYP2D6 and this drug is frequently administered with SSRIs. However, the potential for interactions with drugs metabolized by CYP2D6 should be kept in mind until the safety of the combination is firmly established.

69
Atypical SSRIs:Bupropion
Drug interaction: The major route of metabolism is CYP2B6. Does not appear to be metabolised by CYP2D6 and this drug is frequently administered with SSRIs. However, the potential for interactions with drugs metabolized by CYP2D6 should be kept in mind until the safety of the combination is firmly established.

70
SSRIS SIDE EFFECTS Anhedonia Extremely vivid and strange dreams Apathy
Dizziness Nausea/vomiting Fatigue Drowsiness or somnolence Changes in sexual behavior Headache Suicidal thoughts Bruxism (involuntarily grinding of the teeth)
")
71
Summary Q: What was the first Antidepressant, and what is its mech of action? Iproniazid Q: Describe the clinical effects of tyramine toxicity ncreases the release of NE When a person is on an MAOI and also consumes tyramine containing foods/drinks, there is NE overload which can cause hypertensive crisis. Many side effects go away onec the body gets used to the drug because the drug takes sometime to start working Sexual side effects are common (ED, low libido) due to stimuatlion of 5-HT2 receptors leading to less release of dopamine
 due to stimuatlion of 5-HT2 receptors leading to less release of dopamine.")
72
MAOIs Second line treatment, due to side effect profile
potentially lethal food and drug interactions Still used for refractory depression Venlafaxine is a racemix mixture While SSRIs are less potent than the other classes of drugs, they have more manageable side effects so they’re considered better The mechanism is similar to SSRIs, as are the side effects. However, the rate of suicide for SNRIs has been debateable, especially venlafaxine. Finnish study showed Ven increased suicide risk 1.6 times compared to no treatment while Fluoxetine halved it. FDA study showed 5-fold increase in <25 so it is contraindicated in adolescents.

73
Adverse Effects of TCA's
Significant Overdose Potential due to narrow therapeutic window. Cardiovascular Toxicity (potential for fatal cardiac arrythmia). Side effects: anti-histaminergic (weight gain, drowsiness) anti-cholinergic (constipation, blurred vision, dry mouth, drowsiness again) anti-alpha adrenergic (dizziness, decreased BP) ) Bupropion is a racemic mixture
. Side effects: anti-histaminergic (weight gain, drowsiness) anti-cholinergic (constipation, blurred vision, dry mouth, drowsiness again) anti-alpha adrenergic (dizziness, decreased BP) ) Bupropion is a racemic mixture.")
74
Compare the efficacy and side effects for Secondary amine TCA's vs Tertiary amine TCA's
Tertiary amines have greater alpha, histamine 1, and muscarinic blockade. Secondary amines are newer, have fewer side effects, are less sedating, and hold less overdose risk. Bupropion is a racemic mixture

75
Issues in antidepressant therapy
Important issue in the use of antidepressants is a phenomenon known as the "switch" from a depressed episode to a manic or hypomanic episode, a challenge in managing bipolar illness. For this reason, antidepressants are not recommended as monotherapy for bipolar illness. SSRIs and bupropion may be somewhat less likely to induce the switch from depression to mania than antidepressants from other pharmacological classes.

76
Issues in antidepressant therapy
A controversial issue regarding the use of all antidepressants is their relationship to suicide. The FDA has issued a "black box" warning regarding the use of SSRIs and a number of other antidepressants in children and adolescents, particularly during the early phase of treatment, due to the possibility of an association between antidepressant treatment and suicide.

