Download presentation
Presentation is loading. Please wait.

1
MODERATOR:DR KHAIRUDDIN

2
Mr A,58 years old Malay gentleman, retired teacher Underlying hpt and diabetis mellitus under GP follow up Chronic smoker,30 sticks cigarettes /day History of fall from stairs 7 years ago, experienced shooting pain from buttock to right calve but no muscle weakness not seek medical treatment Went to traditional massage Worsening for 1 year, shooting pain untill both calves assc. with numbness right foot, unable perform ‘rukuk’ during prayer due to pain, disturb daily activities Seek medical treatment,diagnosis: PID with right sciatica pain, under ortho follow up Manage with physiotheraphy and analgesic ( gabapentin 300mg od + celebrex 200mg prn)
.")
3
Physical examinations:alert concious pink, bmi 25 (weight 71kg, height 1.68m) Back:no deformity, no tenderness, straight leg raise positive on right side,power 3/5 right lower limb, sensory intact Other systems were unremarkabke Xray lumbosacral:reduced interverttebral space at t12,l1
 Back:no deformity, no tenderness, straight leg raise positive on right side,power 3/5 right lower limb, sensory intact Other systems were unremarkabke Xray lumbosacral:reduced interverttebral space at t12,l1")
4
Proceed with mri lumbosacral:revealed mixed enhancing solid-cystic intradural lesion at level L4 could be due to an ependymoma with impression intradural lesion L4 Differential: astrocytoma, metastasis spinal mets ? Primary Referred to neurosurgery for intradural mass

5
Was seen by neurosurgical with plan for laminectomy L2-L5 and excision of intradural tumour Refer to anaest clinic

6
First seen in anaest clinic 23/10/2013, plan operation 10/11/2013 He was walking Underlying chronic smoker, hypertension and DM with no other comorbidities or complaint Bp 130/75mmhg, hr 79, weight 71kg, height 1.68m, bmi 25.2 Airway: interdental gap > 3fb, malampati 2, thyromental distance > 4fb, no neck abnormality, normal dentition

7
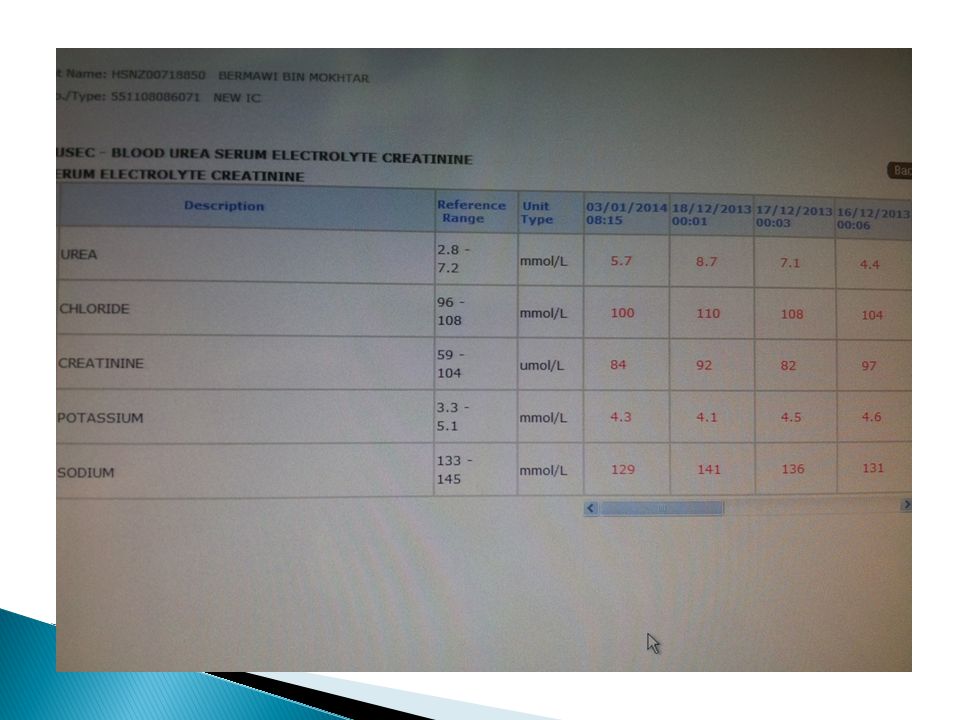
Other systemic review were unremarkable Ecg cxr normal Hb 14.1/plt 174/twbc 8 Buse:4.4/136/4.7/99, creat 76 Classsified as ASA II

8
Admit ward 1 day prior to operation Advised to stop smoking To bring antihypertensive & DM medications to ward Knbm at 2am Tab midazolam 7.5mg on and once ot call Repeat all blood investigation once admitted to ward Gsh as protocol Case d/w with specialist, for AIBP, ICU back up

