Download presentation
Presentation is loading. Please wait.

1
Ramona Bhatia, MD

2
Tuberculosis (TB) ◦ Epidemiology ◦ Diagnostics and treatment ◦ Prevention and student health issues Malaria ◦ Epidemiology ◦ Diagnostics and treatment ◦ Prophylaxis for travelling students Human immunodeficiency virus (HIV) ◦ Epidemiology ◦ Diagnosis and treatment ◦ Needlesticks and post-exposure prophylaxis (PEP)
 ◦ Epidemiology ◦ Diagnostics and treatment ◦ Prevention and student health issues Malaria ◦ Epidemiology ◦ Diagnostics and treatment ◦ Prophylaxis for travelling students Human immunodeficiency virus (HIV) ◦ Epidemiology ◦ Diagnosis and treatment ◦ Needlesticks and post-exposure prophylaxis (PEP)")
3
Undergraduate and medical training at Northwestern ◦ Clinical experience in India Residency at Baylor College of Medicine, Houston, TX ◦ County and VA hospital settings Fellowship in Infectious Diseases at Northwestern ◦ HIV outcomes ◦ HIV and global health Research Associate and Clinical Instructor

4
8.7 million new cases ◦ 13% in HIV-infected (HIV+) patients ◦ India/China->40% ◦ Africa (South Africa>Nigeria)-> 24% ◦ Americas-> 3% 1.4 million TB-related deaths ◦ 990,000 in HIV-uninfected (HIV-) ◦ 430,000 in HIV+ ◦ One of the top three causes of death for adult females in resource-limited settings (RLS)
 patients ◦ India/China->40% ◦ Africa (South Africa>Nigeria)-> 24% ◦ Americas-> 3% 1.4 million TB-related deaths ◦ 990,000 in HIV-uninfected (HIV-) ◦ 430,000 in HIV+ ◦ One of the top three causes of death for adult females in resource-limited settings (RLS)")
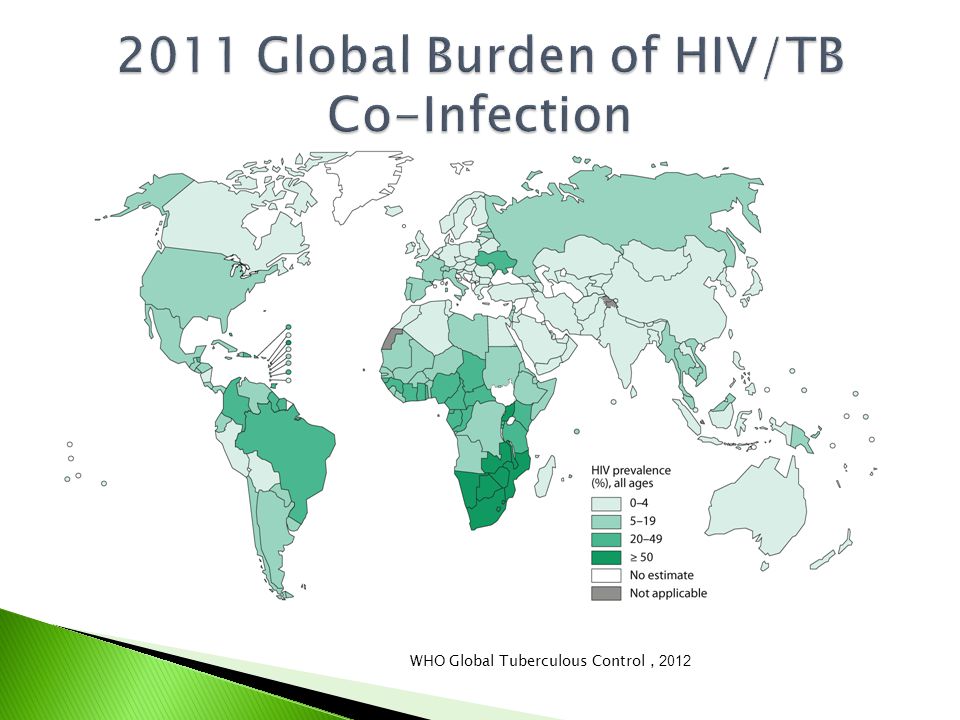
5
WHO Global Tuberculous Control, 2012

