Download presentation
Presentation is loading. Please wait.

1
Novel methods of treatment of diabetic patients
Novel methods of treatment of diabetic patients. Oral hypoglycemic agents, modern insulin preparations and its analogues. assist. prof. Svystun I.I.

2
Good Diabetes Management
Regular Blood Glucose Monitoring Healthy Nutrition Regular Exercise

4
Guidelines for glycaemic control in DM
IDF AACE (2011) ADA HbA1c (%) <6.5 ≤6.5 <7.0 Fasting/ preprandial glucose (mmol/L/ mg/dL) <6.0 / <110 / 2-h postprandial glucose <7.8 / <140 <10.0 / <180
 ADA. HbA1c (%) <6.5. ≤6.5. <7.0. Fasting/ preprandial glucose. (mmol/L/ mg/dL) <6.0 / < / h postprandial glucose. <7.8 / <140. <10.0 / <180.")
5
Criteria of DM compensation

8
DCCT A1C levels and the risk of complications in type 1 diabetes
Patients with type 1 diabetes (n=1,441) Adapted from DCCT. Diabetes 1995;44:
 Adapted from DCCT. Diabetes 1995;44:")
10
UKPDS: Tight glycamic control prevents complications

12
(A) Association of severe hypoglycemia with mortality in intensive and standard treatment groups in ACCORD replotted from Bonds et al. (2010). (B) Association of severe hypoglycemia with mortality in intensive and standard treatment groups in ADVANCE replotted from Holman et al. (2009).
 Association of severe hypoglycemia with mortality in intensive and standard treatment groups in ADVANCE replotted from Holman et al. (2009).")
13
Dedov et al. Diabetes mellitus. 2011;4:6-17. © 2011,Diabetes Mellitus.
Treatment goal HbA1c Age Young Middle Eldery and/or life expectancy <5 years No complications No risk of hypoglycemia <6,5% < 7,0% <7,5% Severe complications and /or risk of hypoglycemia < 8,0% Dedov et al. Diabetes mellitus. 2011;4:6-17. © 2011,Diabetes Mellitus.

14
≤7% ≥7% < 8,5 > 6,0 An A1C ≤6.5% may be targeted in some patients with type 2 diabetes to further lower the risk of nephropathy and retinopathy but this must be balanced against the risk of hypoglycemia Less stringent A1C targets (7.1%–8.5% in most cases) may be appropriate in patients with type 1 or type 2 diabetes with any of the following: a) Limited life expectancy b) High level of functional dependency c) Extensive coronary artery disease at high risk of ischemic events d) Multiple comorbidities e) History of recurrent severe hypoglycemia f) Hypoglycemia unawareness g) Longstanding diabetes for whom it is difficult to achieve an A1C ≤7.0% despite effective doses of multiple antihyperglycemic agents, including intensified basal-bolus insulin therapy ADA: Executive Summary: Standards of Medical Care in Diabetes—2012; Diabetes Care January 2012
 may be appropriate in patients with type 1 or type 2 diabetes with any of the following: a) Limited life expectancy. b) High level of functional dependency. c) Extensive coronary artery disease at high risk of ischemic events. d) Multiple comorbidities. e) History of recurrent severe hypoglycemia. f) Hypoglycemia unawareness. g) Longstanding diabetes for whom it is difficult to achieve an A1C ≤7.0% despite effective doses of multiple antihyperglycemic agents, including intensified basal-bolus insulin therapy. ADA: Executive Summary: Standards of Medical Care in Diabetes—2012; Diabetes Care January")
15
Methods of treatment DM
Education Exercise program. Diet. Oral hypoglycemic agents or insulin (indications for each vary with the type of DM and severity of the disease).
.")
16
Self - control Physician has to educate: - techniques of insulin administration and measurement of urine and blood glucose level (if taking insulin)
")
17
Exercise Exercise: Before diabetic patients engage in exercise program, they should consult with their healthcare provider because they need to have a complete history and physical examination Exercise (total of about 30 minutes a day, at least 5 days a week) lowers blood sugar levels by improving cell uptake of glucose.
 lowers blood sugar levels by improving cell uptake of glucose.")
18
The main principles of diet
Balanced diet (diet should include physiologic meal components: carbohydrate comprises 50 – 60 % of total calories, fat – 24 – 25 % and protein – 16 – 15 %).
.")
19
The main principles of diet.
Normal-calorie diet in patients with type 1 DM (35-50 kcal/kg of ideal weight (weight = height – 100)) and low-calorie diet in obese persons (mostly in patients with type 2 DM (20 – 25 kcal/kg of ideal weight)). We try to decrease weight in obese patients on 1-2 kg/month by such diet.
) and. low-calorie diet in obese persons (mostly in patients with type 2 DM (20 – 25 kcal/kg of ideal weight)). We try to decrease weight in obese patients on 1-2 kg/month by such diet.")
20
Oral hypoglycemic agents.
Inadequate control of hyperglycemia by the diet and exercises interventions suggests the need for a good glucose-lowering agent. Oral hypoglycemic agents are useful only in the chronic management of patients with type 2 DM. The most commonly used are: sulfonilureas, biguanides, alpha-glucosidase inhibitors, non-sulfonylureas insulin stimulators (glinides), thiazolidinediones (glitazones), dipeptidyl peptidase IV (DPP-IV) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonist, analogue of amylin (pramlintide)
, thiazolidinediones (glitazones), dipeptidyl peptidase IV (DPP-IV) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonist, analogue of amylin (pramlintide)")
21
Commonly used sulfonylureas

