Download presentation
Presentation is loading. Please wait.

1
METABOLIC SYNDROME AND VISCERAL OBESITY Nizar ALBACHE University of Aleppo-Diabetes Research Unit President of Syrian of Endocrine Society Vice President of Mediterranean Group for Study of Diabetes( MGSD)
")
2
Metabolic Syndrome Deadly quartet Insulin resistance syndrome Alternate names given to Reaven’s Syndrome Reaven GM. Banting Lecture 1988. Role of insulin resistance in human disease. Diabetes 1988;37:1595-607

3
Three or more of the following five factors : Waist circumference > 102 cm in men > 88 cm in women Plasma triglycerides > 150 mg/dl HDL-C < 40 mg/dl in men <50 mg/dl in women BP > 130/85 mm Hg Plasma glucose > 100 mg/dl Definition of Metabolic Syndrome IDF,ATP III- 2005

4
Disease Risk*BMI (kg/m 2 )Classification 1 --<18.5Underweight --18.5 to 24.9Normal Increased25.0 to 29.9Overweight High30.0 to 34.9IObesity Very High35.0 to 39.9II Extremely High≥40IIIExtreme Obesity Classification of Overweight & Obesity by BMI ORLISTAT
Classification 1 --<18.5Underweight to 24.9Normal Increased25.0 to 29.9Overweight High30.0 to 34.9IObesity Very High35.0 to 39.9II Extremely High≥40IIIExtreme Obesity Classification of Overweight & Obesity by BMI ORLISTAT")
5
Obesity health risks Obesity Heart Failure Cancer Kidney Failure Type 2 diabetes Athero- sclerosis Stroke Hypertension Gallbladder disease

7
International Diabetes Federation Definition: Abdominal obesity plus two other components: elevated BP, low HDL, elevated TG, or impaired fasting glucose

9
9

11
Waist Circumference Correlates Closely with Intra-Abdominal Adiposity (IAA) 300 200 100 0 r = 0.80 6080100120 Front Back Subcutaneous AT Visceral AT Waist circumference (cm) IAA (cm 2 ) Pare A et al. Obes Res. 9(9):526-34; 2001
:526-34;")
12
Glucose Output Glucose GlucoseUptake Large IR fat cells Excess fat in key organs – leading to MD/ CVD FFAS ↓Adiponectin PAI-1, IL-6, TNF- ANGII ALTGGTCRP,PAI-1 ALT - Sattar et al, Diabetes 2004 PAI-1 -Festa et al, Diabetes 2002 Adiponectin - Lindsay et al, Lancet 2002 Lawlor, Sattar et al, AJE Sattar Clin Lab Inter TG SD. LDL, apoB Diet, exercise

13
IDF Country-/ethnicity-specific for waist circumference Country/ethnic groupWaist circumference (cm) (as measure of central obesity) Europid, Middle Eastern Male Female ≥ 94 ≥ 80 South AsiansMale Female ≥ 90 ≥ 80 ChineseMale Female ≥ 90 ≥ 80 JapaneseMale Female ≥ 85 ≥ 90 Diabetes Voice - September 2005 Volume 50 Issue 3
 (as measure of central obesity) Europid, Middle Eastern Male Female ≥ 94 ≥ 80 South AsiansMale Female ≥ 90 ≥ 80 ChineseMale Female ≥ 90 ≥ 80 JapaneseMale Female ≥ 85 ≥ 90 Diabetes Voice - September 2005 Volume 50 Issue 3")
14
Hydrodensitometry

15
Skinfold Thickness measures double thickness of skin and subcutaneous fat Advantages: –inexpensive –fast –portable –large database

16
Segmental Body Composition Analyzer

17
BIA: basic theory The body can be considered to be a series of cylinders. Resistance is proportional to the length of the cylinder Resistance is inversely proportional to the cross-sectional area

18
Major types of BIA analyzers

19
Advanced Body Composition Assessment by DEXA

20
RMI ;VISCERAL FAT Subcutaneous AT Visceral AT

21
21 Normal metabolic profile Smoking ‘Unfavourable’ genotype Maladaptive response to stress NMR Altered metabolic profile

22
22

23
Inflammation in adipose tissue

24
24

25
OBESITY DIABETES MELLITUS INSULIN RESISTANCE INSULIN SECRETION DEFECT GENETIC PREDISPOSITION ENVIRONMENTAL FACTORS GLUCO- AND LIPO- TOXICITY Low physical activity High energy intake Genes Vicious circle IGT FFA TNF-a, resistin, leptin, adiponectin … LiverMuscles