7
After inhalation, TB may symptomatically infect the lower lobes of the lung (primary TB infection) Or, the bacteria are contained in upper lobes by macrophages and cell-mediated immune responses (latent TB infection, LTBI) ◦ Can progress to symptomatic disease later (reactivation or “active” TB) Other patients may completely clear the organism
 Or, the bacteria are contained in upper lobes by macrophages and cell-mediated immune responses (latent TB infection, LTBI) ◦ Can progress to symptomatic disease later (reactivation or active TB) Other patients may completely clear the organism")
8
Lifetime risk of reactivating TB is 10% in those with LTBI ◦ 5% in the first two years ◦ 5% thereafter In untreated HIV+ patients, the risk is 7-10% per year ◦ HIV is the strongest predictor of progression Other immune compromising conditions associated with reactivation: ◦ Diabetes ◦ TNF-α inhibitor use ◦ Steroid use

9
www.cdc.gov

10
WHO Symptoms Screen ◦ Absence of all of: cough, weight loss, fever, night sweats ◦ Commonly used in HIV+ patients Tuberculin skin test (TST) ◦ Look for induration (10 mm in med students, 5 mm in HIV+) after 48-72 hours ◦ A positive test indicates prior exposure ◦ Not always positive in active TB ◦ Recommended in RLS Interferon-γ Release Assay (IGRA) ◦ Looks for in-vitro reaction ◦ A positive test indicates prior exposure ◦ Not always positive in active TB ◦ Not recommended in RLS
 ◦ Look for induration (10 mm in med students, 5 mm in HIV+) after hours ◦ A positive test indicates prior exposure ◦ Not always positive in active TB ◦ Recommended in RLS Interferon-γ Release Assay (IGRA) ◦ Looks for in-vitro reaction ◦ A positive test indicates prior exposure ◦ Not always positive in active TB ◦ Not recommended in RLS")
11
Acid-fast staining of sputum ◦ Analyze 3 early morning samples ◦ Most common method in RLS Mycobacterium tuberculosis culture ◦ May not be widely available in RLS Molecular techniques (i.e., PCR) ◦ Uncommon in RLS ◦ Point of care tests are available (GeneXpert) Chest X-Rays ◦ Uncommon in RLS Univ. S. Carolina School of Medicine

12
Preferred regimen has been 9 months of daily isoniazid (INH) Other regimens ◦ 4 months of daily rifampin (RIF) ◦ 3 months of weekly, directly-observed INH plus rifapentine
 Other regimens ◦ 4 months of daily rifampin (RIF) ◦ 3 months of weekly, directly-observed INH plus rifapentine")
13
First-line treatment-> RIPE ◦ Early intensive phase: 2 months of RIF, INH, pyrazinamide (PZA), and ethambutol (ETH) ◦ Continuation phase: 4 months of RIF and INH Monitor monthly for liver toxicity ◦ Usually from INH>RIF>PZA ◦ In RLS, use the physical examination (scleral icterus, jaundice, and hepatomegaly) ◦ Liver function testing is not widely used Other side effects: rash, GI disturbance, ocular toxicity, and neuropathy
, and ethambutol (ETH) ◦ Continuation phase: 4 months of RIF and INH Monitor monthly for liver toxicity ◦ Usually from INH>RIF>PZA ◦ In RLS, use the physical examination (scleral icterus, jaundice, and hepatomegaly) ◦ Liver function testing is not widely used Other side effects: rash, GI disturbance, ocular toxicity, and neuropathy")
14
MDR-TB: INH and RIF resistant XDR-TB: MDR-TB isolates that are also resistant to an injectable (i.e., aminoglycoside) and a quinolone They have been found in all regions ◦ MDR-TB: 3.7% of new TB ◦ High prevalence in Eastern Europe Longer treatment (20 months) with more side effects Higher mortality
 and a quinolone They have been found in all regions ◦ MDR-TB: 3.7% of new TB ◦ High prevalence in Eastern Europe Longer treatment (20 months) with more side effects Higher mortality")
15
WHO Global Tuberculous Control, 2012

