Download presentation
Presentation is loading. Please wait.

1
가톨릭대학교 인천성모병원 재활의학과 김재민 근골격계 질환에서 비만의 영향

2
비만과 근골격계 질환 Chronic musculoskeletal conditions Disability Decreased health-related quality of life Increased Health-care costs

3
Case 54/M C/C 허리와 무릎이 아파요. 전신이 다 불편해요. –6 months ago –VAS 6 PHx –DM/HTN/Hyperlipidemia (+/+/-) 신장 162, 체중 110, BMI 41.9
 신장 162, 체중 110, BMI")
4
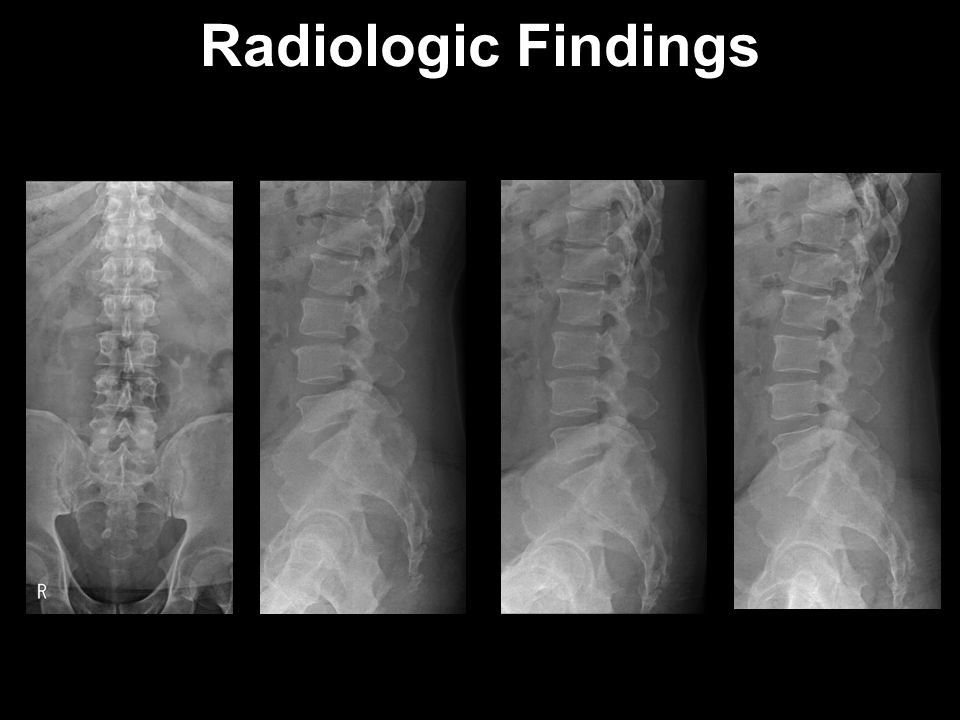
Radiologic Findings

7
Prognosis 1.Knee OA 2.Degenerative Spine c degenerative disc disease 3.Polyarthritis 4.Shoulder rotator cuff tendinopathy 5.Obesity Medication Exercise Injection Body weight

8
비만과 근골격계 질환

9
Musculoskeletal Pain Abnormal movement patterns –Antalgic gait –Postural dysfunction –Increased thoracolumbar stiffness –Decreased proprioception –Altered activation of abdominal and extensor muscles Joint or structural damage Muscle strength deterioration Systemic inflammation Psychosocial problem

10
Case 58/F C/C both knee pain –6 months ago –VAS 5 PHx –DM/HTN/Hyperlipidemia (+/+/+) 신장 152, 체중 85, BMI 36.8
 신장 152, 체중 85, BMI 36.8")
11
Radiologic Findings

12
Pain Control –NSAID –Intraarticular injection –Physical modality Patient education –Body weight control Rehabilitation Treatment

13
Osteoarthritis More than 31% of obese adults >> 16% of non-obese people The odds ratio (OR) per 5-U BMI increase was 1.6 Knee osteoarthritis Hip osteoarthritis Hand osteoarthritis
 per 5-U BMI increase was 1.6 Knee osteoarthritis Hip osteoarthritis Hand osteoarthritis")
14
Knee Osteoarthritis Metabolic factor –Worsens truncal obesity Presence of chronic pain may stimulate release of cortisol –Visceral fat produces numerous substances including derived proinflammatory and insulin resistance–inducing molecules Mechanical factor –Increased axial forces –Varus malalignment –Muscle strength deficits exist in obese persons