22
Action of sulfonilureas
1. Influence on the pancreatic gland: increasing of the β-cells sensitivity to the glucose and as a result higher secretion of insulin; stimulation of the exocytosis of insulin by insulocytes; 2. Nonpancreatic influence: increasing number of the receptors to insulin; normalization of receptors’ sensitivity to insulin; increasing of glucose transportation inside muscle cells; stimulation of glycogen synthesis; decreasing of glycogenolysis and glyconeogenesis; decreasing of glucagon secretion and others.

24
Side effects of sulfonilureas
hypoglycemia (hypoglycemic effect of sulfonilureas will be the most obvious in 7 – 12 days from the beginning of the treatment); allergy; influence on gastrointestinal tract (nausea and others); leucopenia (decreasing of the quantity of white blood cells); primary or secondary resistance; weight gain .
; allergy; influence on gastrointestinal tract (nausea and others); leucopenia (decreasing of the quantity of white blood cells); primary or secondary resistance; weight gain .")
25
Contrandications to sulfanilureas usage
type 1 DM; blood diseases; acute infections, acute coronary heart and cerebral diseases; trauma; pregnant diabetics or lactation; III – IV stages of angiopathy (but Glurenorm can be used in patients chronic renal failure, because of gastrointestinal tract excretion); coma and precoma.
; coma and precoma.")
26
Commonly used biguanides

27
Action of biguanides

28
Contraindications to biguanides usage
type 1 DM; heart and lung disease with their insufficiency (chronic heart and lung failure); status with hypoxemia; acute and chronic liver and kidney diseases with decreased function; pregnant diabetics, lactation; old age; alcoholism; coma and precoma.
; status with hypoxemia; acute and chronic liver and kidney diseases with decreased function; pregnant diabetics, lactation; old age; alcoholism; coma and precoma.")
29
Alpha-glucosidase inhibitors

30
Action of alpha-glucosidase inhibitors
inhibition of gastrointestinal tract absorption (block of α-glucozidase); lowering of postprandial glucose level (postprandial “spikes” in blood glucose are increasingly implicated as a major cause of cardiovascular complications); partly reducing fasting glucose levels by indirectly stimulating insulin secretion in patients who retain β-cell function (and acarbose has a protective effect on β-cells).
; lowering of postprandial glucose level (postprandial spikes in blood glucose are increasingly implicated as a major cause of cardiovascular complications); partly reducing fasting glucose levels by indirectly stimulating insulin secretion in patients who retain β-cell function (and acarbose has a protective effect on β-cells).")
31
Contrandications to alpha-glucosidase inhibitors
type 1 DM; Chronic gastrointestinal disorders: pancreatitis, colitis, hepatitis. Side effects of alpha-glucosidase inhibitors - flatulence, abdominal bloating, diarrhea.