17
In one study of American students travelling to Kenya, risk of converting the TST was 4.1% There was no association with duration of stay or participation in direct medical care Only 27% of students reported “ideal” TB prevention measures and monitoring

18
Vaccine? ◦ No. The BCG vaccine is used abroad to prevent childhood TB. It is not available in the U.S. Medical prophylaxis? ◦ No medications are available for TB prophylaxis Best approach involves limiting exposure and monitoring for disease

19
Current international guidelines recommend triage and isolation of patients suspected to have active TB, but space and resource limitations may preclude this ◦ Especially critical to isolate from HIV+ patients Negative pressure rooms are uncommon ◦ Guidelines recommend natural (i.e., opening windows) or mechanical (i.e., fans arranged to blow air out of room) ventilation
 or mechanical (i.e., fans arranged to blow air out of room) ventilation")
20
Personal respiratory protection is the main option for limiting exposure ◦ Obtain 1box of N95 masks online ◦ Reuse masks ◦ Use when seeing a patient with a positive symptoms screen or who is suspected to have active TB ◦ Share with the host medical team They may not have N95 masks or may only be using them for invasive procedures (i.e., intubations) Students should never be seeing patients with known or suspected MDR-/XDR-TB
 Students should never be seeing patients with known or suspected MDR-/XDR-TB")
21
All student travelers should undergo testing for LTBI with TST or IGRA prior to leaving ◦ Addressed at student health appointment Repeat LTBI testing 8-10 weeks after returning Self-monitor for: ◦ Fever (can occur 2-8 weeks after exposure) ◦ Night sweats ◦ Weight loss ◦ Cough ◦ Others: lymphadenopathy, hemoptysis, pleurisy, etc.
 ◦ Night sweats ◦ Weight loss ◦ Cough ◦ Others: lymphadenopathy, hemoptysis, pleurisy, etc.")
22
216 million cases in 2010 ◦ Large burden of disease (81%) and disease-related mortality (91%) in sub-Saharan Africa ◦ One child dies every minute from malaria in Africa In the U.S., 8,117 travel-related cases reported over last decade ◦ 66% acquired from sub-Saharan Africa ◦ 14% acquired from Asia ◦ 43 fatalities, mostly from Plasmodium falciparum infection acquired in sub-Saharan Africa
 and disease-related mortality (91%) in sub-Saharan Africa ◦ One child dies every minute from malaria in Africa In the U.S., 8,117 travel-related cases reported over last decade ◦ 66% acquired from sub-Saharan Africa ◦ 14% acquired from Asia ◦ 43 fatalities, mostly from Plasmodium falciparum infection acquired in sub-Saharan Africa")
23
This is a general map that does not reflect the within-country variation of malaria endemnicity Transmission depends on survival patterns of the Anopheles vector CDC Yellow Book, 2012

25
Blood-borne transmission after bite of Anopheles mosquito ◦ P. falciparum, ovale, vivax, and malariae ◦ Transmission can occur after needlesticks In high-burden countries, transmission is stable and most develop immunity ◦ Pregnant women, children, HIV+ patients, and visitors continue to be at risk In low-burden countries, transmission is sporadic and immunity may not develop