15
Physiological Forces

16
Knee Osteoarthritis

17
Goal of Management of OA Control pain and swelling Maintain and/or improve joint mobility Minimize functional impairment Improve the quality of life

18
Non-pharmacologic therapy –Lose weight –Exercise –Education –Orthosis –Physical modality –Acupuncture Pharmacologic therapy –Acetaminophen –NSAID –Opioid –Nutritional supplement Management of Knee OA Intra-articular injection –Corticosteroid –Hyaluronates –Platelet-rich plasma

19
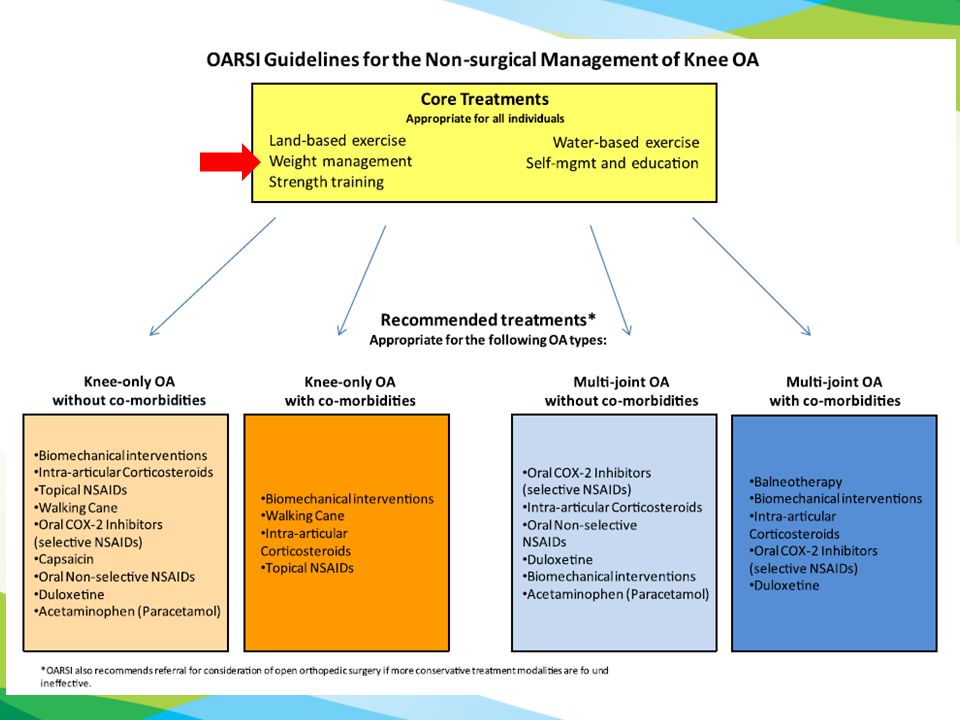
Clinical Practice Guideline 2012 Arthritis Care & Research Vol. 64, No. 4, pp 465–474 2014 Osteoarthritis Cartilage 22(3): 363-88. 2013 Journal of the American Academy of Orthopaedic Surgeons 21(9): 571-576. 2010 J Korean Knee Soc, Vol. 22, No. 1, March 2013 Ann Rheum Dis 72(7): 1125-35
: Journal of the American Academy of Orthopaedic Surgeons 21(9): J Korean Knee Soc, Vol. 22, No. 1, March 2013 Ann Rheum Dis 72(7):")
21
Lose Weight OARSI: Appropriate AAOS: moderate recommendation EULAR: Ia ACR: Strongly recommended AAOS: Patients with symptomatic OA of the knee –Overweight (as defined by a BMI>25) –Lose weight (a minimum of five percent (5%) of body weight) –Maintain their weight at a lower level with an appropriate program of dietary modification and exercise.
 –Lose weight (a minimum of five percent (5%) of body weight) –Maintain their weight at a lower level with an appropriate program of dietary modification and exercise.")
22
Exercise Aerobic exercise Strengthening exercise Balance exercise ROM/flexibility exercise Manual therapy

23
Aerobic Exercise Aquatic exercise program –Aerobic deconditioned patients Regular aerobic exercise Low-impact aerobic fitness exercise OARSI: Appropriate AAOS: Strong recommendation EULAR: Ia ACR: Strongly recommended