32
Non-sulfanylureas insulin stimulators

33
Action of non-sulfanylureas insulin stimulator.
Stimulation of insulin production at meal times; very rapid absorbtion from the intestine and metabolism in the liver; (plasma half-life is less than 1 hour).
.")
34
Indications to non-sulfanylureas insulin stimulator.
- can be used in elderly with type 2 DM (due to short half-life) and in renal impairment (because it is metabolized in liver). Contraindications to non-sulfanylureas insulin stimulator. - as for the sulfanilureas Side effects of non-sulfanylureas insulin stimulator. - hypoglycemia, transient elevation of liver enzymes, rash and visual disturbances.
 and in renal impairment (because it is metabolized in liver). Contraindications to non-sulfanylureas insulin stimulator. - as for the sulfanilureas. Side effects of non-sulfanylureas insulin stimulator. - hypoglycemia, transient elevation of liver enzymes, rash and visual disturbances.")
35
Commonly used thiazolidinediones

36
Action of thiazolidinediones

37
Contraindications to thiazolidinediones usage
Diabetic coma, precoma, ketoacidosis; Acute and chronic diseases of the liver; Heart failure; Pregnancy, lactation; Children, teenagers; Allergic reactions to the drug.

38
GLP-1 Analogues Exenatide Liraglutide
Synthetic form of Exendin-4, derived from the salivary secretions of the Gila monster lizard (Heloderma suspectum) Liraglutide Novel long-acting analog obtained by acylation of GLP-1 with fatty acid chain
 Liraglutide. Novel long-acting analog obtained by acylation of GLP-1 with fatty acid chain.")
39
Exendin-4 in the Gila Monster Plasma Exendin-4 Concentration (pg/mL)
Exendin-4 was originally isolated from the salivary secretions of the Gila monster Exendin-4 was subsequently found to circulate as a meal-related peptide in this animal 400000 300000 Plasma Exendin-4 Concentration (pg/mL) 200000 Exendin-4 is present in high concentration in the saliva of the Gila monster. It is secreted 4x greater in response to an oral glucose stimulus compared to an intravenous stimulus similar to the incretin effect seen in human subjects. 100000 3 6 9 12 Time After Meal (h) Data from Young AA. Insulin Resistance and Insulin Resistance Syndrome 2002,
 Exendin-4 is present in high concentration in the saliva of the Gila monster. It is secreted 4x greater in response to an oral glucose stimulus compared to an intravenous stimulus similar to the incretin effect seen in human subjects Time After Meal (h) Data from Young AA. Insulin Resistance and Insulin Resistance Syndrome 2002,")
40
GLP-1 Modes of Action in Man
Upon ingestion of food… Slows gastric emptying Reduces food intake GLP-1 is secreted from the L-cells in the jejunum and ileum Suppresses glucagon secretion Stimulate insulin secretion only when blood glucose concentration is elevated Long term effects demonstrated in animals… Increases beta-cell cell mass and maintains beta-cell efficiency Drucker DJ. Curr Pharm Des 2001; 7: Drucker DJ. Mol Endocrinol 2003; 17:

41
Structure of native GLP-1 and two GLP-1 analogues
97% homology to native GLP-1 53% homology to native GLP-1 41

42
Exenatide (Byetta) Pen prefill- one month’s supply
Given bid, minutes prior to meal (250 cal) Nausea experienced by almost all initially, typically remits within days Start at 5 mcg BID, then increase to 10 mcg BID after 1 month Current indication: failing SFU, metformin, or both Not FDA approved with insulin or monotherapy Pancreatitis warning Continue exenatide only if a person has a reduction in HbA1c>1% and >3% of initial body weight in 6 months
 Nausea experienced by almost all initially, typically remits within days. Start at 5 mcg BID, then increase to 10 mcg BID after 1 month. Current indication: failing SFU, metformin, or both. Not FDA approved with insulin or monotherapy. Pancreatitis warning. Continue exenatide only if a person has a reduction in HbA1c>1% and >3% of initial body weight in 6 months.")
43
LIRAGLUTIDE 97% homologous with native human GLP-1
Half life of hours Permitting once daily injection 1.2 and 1.8 mg/day Added to metformin, it reduces HbA1c by 1.5% (p<0.01) Main side effects are nausea and vomiting
 Main side effects are nausea and vomiting.")
44
Inhibition of DPP-4 Increases Active GLP-1
Mixed meal Intestinal GLP-1 release GLP-1 (7-36) active GLP-1 (7-36) active DPP-4 DPP-4 inhibitor GLP-1 (9-36) inactive Adapted from Rothenberg P, et al. Diabetes. 2000;49(suppl 1):A39.
 active. GLP-1 (7-36) active. DPP-4. DPP-4 inhibitor. GLP-1 (9-36) inactive. Adapted from Rothenberg P, et al. Diabetes. 2000;49(suppl 1):A39.")
45
Summary of DPP-4 Inhibition
Increases fasting and postprandial GLP-1 levels Reduces fasting and postprandial glycemia Improves ß-cell function Increases insulin secretion, reduces proinsulin/insulin ratio Increases beta-cell mass Inhibits glucagon secretion Reduces hepatic glucose production Increases insulin sensitivity Reduces postprandial lipemia No effect on gastric emptying or body weight Reduces HbA1c by ~1% Is safe and tolerable in short term In renal impairment, dose decreased by 50%

46
SITAGLIPTIN Licensed for use in T2DM at a dose of 100 mg once a day
Can be added to metformin, a glitazone, a sulfonylurea or a sulfonylurea+metformin, when current regime does not achieve glycemic control HbA1c reduction of 0.5-1% Weight neutral and low risk of hypoglycemia Post prandial glucose also reduced (p<0.05) compared to placebo Slightly higher rates of constipation, nasopharyngitis and dizziness
 compared to placebo. Slightly higher rates of constipation, nasopharyngitis and dizziness.")
47
VILDAGLIPTIN Licensed at a dose of 50 mg once or twice daily
In T2DM as dual oral therapy Reduces HbA1c by % Reduces postprandial glucose Weight neutral and low risk of hypoglycemia Main side effects are headache, nosopharyngitis, dizziness

48
DPP-4 inhibitors Continue DPP-4 inhibitor therapy only if there is a reduction of >0.5% HbA1c in 6 months DPP-4 inhibitor is preferable to a Glitazone if further weight gain would cause significant problems TZDs are contraindicated

49
Therapy Expected A1c (%) decrease with monotherapy Lifestyle modifications Metformin Sulfonylurea GLP-1 agonist TZD a-glucosidase inhibitor Glinide DPP-IV inhibitor Pramlintide Insulin unlimited

50
ADA Algorithm for Management of Diabetes Diabetes Care
2009 Tier 1: Well-validated core therapies At diagnosis: Lifestyle + Metformin Lifestyle+Metformin + Basal Insulin Lifestyle+Metformin + Intensive insulin Lifestyle+Metformin + Sulfonylurea Step 1 Step 2 Step 3 Tier 2: less well-validated therapies Lifestyle+Metformin + Pioglitazone Sulfonylurea Lifestyle+Metformin + Pioglitazone (No hypoglycemia, edema, CHF, bone loss) *Useful when hypoglycemia is to be avoided Lifestyle+Metformin + GLP1 (No hypoglycemia, wt loss, Nausea/vomiting) Lifestyle+Metformin + Basal Insulin Amylin agonists, Glinides DPP-4 inhibitors may be appropriate in selected patients
 *Useful when hypoglycemia is to be avoided. Lifestyle+Metformin. + GLP1. (No hypoglycemia, wt loss, Nausea/vomiting) Lifestyle+Metformin. + Basal Insulin. Amylin agonists, Glinides. DPP-4 inhibitors may be appropriate in selected patients.")
52
Management of Hyperglycemia in Type 2 Diabetes: A Patient-Centered Approach: Position Statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). 2012 Inzucchi SE, Bergenstal RM, Buse JB, et al. Diabetes Care Apr 19.