9
He admitted to ward 9/11/2013 to 2ef and again seen for preop assessment No recent urti/no sob/chest pain/failure symptoms o/e alert concious pink, TMD> 3fb,Malamapati III, good neck extension Lungs clear, cvs s1s2 no murmurs Bp 117/72, hr 82

10
Knbm 2am Optimised bp, aim < 140/90mmhg Continue antihypertensive drug on morning of op with sip of clear fluid Start sliding scale once knbm Aim discan 6-10mmol/l Gxm per protocol Gac,AIBP, ICU back up Case d/w anaest specialist:may need icu back up if anticipate long ot time

11
Operation done in acc ot Seen patient before push to ot, noted features of difficult intubation, tmd 2fb, small chin, poor denture He was lying flat but look uncomfortable, asking for any snoring during sleeping and he admit he was snoring but resolved with positioning,need to sleep 2 pillow, felt more comfortable No daytime somnolence, apnoea

12
He were on and off cough, heard like chesty, but no urti.he said the cough was normal like that many years already. Never admitted due to lungs infection before. Anticipate difficult intubation-activated for standby difficult intubation devices, bougy, glidescope, procile.suction functioning Case attempted with 2 specialist, trainee and 2 medical officer

13
Attach monitoring devices, bp 132/74, hr 74 Spo2 100% under ra ivl functioning well Put patient in 30 degree Preoxygenation given longer with 100% O2 Difficult intubation devices and glidescope standby Oral suction done

14
Induced with iv fentanyl 100mcg, profopol 140mg Able to ventilate but with some difficulties Iv scoline 100mg given Laryngoscopy done, unable to visualised the epiglottis, seen large mass whitish in colour obstructed the laryngeal inlet Pass stat to specialist Spo2 maintain 100%

15
Unable to intubate, obstructed airway Secretion +++ from oral cavity Difficult to ventilate, given o2 100% Start desaturated, proseal inserted, still difficult to ventilate desat till spo2 34%, patient blue Good head thin chin lift applied Wake up patient No episode of bradycardia or hypotensive episode during hypoxia episode

16
After patient had spontaneous breathing, tidal volume increasing slowly, spo2 increased but best under 100% oxygen was 92% Not tachypnoic After fully awake, explained regarding the incidence and need for referral on table to ent team for diagnostic airway assessment (ent surgeon just next operation theater) Refer on table to ent collegue next door
 Refer on table to ent collegue next door")
17
Iv glycopyrulate 200mcg given Prepare for fibreoptic videoscope Left nasal packed with gauze soaked with coccaine Fibreoptic videoscope attempted by ent surgeon

19
Findings: glandular mass at base of tongue Cystic mass > right side of epiglottis anterior surface Piriform fossa and valleculae look clear Posterior pharyngeal wall are bulky and inflammed Narrow airway, all tissues oedematous

20
Operation abandoned Suggest by ent surgeon to get biopsy and further ent assessment before proceed op in view anticipate difficult intubation next time with possibility of tracheostomy.

22
Anest plan for next operation to combine ent and neurosurgical Was plan for ct neck early Laryngoscope done by consultant ent next day with the findings same as videoscope, vocal cord moving symmetrical with phonation, no vc mass next day Patient was discharged home with tca ent clinic 25/11/2013

23
Patient had no new complaints No voice changes, noisy breathing, sob, loa/low, urti Laryngoscope done: findings same as before discharged Cxr clear Explained need for biopsy to confirm the diagnosis, plan elms+biopsy on 2/12/2013 Refer anaest clinic, 27/11/2013, admit ward 1/12

24
Imp: soft tissu mass at base of tongue with cystic epiglottic mass and supraglottic soft tissue mass causing oropharyngeal and hypopharyngeal airways obstruction. Diff:lymphoma,hypopharyngeal carcinoma with cervical lymphadenopaties

27
Nil new complaint, alert,pink Bp 121/67,hr 84 Airway assessment:interdental gap>3fb, malampati 2, tyromental distance <4fb, poor dentition Other systemic review were unremarkable Cxr clear, ecg sr, nil ischaemic changes Blood investigations all within normal range

28
Gac, fibreoptic intubation, icu back up Advised to stop smoking Was explained high risk for icu admission in view had airway obstruction, and nature of awake fibreoptic intubation.patient understood and agreed Case d/w specialist incharge,for awake fibreoptic intubation, icu back up