26
In RLS, patients with fever are commonly empirically treated for malaria ◦ This strategy is associated with overtreatment and development of drug resistance ◦ Other symptoms: conjunctival or palmar pallor ◦ End organ dysfunction (i.e., low urine output, altered mental status) defines “severe malaria” Ideally, obtain blood smears or rapid tests prior to starting therapy ◦ If a patient is unstable, empiric therapy is warranted
 defines severe malaria Ideally, obtain blood smears or rapid tests prior to starting therapy ◦ If a patient is unstable, empiric therapy is warranted")
27
Artemisinin-based combination therapy (ACT) is recommended for uncomplicated P.falciparum malaria ◦ Artemether plus lumefantrine (Coartem) ◦ Artesunate plus amodiaquine ◦ Artesunate plus mefloquine ◦ Artesunate plus sulfadoxine-pyrimethamine ◦ Dihydroartemisinin plus piperaquine ◦ Choice of preferred ACT is country-specific Severe malaria ◦ “ABCs” for the critically ill ◦ Hospitalize and start IV or IM artesunate
 is recommended for uncomplicated P.falciparum malaria ◦ Artemether plus lumefantrine (Coartem) ◦ Artesunate plus amodiaquine ◦ Artesunate plus mefloquine ◦ Artesunate plus sulfadoxine-pyrimethamine ◦ Dihydroartemisinin plus piperaquine ◦ Choice of preferred ACT is country-specific Severe malaria ◦ ABCs for the critically ill ◦ Hospitalize and start IV or IM artesunate")
28
The geographic risk of malaria will be determined at the pre-departure student health appointment Prevention has four elements: ◦ A-awareness of the disease process ◦ B-avoid being bitten with effective vector control ◦ C-chemoprophylaxis adherence ◦ D-diagnosis should infection occur

29
http://www.malariaconsortium.org/ Insecticide-treated nets (ITNs) Long sleeves and pants Insect repellant o DEET (10-50%)
 Long sleeves and pants Insect repellant o DEET (10-50%)")
30
Atovaquone-proguanil (Malarone) ◦ Daily dosing ◦ Start 1-2 days prior to leaving; continue for 1 week after returning ◦ Overall well tolerated ◦ Contraindicated in severe renal failure Mefloquine ◦ Serious CNS side effects can occur Chloroquine, hydroxychloroquine ◦ Not used due to high rates of resistance Doxycycline ◦ Sun sensitivity
 ◦ Daily dosing ◦ Start 1-2 days prior to leaving; continue for 1 week after returning ◦ Overall well tolerated ◦ Contraindicated in severe renal failure Mefloquine ◦ Serious CNS side effects can occur Chloroquine, hydroxychloroquine ◦ Not used due to high rates of resistance Doxycycline ◦ Sun sensitivity")
31
Watch for fever Incubation is 1 week, so fever immediately after exposure to an endemic area is unlikely malaria If symptoms occur, seek medical care ◦ List of reputable clinics in your area will be provided to you ◦ DO NOT use medications from marketplaces (high rates of ineffective, expired, and unregulated meds)
")
32
34 million people living with HIV/AIDS (PLWHA) ◦ 2.2 million in North America/Europe ◦ 22.9 million in sub-Saharan Africa (5.6 million in South Africa) 2.7 million new infections ◦ 88,000 in North America/Europe ◦ 1.9 million in sub-Saharan Africa 1.8 million deaths due to HIV/AIDS ◦ 30, 000 in North America/Europe ◦ 1.2 million in sub-Saharan Africa
 ◦ 2.2 million in North America/Europe ◦ 22.9 million in sub-Saharan Africa (5.6 million in South Africa) 2.7 million new infections ◦ 88,000 in North America/Europe ◦ 1.9 million in sub-Saharan Africa 1.8 million deaths due to HIV/AIDS ◦ 30, 000 in North America/Europe ◦ 1.2 million in sub-Saharan Africa")
33
CDC Yellow Book, 2012