53
From the history of insulin
Best Banting Macleod Collip

54
Indications for insulin therapy
1. All patients with type 1 DM. 2. Some patients with type 2 DM: uncontrolled diabetes by diet or oral hypoglycemic agents; ketoacidosis, coma; acute and chronic liver and kidneys disease with decreased function; pregnancy and lactation; II – IV stages of angiopathy; infection diseases; acute heart and cerebral diseases; surgery.

55
Insulin Type+(Trade Name) Onset of Action Peak Duration
Nursing Intervention Rapid-acting (Clear) Insulin Lispro (Humalog) Insulin Aspart (Novorapid) Apidra (insulin glulisine) 10-15min 60-90min 4-5hrs Take within 15 min before meals or within 20 min after meals Short Acting/Regular Insulin (clear) Humulin R 30-60 2-4hrs 5-8hrs Take 30 min before meals Intermediate-acting (cloudy) (NPH/Lente) 1-4hrs 4-12hrs 18-24hrs Ultra Lente and Glargine (clear) 4-8hrs 18hrs 24-38hrs Note: Glargine can not be mixed with any other insulin Premixed: 10/90, 20/80, 30/70, 40/60, 50/50 (cloudy) ideal time to give patients with their premixed is 30 min before their meal, with their meal and after their meal Drawing up Insulin: Clear then cloudy to avoid contaminating the clear insulin
 Insulin Lispro (Humalog) Insulin Aspart (Novorapid) Apidra (insulin glulisine) 10-15min min. 4-5hrs. Take within 15 min before meals or within 20 min after meals. Short Acting/Regular Insulin (clear) Humulin R hrs. 5-8hrs. Take 30 min before meals. Intermediate-acting (cloudy) (NPH/Lente) 1-4hrs. 4-12hrs hrs. Ultra Lente and Glargine. (clear) 4-8hrs. 18hrs hrs. Note: Glargine can not be mixed with any other insulin. Premixed: 10/90, 20/80, 30/70, 40/60, 50/50 (cloudy) ideal time to give patients with their premixed is. 30 min before their meal, with their meal and after their meal. Drawing up Insulin: Clear then cloudy to avoid contaminating the clear insulin.")
56
Insulin preparations of ultrashort action (human analog, recombinant)
beginning maximum duration NovoRapid (Insulin aspart) Novo-Nordisk 2-10 min min 3 - 5 h Humalog (insulin lispro) Lilly Apidra (insulin glulisine)
 Novo-Nordisk min min h. Humalog (insulin lispro) Lilly. Apidra (insulin glulisine)")
57
Insulin preparations of short action
beginning maximum duration Humodar R 100 Indar - human insulin (semi-synthetic) 30 min 1 - 3 h 5 - 8 h Humodar R 100 R Indar - human insulin (recombinant) Farmasulin H (regular insulin human injection, [rDNA origin]) Farmak Actrapid (НМ) Novo-Nordisk Humulin R (regular insulin human injection, [rDNA origin]), Lilly Insuman rapid (regular insulin human injection, [rDNA origin]) Sanofi-aventis
 30 min h h. Humodar R 100 R Indar - human insulin (recombinant) Farmasulin H (regular insulin human injection, [rDNA origin]) Farmak. Actrapid (НМ) Novo-Nordisk. Humulin R (regular insulin human injection, [rDNA origin]), Lilly. Insuman rapid (regular insulin human injection, [rDNA origin]) Sanofi-aventis.")
58
Insulin preparations of intermediate action
beginning maximum duration Humodar B 100 R Indar 1 – 1,5 h 6 - 8 h 12 – 18 h Farmasulin Н NР Farmak Protaphan (МС, НМ) Novo-Nordisk Insuman basal Aventis Humulin NPH Lilly Monotard НМ Novo-Nordisk
 Novo-Nordisk. Insuman basal Aventis. Humulin NPH Lilly. Monotard НМ Novo-Nordisk.")
59
Insulin preparations of long action
beginning maximum duration Farmasulin Н L Farmak 3 – 4 h h 24 – 30 h Ultralente Humulin Lilly Ultratard НМ Glargine (Lantus)Aventis - (human analog, recombinant) 24 h Detemir (Levemir) Novo Nordisk
Aventis. - (human analog, recombinant) 24 h. Detemir (Levemir) Novo Nordisk.")
60
Insulin preparations combined

