Download presentation
Presentation is loading. Please wait.

1
SURGICAL MANAGEMENT OF DIALYSIS ACCESS STEVE WORATYLA, MD SURGICAL SPECIALISTS OF LANCASTER

2
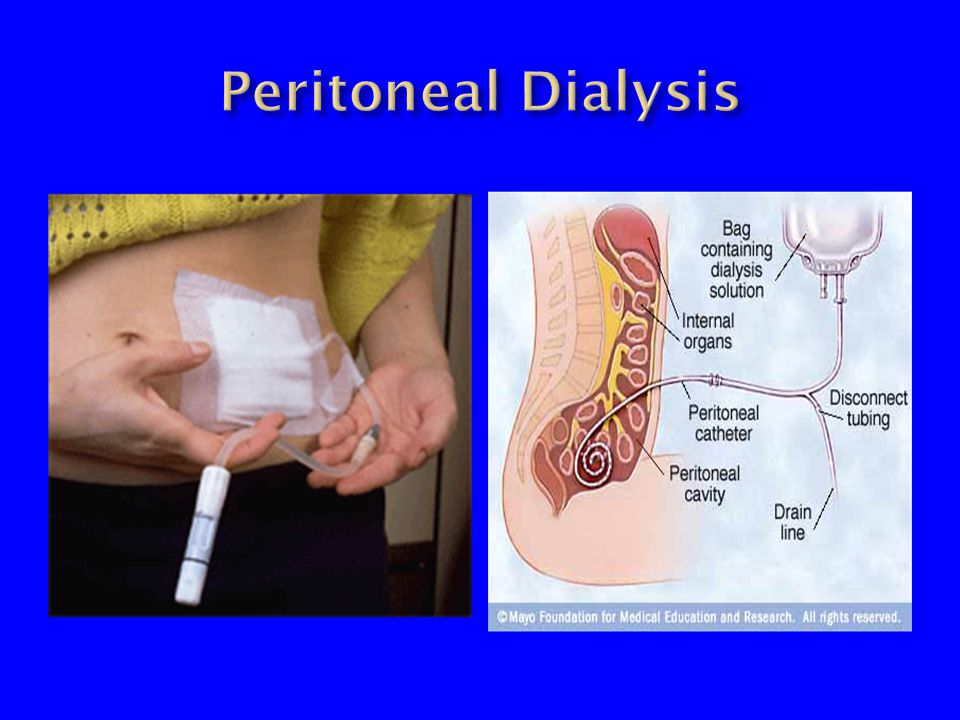
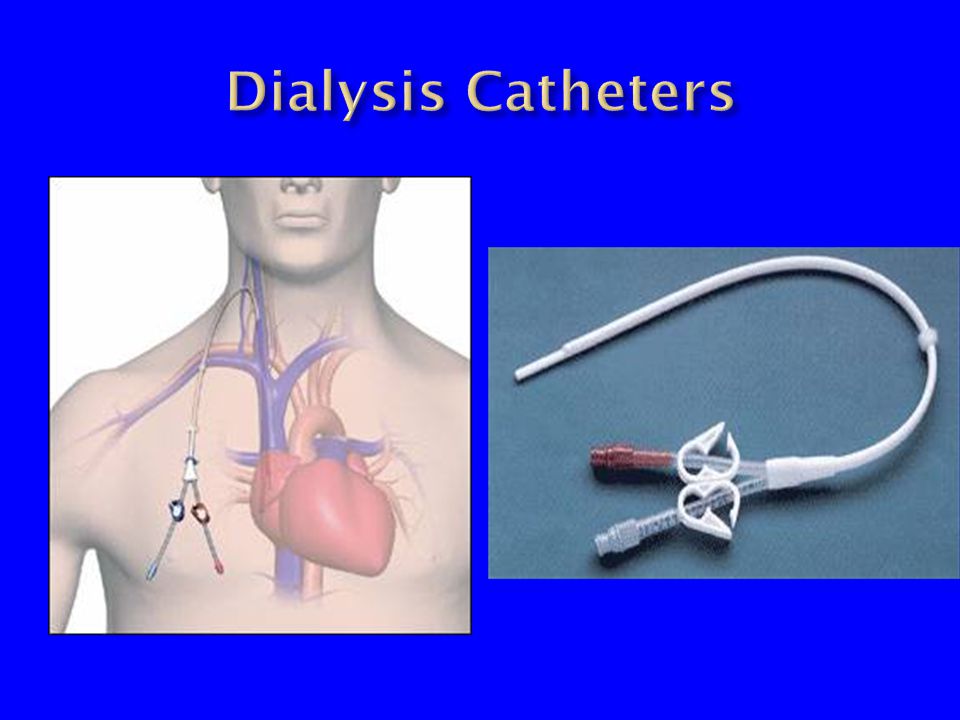
1. CENTRAL VENOUS CATHETERS TEMPORARY TUNNELLED (CUFFED) 2 ARTERIAL VENOUS GRAFTS PROSTHETIC PTFE (GORTEX) VECTRA (immediate access) HeRO graft BIOPROSTHESIS BOVINE