34
HIV infects CD4+ T-lymphocytes (CD4 cells) Transmitted through sexual fluids, breastmilk, or blood ◦ Possible transmission through oral sex but rare ◦ No transmission from kissing or close contact ◦ No transmission from fomites
 Transmitted through sexual fluids, breastmilk, or blood ◦ Possible transmission through oral sex but rare ◦ No transmission from kissing or close contact ◦ No transmission from fomites")
35
In acute infection, flu-like syndrome with rash, lymphadenopathy, and/or meningitis Or can be completely asymptomatic In chronically infection, symptoms are often from opportunistic infections (OI)
")
36
TB is the most common OI in HIV+ patients ◦ Occurs at any CD4 count ◦ One-third of HIV+ patients also have LTBI TB is the most common cause of death in HIV/AIDS patients in Africa and a leading cause globally ◦ 350,000 deaths yearly worldwide All patients with TB should be tested for HIV; all patients with HIV should be screened for TB

37
All HIV+ patients should undergo symptom screening for TB and (if negative) receive INH preventative therapy (IPT) ◦ In RLS, PPD, IGRA, and CXR not routinely used Presentation of active TB depends on CD4 count. In general: ◦ Immunocompetent (CD4>300/µl): pulmonary TB, cavities, granulomas ◦ Immunosuppressed (CD4<300/µl): extra-pulmonary TB (virtually anywhere including blood, lymph nodes, GI tract, CNS), atypical/normal CXR, +/-granulomas
: pulmonary TB, cavities, granulomas ◦ Immunosuppressed (CD4<300/µl): extra-pulmonary TB (virtually anywhere including blood, lymph nodes, GI tract, CNS), atypical/normal CXR, +/-granulomas.")
38
India Ink, www.stanford.edu Occurs at CD4 count <50/µl Subacute mental status changes, headache, fever common CSF may be normal In RLS, may treat with fluconazole Amphotericin may not be available

39
Occurs at CD4 count<100/µl Focal neurologic signs, fever, headache common Ring-enhancing lesions Treat with pyrimethamine plus sulfadiazine plus leucovorin (folinic acid) ◦ Some RLS may utilize sulfadoxine instead of sulfadiazine www.radiopaedia.com
 ◦ Some RLS may utilize sulfadoxine instead of sulfadiazine")
40
In U.S., common screening test is ELISA ◦ High sensitivity In RLS, rapid serologic HIV testing more common for screening Confirmatory test for both is Western Blot ◦ High specificity In suspected cases of acute HIV, obtain HIV viral load ◦ The other tests may be negative ◦ HIV viral load may not be available in all RLS