29
Elective admitted to ward 6A for elms+biopsy Nil complaints Details airway assessment done in ent clinic flexible endoscopy : no deviated nasal septum, it hypertrophy adenoid 50% enlarged retropalate collapse < 50% retrolingual collapse> 50% during normal inspiration (lateral collapse)
")
30
Lateral pharyngeal wall redundant Base of tongue-redundant tissue(hyperplasia of base of tongue) Mass at right lingual surface of epigglotis Epiglottic rigid, not easily collapse Aryepiglottic fold/aryhtenoid normal Vestibular fold redundant Present of ? Fatty tissue accumulation Vocal cord normal No mass at true cord Subglottic area clear, no mass No collapsing wall at level of upper trachea

31
Plan for op as plan next morning with high risk consent and icu back up Next morning, case not proceed after further detail discussion from anaesthetic and surgeon. Not to risk patient with unindicated tracheostomy by surgeon. plan to combine with neurosurgical team Discharged home with next operation was plan combined ent and neurosurgical team on 15/12/2013

32
Mr A admitted 1/7 before op, classified as ASA III with icu backup, awake fibreoptic intubation Attended in ot 2 anaesthetics, 2 mo Alert concious, bp 142/92, hr 92,spo2 100% under RA Difficult intubations trolley standby nearby, fibreoptic ready

33
Iv glycopyrulate 200mcg, fentanyl 100mcg given Nasal pack with cocaine Preoxygenation given Awake fibreoptic intubation done using armoured size 7 anchored at 26cm succesfully Spo2 maintain 100% during procedure Iv propofol 120mg, esmeron 30mg given Connected to ventilator tv 425ml, rate 12, peep 4 Proceed op first with laminectomy L4 and excision intradural mass at 1200noon

34
Anaesthesia maintained with TIVA remifentanyl/propofol Intraop, bp stable Minimal blood loss Op uneventhful Ended neurosurgical op at 1545h, op almost 4 hours

35
Proceed with DL+biopsy+ excision of epiglottic mass at 1620 after reposition patient from prone to supine Nil complications during operation.ended case at 1730h, op 1hour 10minutes Not proceed with tracheostomy, trial of weaning in icu

36
Neurosurgical:well defined smooth surface, solid and cystic tumour firmly adherent to 2 nerve roots.90% excision of tumour with small part of tumour capsule adherent to nerve root was coagulated and left in-situ IMP:neurofibroma Intraoperatively monitoring showed 10% improvement

37
Ent: mass(retention cyst)arising from tip of epiglottis, broad base, ruptured with cheesy material ++, cystic sac excised with microscissor, redundant mucosa of lateral pharyngeal wall, arytenoid swollen and bulky IMP: epiglottic retention cyst Plan: for iv dexamethasone 8mg tds 3/7
arising from tip of epiglottis, broad base, ruptured with cheesy material ++, cystic sac excised with microscissor, redundant mucosa of lateral pharyngeal wall, arytenoid swollen and bulky IMP: epiglottic retention cyst Plan: for iv dexamethasone 8mg tds 3/7")
38
Admitted icu for weaning Need high sedation post op in view patient restless Patient haemodinamically stable in icu D1 post op was plan for extubation but patient apnoe on cpap, done direct videoscope in icu through right nasal cavity which unable to pass through the videoscope Proceed with glidescope, noted soft tissue swelling surrounding the supraglottic area, erythematous, cannot visualised epiglottis

39
Was then plan for DL+ Trachy by ent on 17/12/2012-D2 post op Patient intubated sedated, In ot, attended by 3 anaesthetics Direct laryngoscope done, noted bilateral enlarged tonsil(almost kissing)distorted anatomy Glidescope: able to visualize epiglottis and anterior vocal cord, both oedematous Proceed tracheostomy by ent, uneventhful
distorted anatomy Glidescope: able to visualize epiglottis and anterior vocal cord, both oedematous Proceed tracheostomy by ent, uneventhful")
40
Trachea slunted deep, slight deviated to left side Thyroid enlarged Ishmectomy done, part of thyroid tissue cut, bleeding secured Direct laryngoscopy-supraglottic region oedematous, redundant mucosa of pharyngeal wall Only can visualised tip of epiglottis Unable to access vocal cord due to limited view