77
Drugs Serotonin Receptor Antagonists
Several antagonists of the 5-HT2 family of receptors are effective antidepressants, although most agents of this class affect other receptor classes as well. The class includes two pairs of close structural analogues, trazodone and nefazodone, as well as mirtazapine and mianserin (not marketed in the U.S.).
.")
79
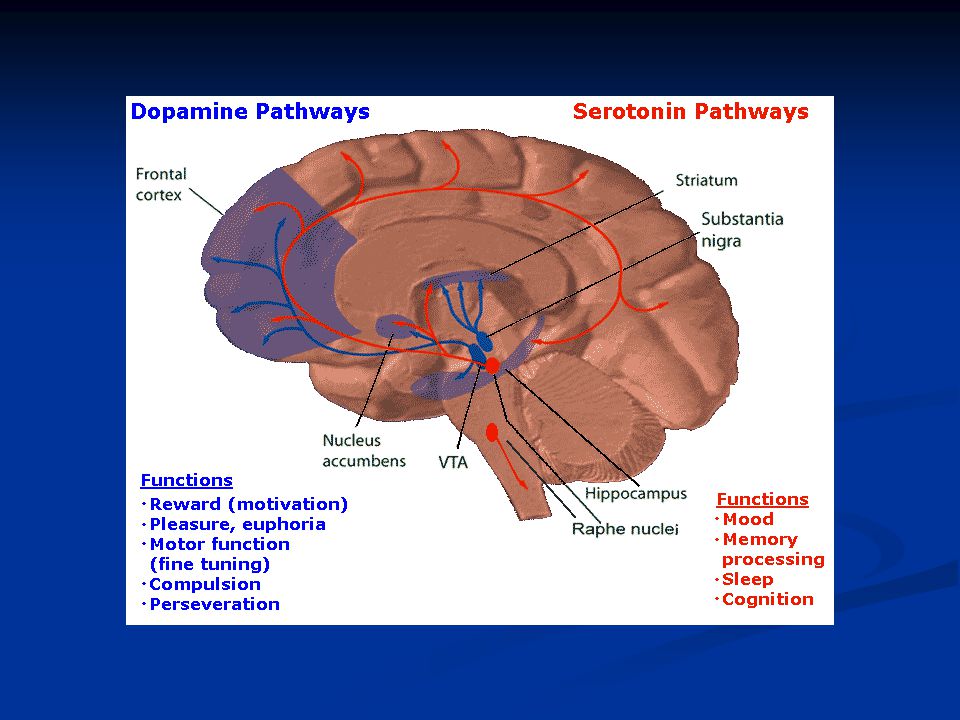
the nucleus of the brain that uses serotonin, and locations to which its neurons project:
5HT neurons project to: Frontal Limbic Brainstem Hypothalamus

80
Serotonin Antagonist & Reuptake Inhibitors
Its an SSRI that also blocks the 5HT2A-R (overall, its less activating and more sedating than the SSRI's Used to treat depression, anxiety, insomnia AND no associated weight gain OR sexual dysfunction Adverse: Sedation, orthostatic hypotention, priapism (rare Yet its rarely used, not 1st line

81
Serotonin vs Norepinephrine Therapeutic Effects and Side Effects
Overall, Serotonin is more of a calming agent, NE more of a stimulating agent Serotonin - therapeutically acts on mood, anxiety, and obsessions NE - acts on mood, attention, and improves low energy states. Serotonin side effects - sexual dysfunction, GI, Insomnia, Akasthesia NE side effects - Tremor, elevated BP/HR, urinary retention

82
5-HT1 Receptors preferentially couple to Gi/o ; inhibit adenylyl cyclase. The 5-HT1A, 5-HT1B, & 5-HT1D activate a receptor-operated K+ channel and inhibit a voltage-gated Ca2+ channel. The 5-HT1A is found in raphe nuclei of the brainstem- functions as an inhibitory, somatodendritic autoreceptor on cell bodies of serotonergic neurons. Another 5-HT1 subtype, the 5-HT1D/1B, functions as an autoreceptor on axon terminals, inhibiting 5-HT release.

83
5-HT2 Receptors 3subtypes of 5-HT2 couple to Gq/G11 proteins and activate phospholipase C, generating 2 second messengers: diacylglycerol and inositol trisphosphate. 5-HT2A and 5-HT2C receptors also activate phospholipase A2 -release of arachidonic acid. 5-HT2A : broadly distributed in the CNS, serotonergic terminal. Also in prefrontal, parietal, and somatosensory cortex, in blood platelets and smooth muscle cells. 5-HT2B found in stomach fundus, where they are abundant. The expression of 5-HT2B receptors is highly restricted in the CNS.

84
5-HT3 Receptors The 5-HT3 receptor is the only monoamine neurotransmitter receptor function as a ligand-operated ion channel. Activation of 5-HT3 elicits a rapidly desensitizing depolarization, mediated by the gating of cations. Located on parasympathetic terminals in the GI tract, including vagal and splanchnic afferents. In the CNS, in the solitary tract nucleus and in the area postrema. 5-HT3 receptors in both the GI tract and the CNS participate in the emetic response, providing a basis for the anti-emetic property of 5-HT3 receptor antagonists.

85
5-HT4 Receptors 5-HT4 couple to Gs to activate adenylyl cyclase.
distributed throughout the body. on neurons of the superior and inferior colliculi and in the hippocampus in CNS. In the GI tract, 5-HT4 are located on neurons of the myenteric plexus and on smooth muscle and secretory cells. Stimulation of the 5-HT4 receptor evokes secretion and facilitates the peristaltic reflex. Effects of pharmacological manipulation of 5-HT4 receptors on memory and feeding in animal models suggest possible clinical applications in the future

86
5-HT Receptors on CNS A multitude of brain functions are influenced by 5-HT, including sleep, cognition, sensory perception, motor activity, temperature regulation, nociception, mood, appetite, sexual behavior, and hormone secretion. The principal cell bodies of 5-HT neurons are located in raphe nuclei of the brainstem and project throughout the brain and spinal cord. release of serotonin occurs at sites of axonal swelling, termed varicosities, which do not form distinct synaptic contacts. Such non-synaptic release is consistent with the idea that 5-HT acts as a neuromodulator as well as a neurotransmitter.