41
U.S. (AIDSinfo)RLS (WHO) Indication?All HIV+ patientsCD4<350/µl or stage 3 or 4 (i.e., presence of OI) What to initiate?Several regimens are first-line; more being added Only zidovudine, lamivudine, emtricitibine, tenofovir, efavirenz, nevirapine first-line How to monitor?CD4 count, viral load, clinical assessment CD4 count and clinical assessment (viral load only if available) Pregnant women?All women (lifelong treatment) All women (lifelong or pregnancy-only treatment)
RLS (WHO) Indication All HIV+ patientsCD4<350/µl or stage 3 or 4 (i.e., presence of OI) What to initiate Several regimens are first-line; more being added Only zidovudine, lamivudine, emtricitibine, tenofovir, efavirenz, nevirapine first-line How to monitor CD4 count, viral load, clinical assessment CD4 count and clinical assessment (viral load only if available) Pregnant women All women (lifelong treatment) All women (lifelong or pregnancy-only treatment).")
42
Know what defines a high-risk exposure: An exposure that might place HCP at risk for HBV, HCV, or HIV infection is defined as a percutaneous injury (e.g., a needlestick or cut with a sharp object) or contact of mucous membrane or nonintact skin (e.g.,exposed skin that is chapped, abraded, or afflicted with dermatitis) with blood, tissue, or other body fluids Potentially infectious : blood, CSF, synovial fluid, pleural fluid, pericardial fluid, amniotic fluid, semen, vaginal secretions Not infectious: feces, nasal secretions, saliva, sputum, sweat, tears, urine, and vomit, as long as these are not visibly contaminated with blood
 or contact of mucous membrane or nonintact skin (e.g.,exposed skin that is chapped, abraded, or afflicted with dermatitis) with blood, tissue, or other body fluids Potentially infectious : blood, CSF, synovial fluid, pleural fluid, pericardial fluid, amniotic fluid, semen, vaginal secretions Not infectious: feces, nasal secretions, saliva, sputum, sweat, tears, urine, and vomit, as long as these are not visibly contaminated with blood")
43
Avoidable high-risk behaviors: ◦ Tattoos, piercings, acupuncture ◦ Sexual activity ◦ Drug use Use standard precautions if using sharps Needlestick risks of infection: ◦ HIV: 0.3% (approx. 1000 cases/year) ◦ Hepatitis C: 3.0% ◦ Hepatitis B: 30%
 ◦ Hepatitis C: 3.0% ◦ Hepatitis B: 30%.")
44
Immediately flush area with soap and water Obtain source source rapid HIV test and hepatitis B and C serologies ◦ The hepatitis testing may not be readily available Exposed student should know his/her baseline serologies ◦ All med students should have received hepatitis B vaccine with follow-up HepBSAb pre-departure ◦ Pre-departure HIV testing encouraged ◦ HIV, hepatitis B, and hepatitis C serologic testing should be performed after exposure Report exposure to attending/supervisor and Northwestern contact (Dan Young, Dr. Thomas, Dr. Sanguino)-but should not delay testing or PEP!
-but should not delay testing or PEP!.")
45
Hepatitis B ◦ If student HepBSAb positive (i.e., >100IU/L), no action needed ◦ If student HepBSab negative or unknown, administer hepatitis B vaccine and HBIG (immunoglobulin) within 24 hours and repeat serologies at 1 and 3 months Hepatitis C ◦ In addition to baseline student testing, obtain repeat serology at 1, 3, and 6 months ◦ OR obtain PCR at 4-6 weeks ◦ No recommended PEP
, no action needed ◦ If student HepBSab negative or unknown, administer hepatitis B vaccine and HBIG (immunoglobulin) within 24 hours and repeat serologies at 1 and 3 months Hepatitis C ◦ In addition to baseline student testing, obtain repeat serology at 1, 3, and 6 months ◦ OR obtain PCR at 4-6 weeks ◦ No recommended PEP")
46
Initiate PEP ASAP if source is HIV+, HIV unknown, or may be in the window period with false-negative rapid testing ◦ MUST BE within 72 hours but do not wait this long! Many host hospitals have PEP on hand ◦ ASK about PEP policies on the first day of work! Monitor for side effects: diarrhea common ◦ Fevers, rashes, intolerable GI side effects need to be further evaluated PEP duration 28 days… Adherence is crucial! Follow-up testing at 1, 3, and 6 months

47
After needlestick, student should self- monitor for symptoms ◦ Flu-like illness ◦ Lymphadenopathy ◦ Abdominal pain or jaundice Student can continue to work in the hospital Student should refrain from donating blood or unprotected sexual activity for 6 months On returning home, student will see an ID physician for repeat serologies as needed and PEP monitoring

48
You are rotating on the general medicine ward in a hospital in Cape Town, South Africa. You are asked to help out a friend who is doing a lumbar puncture on a cachectic patient with altered mental status of unknown etiology. Your friend is startled, and the needle punctures through his glove and into his skin. You are not wearing goggles, and the fluid gets into your eyes.

49
Has there been a high-risk exposure? What is the very first thing that should be done? What should be done next? How could this have been prevented?