41
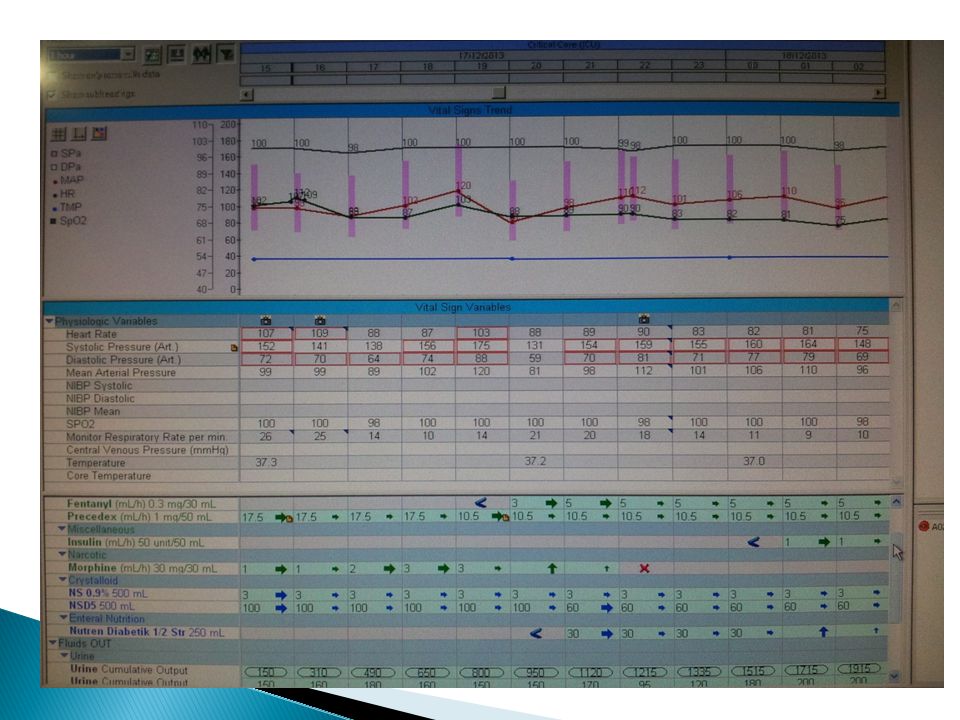
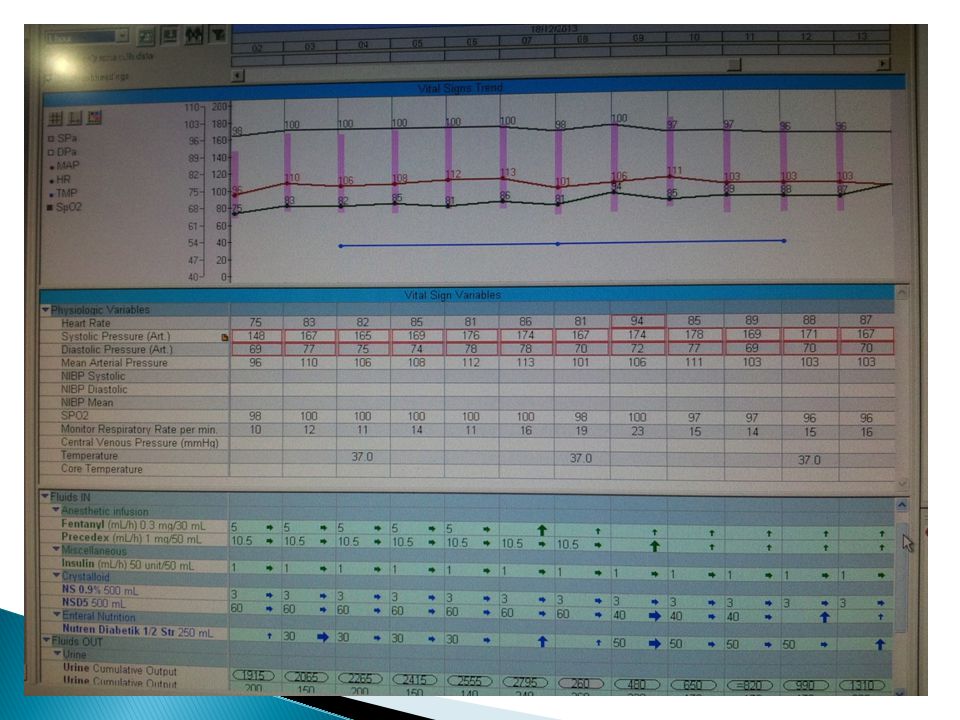
Post tracheostomy, weaning in icu Able maintain spo2> 95% under tracheventimask, patient alert concious and haemodinamically stable Discharged to general ward after D1 post tracheostomy, D3 post laminectomy L4+ excision intradural tumour, D3 post direct laryngoscopy+biopsy+ excision epiglottis mass

42
Throughout ICU stay, nil complications encountered.Hemodinamically stable, able wean ventilator setting,good renal profile, tolerate feeding well, discan well controlled and sepsis parameter static, no documented fever.

50
Was t/o to 2ef on 18/12/2013 Under neurosurgical and ent reviews He was well, on regular physiotheraphy and bed rest On regular tracheostomy suction Tracheostomy off on 6/1/2014 He was able to walk without aided Discharged home 7/1/2014with tca ent and neurosurgical Hpe result still pending

Similar presentations