24
Strengthening Exercise Quadriceps strengthening Relief of pain and improvement in function OARSI: Appropriate AAOS: Strong recommendation EULAR: Ia ACR: Strongly recommended (with aerobic exercise)
")
25
Exercise Balance exercise –No recommendation by ACR ROM/flexibility exercise –AAOS LoE(V), Grade of recommendation (C) Manual therapy –Supervised by a physical therapist: conditionally recommend by ACR
, Grade of recommendation (C) Manual therapy –Supervised by a physical therapist: conditionally recommend by ACR")
26
Patients Education Education of patient’s family, friends, or caregivers Education material (videos, pamphlets, news letters) Self-management of educational program OARSI: Appropriate AAOS: Strong recommendation EULAR: Ia ACR: Conditionally recommended
 Self-management of educational program OARSI: Appropriate AAOS: Strong recommendation EULAR: Ia ACR: Conditionally recommended")
27
Patients Education Self-management program –Conditional recommend by ACR Tai chi program ( 태극권 ) –Conditional recommend by ACR Regular contact –AAOS LoE (IV), Grade (C) –Personalized social support through telephone contact
 –Conditional recommend by ACR Regular contact –AAOS LoE (IV), Grade (C) –Personalized social support through telephone contact")
28
Osteoarthritis Hip osteoarthritis –Bilateral hip OA > unilateral hip OA –The odds ratio (OR): 2 Hand osteoarthritis –BMI was found to be directly proportional to the prevalence of thumb carpo-metacarpal OA in both sexes –The adjusted OR was 1.29 per 5 kgm2 increment in BMI.
: 2 Hand osteoarthritis –BMI was found to be directly proportional to the prevalence of thumb carpo-metacarpal OA in both sexes –The adjusted OR was 1.29 per 5 kgm2 increment in BMI.")
29
CASE 33/F C/C LBP with right leg radiating pain –3 months ago –VAS 5-6 PHx –DM/HTN/Hyperlipidemia (-/-/-) –Previous LBP 3yrs ago 신장 162, 체중 75, BMI 28.6
 –Previous LBP 3yrs ago 신장 162, 체중 75, BMI 28.6")
30
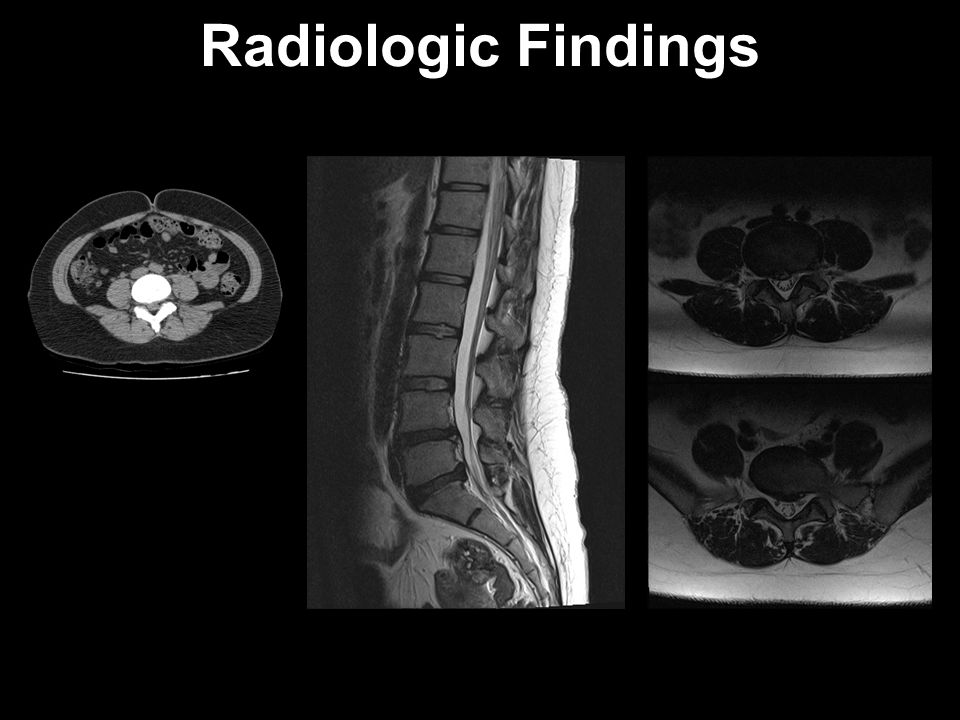
Motor –Intact Sensory –No discrepancy SLR (60/F) Thomas (+/+) Patrick (-/-) Provocation test (+) Neurogenic claudication (-) DTR –Normoactive Pathologic reflex –Barbinski sign(-/-) Physical Examination
 Thomas (+/+) Patrick (-/-) Provocation test (+) Neurogenic claudication (-) DTR –Normoactive Pathologic reflex –Barbinski sign(-/-) Physical Examination")
31
Radiologic Findings