50
There is a large burden of TB, malaria, and HIV in RLS The management of these infections may be different in RLS Students should engage in prevention strategies to protect themselves from these infections Host attendings/supervisors and Northwestern Global Health contacts are available for any concerns during travel

51
Infectious Diseases Clinic ◦ Drs. Murphy, Galvin, Achenbach, Bhatia ◦ 312-695-8358 Travel Clinic ◦ Dr. Lee ◦ 312 926-3155

53
WHO recommended IC practices: 1.Triage pt with TB –depends on region 2.Isolate TB pts ESP from HIV pts 3.Cough etiquitte for TB pts (unknown if a mask on them helps) 4.Natural and mechanical ventilation (fans) In particular, health workers should use particulate respirators: during high-risk aerosol-generating procedures associated with high risk of TB transmission (e.g. bronchoscopy, intubation, sputum induction procedures, aspiration of respiratory secretions, and autopsy or lung surgery with highspeed devices) when providing care to infectious MDR-TB and XDR-TB patients or people suspected of having infectious MDR-TB and XDR-TB. http://whqlibdoc.who.int/publications/2009/9789241598323_eng. pdf
 when providing care to infectious MDR-TB and XDR-TB patients or people suspected of having infectious MDR-TB and XDR-TB. pdf.")
54
People working internationally who will be engaging in high-risk occupational health care activities, such as drawing blood or the other use of sharps during patient care, should consistently follow standard precautions to reduce the risk of occupational exposure to HIV and other bloodborne pathogens. Standard precautions involve the use of protective barriers such as gloves, gowns, aprons, masks, or protective eyewear. Additional information about occupational health and safety standards for bloodborne pathogens can be found at http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=10051http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=10051 In addition, clinicians working internationally should: Always be mindful of the hazards posed by sharps injuries. Maintain strict safety standards while working in environments that may have less stringent standards. Use devices with safety features and improved work practices (www.cdc.gov/niosh/docs/2000-108/).www.cdc.gov/niosh/docs/2000-108/ Consider bringing their own protective equipment if they are unsure of its availability at their destination. Consider bringing postexposure prophylaxis (PEP) for HIV in the event that they are injured with a potentially contaminated sharp. POSTEXPOSURE MANAGEMENT Health care workers who may have been occupationally exposed to HIV should immediately perform the following steps: Wash the exposed area with soap and water thoroughly. If mucous membrane exposure has occurred, flush the area with copious amounts of water or saline. If possible, assess the HIV status of the source. Rapid HIV testing is preferred. If the source’s rapid HIV antibody test result is positive, assume that it is a true positive. Seek qualified medical evaluation as soon as possible to guide decisions on postexposure treatment and testing. Contact the National Clinicians’ Postexposure Prophylaxis Hotline (PEPline) at 1-888-448-4911 (24 hours a day, 7 days per week) for assistance in assessing risk and advice on managing occupational exposures to HIV and other bloodborne pathogens (www.nccc.ucsf.edu/about_nccc/pepline). If the toll-free number is not accessible when calling from another country, the main administrative line for the National HIV/AIDS Clinicians’ Consultation Center is 415-206-8700.www.nccc.ucsf.edu/about_nccc/pepline Consider beginning PEP for HIV (see below). Postexposure Prophylaxis A number of medication combinations are available for PEP. Since these regimens may change based on new research, refer to MMWR’s Updated US Public Health Service Guidelines for the Management of Occupational Exposures to HIV and Recommendations for Postexposure Prophylaxis (http://aidsinfo.nih.gov/Guidelines/GuidelineDetail.aspx?MenuItem=Guidelines&Search=Off&GuidelineID=10&ClassID=3) and the PEPline for more information about PEP recommendations. Specific regimens should be determined by clinicians familiar with the medications and the health care worker’s medical history.http://aidsinfo.nih.gov/Guidelines/GuidelineDetail.aspx?MenuItem=Guidelines&Search=Off&GuidelineID=10&ClassID=3 If the exposed person chooses to initiate PEP, he or she must do so within hours of the exposure. PEP can be stopped if new information changes the assessment; however, waiting to start PEP until all information is gathered can decrease its efficacy. If indicated, arrange for procurement or shipment of additional PEP