62
Storing and Handling Insulin
Opened bottles stored at room temperature (15 to 30°C). If stored in a refrigerator, unopened bottles are good until the expiration date printed on the bottle. Opened bottles that are stored in a refrigerator should be used within one month of being opened. Protect your insulin (bottles, pens, and cartridges) from extremes of hot and cold. Never store your insulin in the freezer - once insulin is frozen, it loses its potency.
. If stored in a refrigerator, unopened bottles are good until the expiration date printed on the bottle. Opened bottles that are stored in a refrigerator should be used within one month of being opened. Protect your insulin (bottles, pens, and cartridges) from extremes of hot and cold. Never store your insulin in the freezer - once insulin is frozen, it loses its potency.")
63
Initiation and modification of insulin therapy
It is started as soon as possible in an attempt to “rest” the damaged islet cells and help to “induce” a remission (“honeymoon” phase). 1 Unite It is activity of 0,04082 mg of crystalic insulin (standart)
. 1 Unite. It is activity of 0,04082 mg of crystalic insulin (standart)")
64
Initiation and modification of insulin therapy
We can use traditional or multiple component insulin program. The last is better. Advantages include the following: hypoglycemic reactions may be decreased or prevented because smaller doses of insulin are needed; more physiologic match of insulin to meals is achieved.

65
Initiation and modification of insulin therapy to achieve diabetic control. Step 1: Estimate Total Daily Insulin (TDI) The daily insulin requirement in patients: on the first year of the disease is 0,3 – 0,5 unite of insulin per kilogram of body weight (0,5 – if the patient with ketosis or DKA); on the next years is 0,6 – 0,8 – 1,0 unite/ kg of body weight.
; on the next years is 0,6 – 0,8 – 1,0 unite/ kg of body weight.")
67
Initiation and modification of insulin therapy
2/3 of the total daily dose we give before breakfast, 1/3 in the evening and then make correction due to the glucose blood level. Insulin doses should be given 30 minutes before meals to allow for adequate absorption of regular insulin. It using three or four shots of short-acting insulin (1/3 of total daily dose) plus intermediate-acting (2/3 of total daily dose) insulin daily twice a day.
 plus intermediate-acting (2/3 of total daily dose) insulin daily twice a day.")
68
2/3 TDI 1/3 TDI