26
Insulin resistance or metabolic syndrome Type 2 diabetes Atherosclerosis Hypertension Impaired glucose tolerance Dyslipidemia Insulin resistance Obesity (central) Obstructive Sleep apnea Proteinuria Hepatopathy Polycystic ovary diseaseHyperuricaemia Decreased fibrinolytic activity Acanthosis nigricans
 Obstructive Sleep apnea Proteinuria Hepatopathy Polycystic ovary diseaseHyperuricaemia Decreased fibrinolytic activity Acanthosis nigricans")
27
Environment Early Life Low birth weight Poor nutrition Adult Life Sedentary lifestyle Dietary factors Cardiovascular Disease Genes Metabolic Syndrome The Metabolic Syndrome: genes & environment interacting

28
Three or more of the following five factors : Waist circumference > 102 cm in men and > 88 cm in women Plasma triglycerides > 150 mg/dl HDL-C < 40 mg/dl in men, <50 mg/dl in women BP > 130/85 mm Hg Plasma glucose > 100 mg/dl Metabolic Syndrome IDF,ATP III- 2005

29
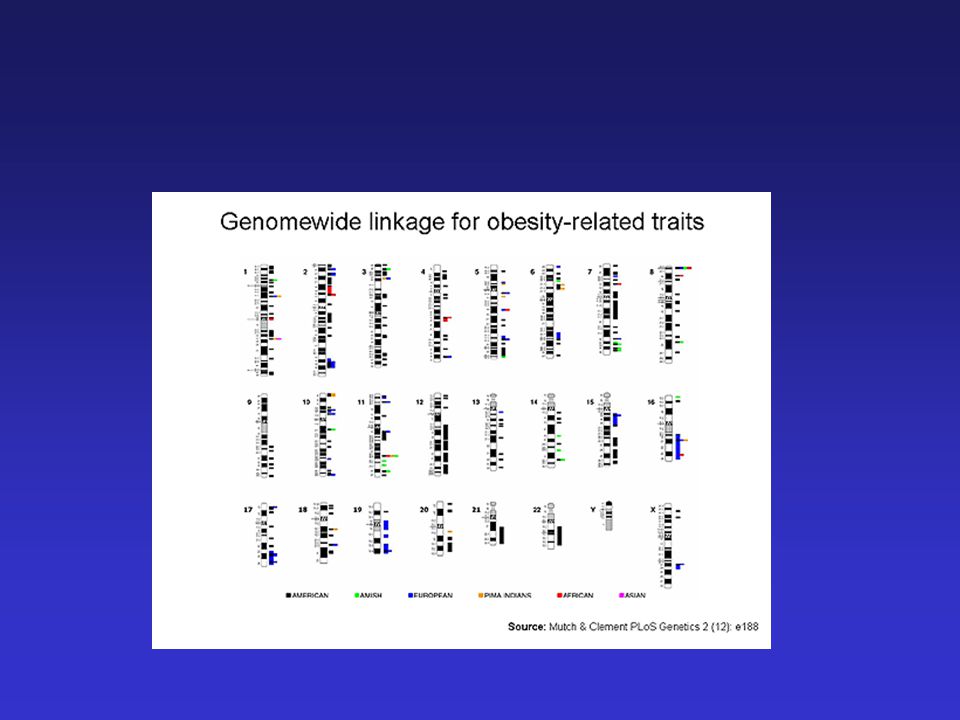
Does Metabolic Syndrome exist or is it a sum of its risk components? Components of the system occur more often than expected by chance –Common underlying process Heritability of Metabolic Syndrome –26% - 48% Linkage loci –Chromosomes 1,2,5,6,17,18 Candidate Genes –LDLR, PPARG, APOA5, CYP3A4, C1QTNF5

30
Syndrome Wikipedia encyclopedia The term syndrome derives from the Greek συνδρομή (sundromē) and means "concurrence of symptoms, concourse“Greek It is an association of several clinically recognizable features, signs & symptoms phenomena or characteristics that often occur togethersignssymptoms the presence of one or more features alerts the physician to the possible presence of the othersphysician
 and means concurrence of symptoms, concourse Greek It is an association of several clinically recognizable features, signs & symptoms phenomena or characteristics that often occur togethersignssymptoms the presence of one or more features alerts the physician to the possible presence of the othersphysician")
31
Is Metabolic Syndrome a valid Indicator of Cardiovascular Risk ? Yes The risk from the metabolic syndrome for major CVD events is approximately twice as high as for those without the syndrome. For type 2 diabetes, the metabolic syndrome confers an approximate 5 – fold greater risk Lakka H M etal JAMA 2002;288:2709 - 16