87
Sleep-Wake Cycle Control of the sleep-wake cycle is one of the first behaviors in which a role for 5-HT was identified. Depletion of 5-HT with p-chlorophenylalanine, a tryptophan hydroxylase inhibitor, elicits insomnia that is reversed by the 5-HT precursor, 5-hydroxytryptophan. Conversely, treatment with L-tryptophan or with nonselective 5-HT agonists accelerates sleep onset and prolongs total sleep time.

88
Aggression and Impulsivity
5-HT serves a critical role in aggression and impulsivity. Pharmacological studies of aggressive behavior in laboratory animals suggest a role for 5-HT. 5-HT1B receptors in the development of neuronal pathways important in aggression or a direct role in the mediation of aggressive behavior.

89
Anxiety and Depression
The effects of 5-HT–active drugs in anxiety and depressive disorders, like the effects of selective serotonin reuptake inhibitors (SSRIs), strongly suggest a role for 5-HT in the neurochemical mediation of these disorders. Mutant mice lacking the 5-HT transporter display anxiety and a "depressive-like" phenotype.
, strongly suggest a role for 5-HT in the neurochemical mediation of these disorders. Mutant mice lacking the 5-HT transporter display anxiety and a depressive-like phenotype.")
90
Anxiety and Depression

91
Mech of Action: Serotonin-Norepinephrine Reuptake Inhibitors
SNRIs inhibit both SERT and NET. SNRIs cause enhanced serotonergic and/or noradrenergic neurotransmission. Similar to the action of SSRIs, the initial inhibition of SERT induces activation of 5-HT1A and 5-HT1D autoreceptors. This action decreases serotonergic neurotransmission by a negative feedback mechanism until these serotonergic autoreceptors are desensitized. Then, the enhanced serotonin concentration in the synapse interact with postsynaptic 5-HT receptors.

92
Serotonin Receptor Antagonists
antagonists of the 5-HT2 are effective antidepressants, although most agents of this class affect other receptor classes as well. The class includes two pairs of close structural analogues, trazodone and nefazodone, mirtazapine (REMERON, others) and mianserin. Trazodone and nefazodone block 5-HT2 and alfa1 adrenergic receptors. Trazodone also inhibits the serotonin transporter, but is markedly less potent relative to its blockade of 5-HT2A receptors.
 and mianserin. Trazodone and nefazodone block 5-HT2 and alfa1 adrenergic receptors. Trazodone also inhibits the serotonin transporter, but is markedly less potent relative to its blockade of 5-HT2A receptors.")
93
Differential Diagnosis: Other mood and anxiety disorders
Symptoms of mood disorders may overlap (e.g., dysthymia and MDD) Diagnosis is often based on history – and patient’s memory of past symptoms may be unreliable
 Diagnosis is often based on history – and patient’s memory of past symptoms may be unreliable.")
94
Medical conditions Thyroid abnormalities Cortisol abnormalities
Parkinson’s disease Multiple sclerosis Epilepsy Brain tumor Cancer (e.g., pancreatic) Dementia Traumatic brain injury Autoimmune disorders Stroke Huntington’s disease Chronic infections Certain medications: Steroids Interferon Beta-blockers Isotretinoin (Accutane) Oral contraceptives Antidepressants (!!) Everything else?!?
 Dementia. Traumatic brain injury. Autoimmune disorders. Stroke. Huntington’s disease. Chronic infections. Certain medications: Steroids. Interferon. Beta-blockers. Isotretinoin (Accutane) Oral contraceptives. Antidepressants (!!) Everything else !")
95
Substance-induced mood disorder
Alcohol: depression Cocaine: hypomania, mania Amphetamines: hypomania, mania PCP, ketamine: hypomania, mania Heroin: depression? Marijuana: depression? Mood symptoms with intoxication or withdrawal May take weeks-months to normalize mood Substance use highly comorbid in mood disorders (bipolar I > bipolar II > MDD)
")
96
Long-term effects: Antidepressant drugs
Long-term effects of antidepressant drugs evoke adaptive or regulatory mechanisms that enhance the effectiveness of therapy. These responses include increased adrenergic or serotonergic receptor density or sensitivity, increased receptor-G protein coupling and cyclic nucleotide signaling, induction of neurotrophic factors, and increased neurogenesis in the hippocampus. hanced serotonergic or noradrenergic neurotransmission achieved by an alternative pharmacological mechanism.