from a credible source to complete the recommended 4-week course of treatment. Consider other potential infectious disease exposures from the source material, including hepatitis B virus or hepatitis C virus (HCV), and manage as appropriate. Postexposure Testing People with occupational exposure to HIV should receive HIV antibody testing by enzyme immunoassay as soon as possible after exposure as a baseline, with follow-up testing at 6 weeks, 3 months, and 6 months. Extended HIV follow-up testing for up to 12 months is recommended for those who become infected with HCV after exposure to a source coinfected with HIV and HCV. Postexposure counseling and medical evaluation should be provided, whether or not the exposed person receives PEP (http://aidsinfo.nih.gov/contentfiles/Health CareOccupExpoGL_PDA.pdf ).http://aidsinfo.nih.gov/contentfiles/Health CareOccupExpoGL_PDA.pdf Exposed health care workers should be advised to use precautions (avoid blood or tissue donations, breastfeeding, or pregnancy) to prevent secondary transmission, especially during the first 6–12 weeks after exposure. For exposures for which PEP is indicated, exposed people should be counseled regarding possible drug toxicities and interactions, the need for monitoring, and the importance of careful adherence to PEP regimens. Cdc yellow book 2012
 for HIV in the event that they are injured with a potentially contaminated sharp. POSTEXPOSURE MANAGEMENT Health care workers who may have been occupationally exposed to HIV should immediately perform the following steps: Wash the exposed area with soap and water thoroughly. If mucous membrane exposure has occurred, flush the area with copious amounts of water or saline. If possible, assess the HIV status of the source. Rapid HIV testing is preferred. If the source’s rapid HIV antibody test result is positive, assume that it is a true positive. Seek qualified medical evaluation as soon as possible to guide decisions on postexposure treatment and testing. Contact the National Clinicians’ Postexposure Prophylaxis Hotline (PEPline) at (24 hours a day, 7 days per week) for assistance in assessing risk and advice on managing occupational exposures to HIV and other bloodborne pathogens ( If the toll-free number is not accessible when calling from another country, the main administrative line for the National HIV/AIDS Clinicians’ Consultation Center is Consider beginning PEP for HIV (see below). Postexposure Prophylaxis A number of medication combinations are available for PEP. Since these regimens may change based on new research, refer to MMWR’s Updated US Public Health Service Guidelines for the Management of Occupational Exposures to HIV and Recommendations for Postexposure Prophylaxis ( MenuItem=Guidelines&Search=Off&GuidelineID=10&ClassID=3) and the PEPline for more information about PEP recommendations. Specific regimens should be determined by clinicians familiar with the medications and the health care worker’s medical history. MenuItem=Guidelines&Search=Off&GuidelineID=10&ClassID=3 If the exposed person chooses to initiate PEP, he or she must do so within hours of the exposure. PEP can be stopped if new information changes the assessment; however, waiting to start PEP until all information is gathered can decrease its efficacy. If indicated, arrange for procurement or shipment of additional PEP from a credible source to complete the recommended 4-week course of treatment. Consider other potential infectious disease exposures from the source material, including hepatitis B virus or hepatitis C virus (HCV), and manage as appropriate. Postexposure Testing People with occupational exposure to HIV should receive HIV antibody testing by enzyme immunoassay as soon as possible after exposure as a baseline, with follow-up testing at 6 weeks, 3 months, and 6 months. Extended HIV follow-up testing for up to 12 months is recommended for those who become infected with HCV after exposure to a source coinfected with HIV and HCV. Postexposure counseling and medical evaluation should be provided, whether or not the exposed person receives PEP ( CareOccupExpoGL_PDA.pdf ). CareOccupExpoGL_PDA.pdf Exposed health care workers should be advised to use precautions (avoid blood or tissue donations, breastfeeding, or pregnancy) to prevent secondary transmission, especially during the first 6–12 weeks after exposure. For exposures for which PEP is indicated, exposed people should be counseled regarding possible drug toxicities and interactions, the need for monitoring, and the importance of careful adherence to PEP regimens. Cdc yellow book")
Similar presentations





















 Training BLOOD BORNE PATHOGENS 2/26/2014.>")