70
Treatment of type 2 DM

71
NPH-Based Multiple-Dose Insulin Therapy (MDI)
2 injections: • Premix 70/30 before AM and evening meal OR NPH + R/aspart/lispro/glulisine (ratio 2:1) before AM and evening meal; mix insulins in same syringe. Starting Dose: units/kg/day divided as follows: 2/3 morning, 1/3 evening; before meals
 before AM and evening meal; mix insulins in same syringe. Starting Dose: units/kg/day divided as follows: 2/3 morning, 1/3 evening; before meals.")
75
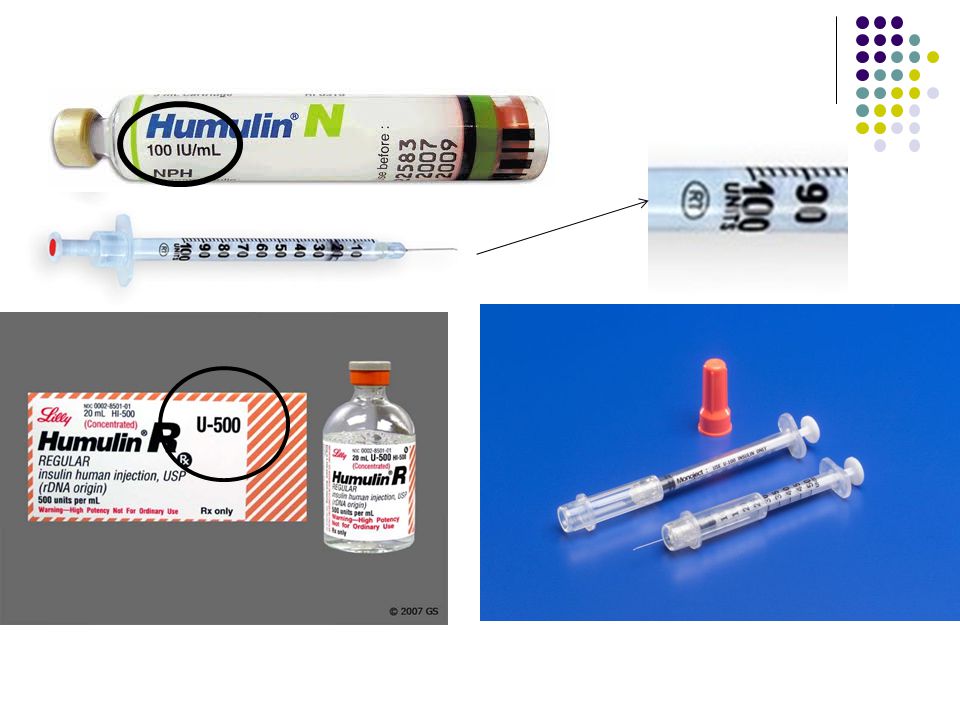
Methods of delivery insulin
Intravenous (IV) Syringes (SC) Pens Jet injectors Insulin pumps
 Syringes (SC) Pens. Jet injectors. Insulin pumps.")
77
Site Selection for the Injections
4 major areas: Arms-posterior surface Abdomen-avoid 1 inch area around navel Thighs-anterior surface Hips Note: Systematic rotation of injection sites within an anatomic area to prevent lipodystrophy. Administering each injection 0.5-1inch away from the previous injection.

78
Some peculiarities of insulin therapy:
insulin acts faster when is administrated i/v; subcutaneous and intramuscular absorption of insulin is decreased in the dehydrated or hypotensive patients; the most rapid absorption from the abdomen; exercise accelerates insulin absorption (before planned exercise program patient has to decrease insulin dose or take more caloric diet).
.")
80
Side effects (complications) of insulin therapy.
1. Hypoglycemia. - This complication represents insulin excess and it can occur at any time (frequently at night (common symptom: early-morning headache)). - Precipitating factors: irregular ingesting of food; extreme activity; alcohol ingestion; drug interaction; liver or renal disease; hypopituitarism; adrenal insufficiency.
). - Precipitating factors: irregular ingesting of food; extreme activity; alcohol ingestion; drug interaction; liver or renal disease; hypopituitarism; adrenal insufficiency.")
81
Side effects (complications) of insulin therapy.
1. Hypoglycemia It is a syndrome characterized by symptoms of sympathetic nervous system stimulation or central nervous system dysfunction that are provoked by an abnormally low plasma glucose level. Hypoglycemia represents insulin excess and it can occur at any time.

82
Side effects (complications) of insulin therapy
2. Somogyi effect (Somogyi phenomenon, rebound effect). It is caused by overinsulinization: hyperglycemia proceeded by insulin – induced hypoglycemia. Hypoglycemia causes an increase in the secretion of the counterregulatory hormones (glucagon, epinephrine, cortisol, growth hormone), which inhibit insulin secretion and increase glucose output by the liver (as a result of the stimulation of glucogenolysis and glucogenesis). Treatment: gradual reduction of insulin dose.
. It is caused by overinsulinization: hyperglycemia proceeded by insulin – induced hypoglycemia. Hypoglycemia causes an increase in the secretion of the counterregulatory hormones (glucagon, epinephrine, cortisol, growth hormone), which inhibit insulin secretion and increase glucose output by the liver (as a result of the stimulation of glucogenolysis and glucogenesis). Treatment: gradual reduction of insulin dose.")
83
Side effects (complications) of insulin therapy
3. Dawn phenomenon. Many patients with type 1 DM demonstrate an early morning (4 – 8 a.m.) rise in glucose levels, because of activation of counterregulatory hormones. It may be confused with the Somogyi phenomenon. Sampling of glucose levels throughout the night might help differentiate the two conditions. Treatment: some have recommended an earlier injection in the morning (5 – 6 a.m.), and most suggest a late evening (before bedtime) injection of intermediate-acting insulin.
 rise in glucose levels, because of activation of counterregulatory hormones. It may be confused with the Somogyi phenomenon. Sampling of glucose levels throughout the night might help differentiate the two conditions. Treatment: some have recommended an earlier injection in the morning (5 – 6 a.m.), and most suggest a late evening (before bedtime) injection of intermediate-acting insulin.")
84
Side effects (complications) of insulin therapy
4. Allergic reactions. These include burning and itching at the site of insulin injection; skin rash; vasculaties; purpura and anaphylactic reaction. Treatment: - antihistamines; - changing of standard insulin to pure pork insulin or to human insulin; - in extreme cases – glucocorticoids.