33
Spinal Intervention

34
Core Stabilization Exercise

35
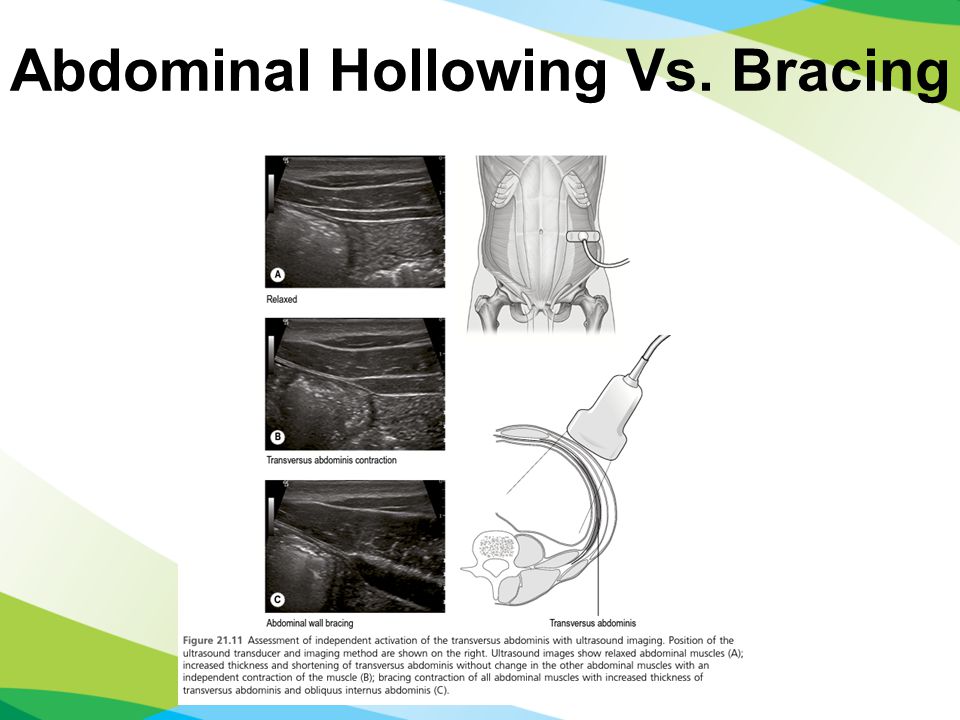
Hodges PW (Australia) Motor control Transverse abdominis Abdominal hollowing McGill S (Canada) Stiffness All of the torso muscles Abdominal bracing Abdominal Hollowing Vs. Bracing

37
Spine Rehabilitation

38
Low Back Pain

39
Obese patients were more likely to have radicular pain and neurologic signs. Obesity was a significant, independent determinant of chronicity in a prospective cohort study in workers claiming compensation for lower back pain. In morbidly obese subjects with lower back pain undergoing bariatric surgery, weight loss significantly improved the degree of functional disability, and resulted in less frequent lower back pain and the use of reduced doses of medications

40
Lumbar Disc Herniation Spine Patient Outcomes Research Trial (SPORT) Rihn, J. A., et al. (2013). J Bone Joint Surg
. J Bone Joint Surg.")
41
Tendinopathy Common musculoskeletal diseases Obesity measured in terms of BMI (BMI ≥ 30 kg/m2) and tendon diseases, with odds ratios ranging from 1.9 (95% CI: 1.1–2.2) to 5.6 (1.9–16.6) Mechanical factor –Stronger association between lower limb tendinopathies and obesity, compared to upper limbs Metabolic factor –Failed healing response Franceschi, F., et al. Int J Endocrinol 2014

42
Achilles Tendinopathy Overloading Long stranding Failed healing response –Alteration of blood flow Metabolic risk factors –Obesity –Diabetes –Hypertension –Use steroid

43
Achilles Tendinopathy

44
Rotator Cuff Tendinopathy Wendelboe et al. in 2004, 311 participants –Individuals with a BMI ≥35.0 had an increased risk to require rotator cuff repair Odd ratio: 3.1 (CI 1.3–7.6) for males Odd ratio: 3.5 (1.8–6.9) for females Titchener et al. in 2013, 5000 patients –Overweight body mass index of 25.1 to 30 (OR = 1.15) was significantly associated with rotator cuff disease –Body mass index greater than 30 was not found to be associated with rotator cuff disease
 for males Odd ratio: 3.5 (1.8–6.9) for females Titchener et al. in 2013, 5000 patients –Overweight body mass index of 25.1 to 30 (OR = 1.15) was significantly associated with rotator cuff disease –Body mass index greater than 30 was not found to be associated with rotator cuff disease.")
45
Rotator Cuff Tendinopathy Rechardt et al. in 2010, 6237 patients –Smoking, waist circumference, and waist-to-hip ratio were related to an increased prevalence of shoulder pain in both men and women. –Metabolic syndrome, type 2 diabetes mellitus, and carotid intima-media thickness were associated with shoulder pain in men, –Increased waist circumference and type 1 diabetes mellitus were associated with chronic rotator cuff tendinitis in men.