CAROTID ARTERY 3. ARTERIAL VENOUS FISTULAS 4. PERITONEAL CATHETERS
 2 ARTERIAL VENOUS GRAFTS PROSTHETIC PTFE (GORTEX) VECTRA (immediate access) HeRO graft BIOPROSTHESIS BOVINE CAROTID ARTERY 3. ARTERIAL VENOUS FISTULAS 4. PERITONEAL CATHETERS.")
5
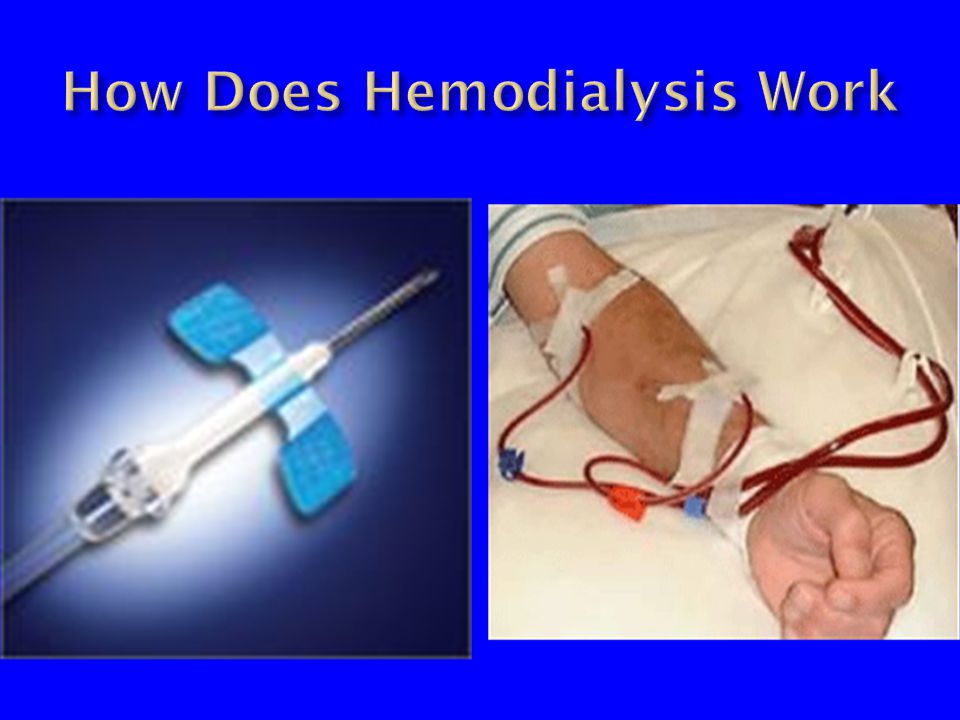
Historical Background Era of modern dialysis began in the 1960’s with the creation of the radio-cephalic av fistula