85
Side effects (complications) of insulin therapy
5. Insulin resistance. - Clinical status characterized by insulin resistance: obesity; therapy with oral contraceptives; glucocorticoid therapy; acromegaly; Cushing’s syndrome; acanthosis nigricans; chronic liver or renal disease. - Non-true insulin resistance may be caused by long-time injections of insulin into the one site.

86
Side effects (complications) of insulin therapy
6. Lipodystrophy. - It is atrophy or hypertrophy of the adipose tissue, which occur at the site of insulin injection. - Treatment: changing the site of injection; the usage of human insulin.

87
Thank you for attention!

Similar presentations

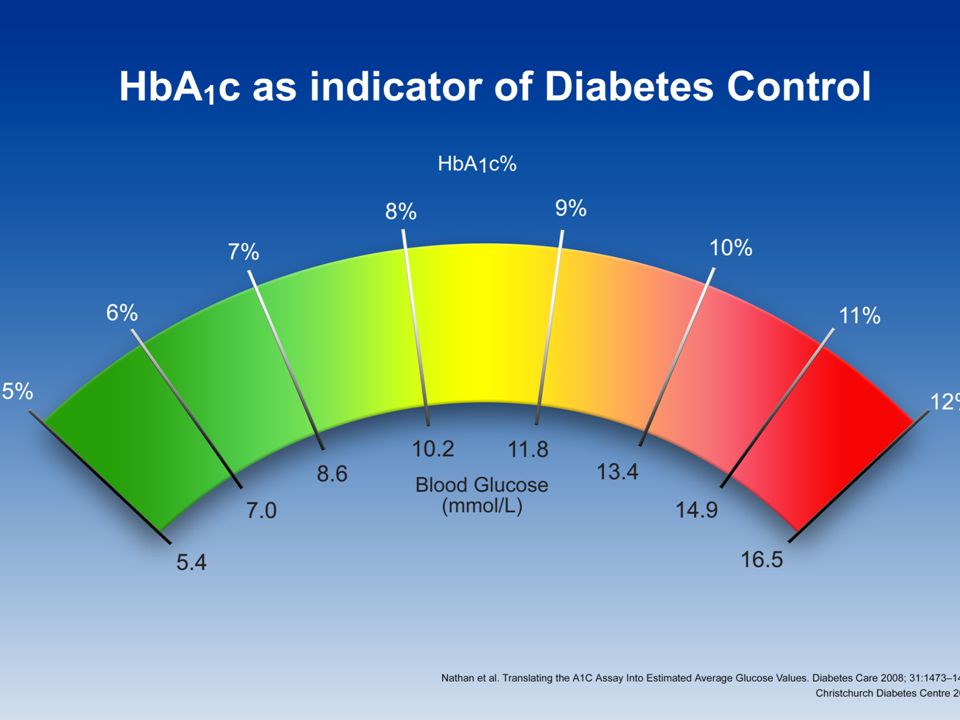













 HbA1c – IFFC (mmol/mol) 6.042 6.548 7.053 7.559 8.064 9.075.>")

![Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]](/15/4663650/big_thumb.jpg "Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]>")








>")