97
Long-term effects: Antidepressant drugs
Chronic treatment with some antidepressants that interact directly with monoamine transporters (e.g., SSRIs, SNRIs, or NE reuptake inhibitors) reduces the expression and activity of 5-HT or NE transporters in the brain, which results in enhanced serotonergic or noradrenergic neurotransmission. Sustained signaling via NE or 5-HT increases the expression of specific downstream gene products, particularly brain-derived neurotrophic factor (BDNF).
 reduces the expression and activity of 5-HT or NE transporters in the brain, which results in enhanced serotonergic or noradrenergic neurotransmission. Sustained signaling via NE or 5-HT increases the expression of specific downstream gene products, particularly brain-derived neurotrophic factor (BDNF).")
98
Suggested history/workup
Review of current and past psych sx/dx Get collateral history Review prior treatments and response Family history Medical history Current medications Substance use history Social history Review of systems Workup CBC Electrolytes Renal function Liver Function TSH RPR? HIV? Imaging?

99
Treatment/management
ALWAYS ASSESS FOR SUICIDE!!! Ideation, plan, intent, means, risk factors Choose medications carefully and thoughtfully Don’t give up too soon Can always incorporate some behavioral and CBT techniques (e.g., behavioral activation) Address perpetuating factors (medical problems, psychosocial stressors) Treat the acute AND chronic aspects of the illness (i.e., preventive management)
 Address perpetuating factors (medical problems, psychosocial stressors) Treat the acute AND chronic aspects of the illness (i.e., preventive management)")
100
Case #1a Mr. M is a 34 y/o man who presents with 1-month history of sad mood and decreased motivation to go to work. He reports difficulty falling asleep at night and multiple mid-cycle awakenings. His appetite and energy are normal. What other questions do you have? What is your working diagnosis? What is your initial treatment plan? Was reprimanded by his boss 2.5 weeks ago; works as civil engineer for Seattle – worried he isn’t qualified for the job, may get laid off. No wt change, some feelings of worthlessness. No hopelessness. No SI. Still enjoys doing things around the house and hobbies. Married with one child, good relationship with family. No other stressors. Positive family history for bipolar d/o in mother.

101
Case #1b Mr. M returns one month later. He continues to have sad mood, decreased motivation, and feels that things are getting worse. What other questions do you have? What is your working diagnosis? What is your treatment plan? Sleep is worsening. App decr with 5lb wt loss. Anhedonia. Thoughts of death.

102
Case #2a Ms. T is a 19 y/o female college student who presents to the emergency room with a several day history of bizarre behavior at school. Her friends say she hasn’t slept for 4-5 days, is talking “a mile a minute,” and is trying to help everybody do their homework stating, “you’ll never find a better tutor than me!!” What other questions do you have? What is your working diagnosis? What is your treatment plan? Consider amphetamine use (no doz?)
")
103
Case #2b Ms. T does well during the hospitalization and is discharged in about 8 days. She returns to clinic in 4 weeks and says she thinks she’s ready to come off the medication. What other questions do you have? What do you tell her? Consider amphetamine use (no doz?)
")
104
Case #2c Ms. T stops her medications. She returns to see you in another 4 weeks and tells you she feels great – especially since she’s “off of those mind-dulling drugs.” She feels much more alert and is able to accomplish “more than ever before.” She says she is doing well with just 5 hours sleep per night and feels that she’s finally “found” herself. What other questions do you have? What is your working diagnosis (has it changed)? What is your treatment plan? Consider amphetamine use (no doz?)
 What is your treatment plan Consider amphetamine use (no doz )")
105
Case #2d Ms. T refuses to re-start medications. Eight weeks later, she is brought into the emergency room after an acetaminophen OD. You evaluate her during the medical hospitalization. She reports 4-5 weeks of worsening “emptiness,” difficulty falling asleep, racing thoughts, and feeling “revved up.” She has had increasing SI over the past week. What other questions do you have? What is your working diagnosis (has it changed)? What is your treatment plan? Consider amphetamine use (no doz?)
 What is your treatment plan Consider amphetamine use (no doz )")
106
Case #3a Patient is a 6-7 y/o gray male donkey who complains that “no one really cares about me.” He states that he generally feels down and never has enough energy. What other questions do you have? What is your working diagnosis? What is your treatment plan? How many other psychiatric diagnoses can you identify in the writings of A.A. Milne? Tigger-hypomania, Pooh-GAD, Owl-NPD

107
Case #3b He returns 4 weeks later and tells you he doesn’t really feel any better. What other questions do you have? What is your working diagnosis? What is your treatment plan? How many other psychiatric diagnoses can you identify in the writings of A.A. Milne? Tigger-hypomania, Pooh-GAD, Owl-NPD

Similar presentations
 Bind to receptor site but do not cause an action Bind to receptor site but do not cause an action.>")





 are a class of powerful antidepressant drugs. They are particularly effective in treating.>")
: Lengthy, uninterrupted periods of depressed mood. Manic.>")