6
Use best vein and best artery available Usually upper extremity (vein map preop) Cephalic vein and Basilic vein Radial artery and Brachial artery Start distal and work proximal in the arm Requires 6-8 weeks for maturation Allows vein to dilate and thicken 80-85% success rate (supports dialysis) May be improved with aggressive followup program Physical exam, ultrasound, Fistulogram
 Cephalic vein and Basilic vein Radial artery and Brachial artery Start distal and work proximal in the arm Requires 6-8 weeks for maturation Allows vein to dilate and thicken 80-85% success rate (supports dialysis) May be improved with aggressive followup program Physical exam, ultrasound, Fistulogram")
9
Lower cost Lower morbidity Lower mortality

10
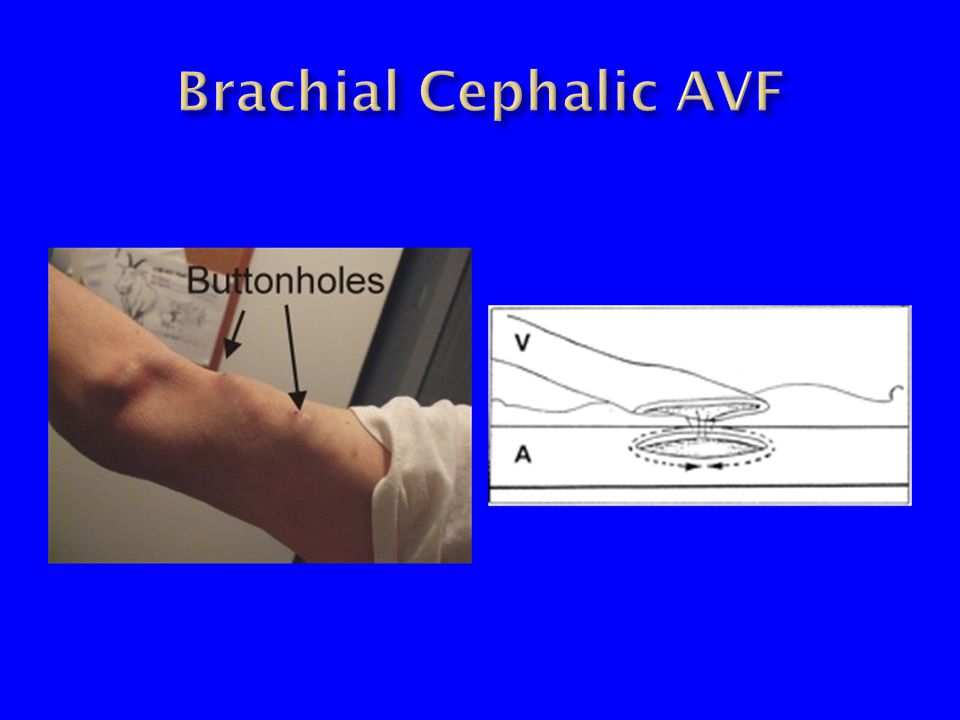
Nomenclature : Artery-Vein Radial-Cephalic Radial-Basilic Brachial-Cephalic Brachial-Basilic Brachial-Brachial Transposing Vein to more superficial and accessible location Basilic Veins Deep Veins

17
Brachial artery to antecubital vein Forearm loop graft Radial artery to antecubital vein Brachial artery to Axillary vein Axillary artery to Axillary vein

23
Thrombosis Stenosis Pseudoaneurysm Infiltration Infection Bleeding Poor maturation Tortuosity Depth of AVF Steal syndrome

28
Autologous AV Fistula is best Requires good communication and planning between Nephrologist, Patient, and Surgeon Peritoneal dialysis catheter is viable alternative to hemodialysis in most patients Requires more active patient involvement Avoid CVC’s and PICC’s Central venous stenosis is achilles heel of upper extremity AV access

Similar presentations


























 PTFE hemodialysis graft in her right upper arm.>")