46
CASE 51/F C/C 좌측 견관절 통증 및 움직임 제한 –1 months ago –VAS 6 PHx –DM/HTN/Hyperlipidemia (+/+/+) 신장 158, 체중 100, BMI 40.1
 신장 158, 체중 100, BMI 40.1")
47
Physical Examination Neck pain (-) Active ROM Flex/Abd/ER 100/130/30 IR: lower lumbar Passive ROM Flex/Abd/ER 170/170/60 Impingement test: (-/+) Motor : intact Greater tubercle Tenderness (-/+)
 Active ROM Flex/Abd/ER 100/130/30 IR: lower lumbar Passive ROM Flex/Abd/ER 170/170/60 Impingement test: (-/+) Motor : intact Greater tubercle Tenderness (-/+)")
48
Radiologic Findings

49
Treatment Supraspinatus tendinopathy, left Subacromial bursitis, left Pain control Patient education

50
Elbow Tendinopathy Mechanical overloading Abnormal microvascular responses Titchener et al. in 2013, 4998 participants –Obesity is not associated with epicondylitis

51
Elbow Tendinopathy Descatha et al. in 2013, 699 patients –Subjects with BMI >30 kg/m2 had higher incidence rates for the disease (OR: 2.4, CI: 1.2–4.8) –No significant association was instead found for medial epicondylitis Shiri et al. in 2006 4783 patients –Medial epicondylitis in women and both waist circumference >100 cm (OR: 2.7CI: 1.2–6.0) and BMI >30 kg/m2 (OR: 1.9CI: 1.0–2.7), –No increased risk as regards lateral epicondylitis.
 –No significant association was instead found for medial epicondylitis Shiri et al. in patients –Medial epicondylitis in women and both waist circumference >100 cm (OR: 2.7CI: 1.2–6.0) and BMI >30 kg/m2 (OR: 1.9CI: 1.0–2.7), –No increased risk as regards lateral epicondylitis..")
52
Plantar Fasciitis Loss of the transverse foot arch Higher vertical forces under the heel during gait Effect of an increased weight on musculoskeletal disorders of the lower district (feet and ankles), which are known to be caused by overuse and stress, which are factors made worse by weight
, which are known to be caused by overuse and stress, which are factors made worse by weight")
53
Entrapment Neuropathy Meralgia paresthetica –Neuropathy of the lateral femoral cutaneous nerve –MP with BMI odds ratio (OR) 1.2 Carpal tunnel syndrome –Obesity was a significant risk factor associated with carpal tunnel syndrome (OR=2.06).
 1.2 Carpal tunnel syndrome –Obesity was a significant risk factor associated with carpal tunnel syndrome (OR=2.06).")
54
Trochanteric Bursitis Chronic pain overlying the lateral aspect of the hip Prevalence being higher in women, and patients with coexisting low back pain, osteoarthritis, iliotibial band tenderness, and obesity. Williams, B. and S. Cohen (2009) Anesthesia and analgesia
 Anesthesia and analgesia.")
55
Osteoporosis 10 kg increase in body weight is associated with approximately a 1% increase in BMD the effect of weight on BMD appears to be stronger in women than in men Mechanism –Adipose tissue the major site of conversion of androgens to estrogen in both elderly men and women –increased mechanical load

56
Gout Obesity is a well-known modifiable risk factor in the pathogenesis of gout and serum uric acid is positively associated with BMI The size of the visceral fat area is the strongest contributor to elevated serum uric acid concentration, decreased uric acid clearance and increased urinary uric acid/creatinine ratio

58
경청해주셔서 감사합니다.

Similar presentations



 Rogelio A Balagat MD ASMPH.>")



 Femoroacetabular Impingement (FAI) Labral tears Bursitis Tendonitis Conditions we.>")






 is one of the oldest and most common forms of arthritis. Known as the “wear and tear” kind of arthritis.>")






 a joint دکتر علی اصغر مغاری متخصص طب فیزیکی و توانبخشی.>")