32
People with the Metabolic Syndrome have three times the risk of suffering a heart attack or stroke – and twice the risk of dying from such an event – compared with people without the syndrome. Diabetes Voice September 2005 Volume 50 Issue 3

33
A big waist increases the risk of developing type 2 diabetes <7171–75.976–8181.1–8686.1–9191.1–96.3>96.3 24 20 16 12 8 4 0 Relative risk Waist circumference (cm) Carey V, 1997 December 2005
 Carey V, 1997 December 2005")
34
A big waist is associated with multiple cardiovascular risk factors 30 20 10 0 Low HDL-C a High TG b High FPG c High BP d >2 risk factors e Prevalence of high waist circumference (%) a 150 mg/dL; c >110 mg/dL; d >130/85 mmHg; e NCEP/ATP III metabolic syndrome US population age >20 years NHANES 1999–2000 cohort
 a 150 mg/dL; c >110 mg/dL; d >130/85 mmHg; e NCEP/ATP III metabolic syndrome US population age >20 years NHANES 1999–2000 cohort")
35
Big waist: a major underlying cause of acute myocardial infarction Yusuf S, 2004 PAR (%) a a Proportion of MI in the total population attributable to a specific risk factor Big waist predicts the risk of CVD beyond BMI Cardiometabolic risk factors in the InterHeart Study 0 20 40 60 18 HTN 10 Diabetes 20 Big waist 49 Abn Lipids December 2005
 a a Proportion of MI in the total population attributable to a specific risk factor Big waist predicts the risk of CVD beyond BMI Cardiometabolic risk factors in the InterHeart Study HTN 10 Diabetes 20 Big waist 49 Abn Lipids December 2005")
36
Common Hormonal Abnormalities Associated with Obesity Increased cortisol production Insulin resistance Decreased sex hormone-binding globulin in women Decreased progesterone levels in women Decreased testosterone levels in men Decreased growth hormone production

37
Lyari Survey Prevalence of metabolic syndrome according to three different Criteria

38
Atherogenic dyslipidemia –Elevated Apolipoprotein B –Triglycerides –LDL-c –HDL-c Elevated blood pressure Elevated plasma glucose Prothrombotic state Proinflammatory state 38

39
Prevent Obesity to prevent Metabolic Syndrome

40
Obesity in Syria BMI>30kg/m2> 25 y ALBACHE N.,R Al-Ali, S. Rastam, F. M. Fouad, F.Mzayek, W. Maziak : Epidemiology of Type 2 Diabetes in Aleppo, Syria ( submetted dada)
.")
41
Diabetes Mellitus in Syria 2006(>25y) Aleppo study of prevalence of DM and C.V.Risk Factors, Diabetes Research Unit,Aleppo University 2006, (SUMETTED DATA )
 Aleppo study of prevalence of DM and C.V.Risk Factors, Diabetes Research Unit,Aleppo University 2006, (SUMETTED DATA )")
42
METABOLIC SYNDROME IN SYRIA ALI R..,MEZIAK W.,ROSTOM S.,ALBAHE N.,FOUAD F ;SUBMITTED DATA

43
ABC’s of Metabolic Syndrome Management InterventionGoals / Treatment A Antiplatelet agent Treat all high-risk patients with low-dose aspirin (or clopidogrel in those with CVD if aspirin is contraindicated) and consider low-dose aspirin in moderately high-risk patients. B BP Control Aim for BP <130/85 mm Hg, or <130/80 mm Hg for type 2 diabetes. Consider ACE-I or ARBs and low dose diuretics in combination rx.

44
ABC’s of Metabolic Syndrome Management Interventio n Goals C Cholesterol Management LDL-C targets, ATP III guidelines – High Risk: CHD, CHD risk equivalents (incl. >20% 10-year risk): <100 mg/dL (option <70 mg/dl if CVD present) – Moderately High Risk (10-20% risk or subclinical disease) 2 RF: <130 mg/dL, option <100 mg/dL – Moderate Risk (2+ RF, <10%) <130 mg/dL -- Low Risk: 0-1 RF: <160 mg/dL Non-HDL-C targets 30 mg/dL higher HDL-C: >40 mg/dL (men) >50 mg/dL (women) TG: <150 mg/dL Cigarette Smoking Long term smoking cessation
: <100 mg/dL (option <70 mg/dl if CVD present) – Moderately High Risk (10-20% risk or subclinical disease) 2 RF: <130 mg/dL, option <100 mg/dL – Moderate Risk (2+ RF, <10%) <130 mg/dL -- Low Risk: 0-1 RF: <160 mg/dL Non-HDL-C targets 30 mg/dL higher HDL-C: >40 mg/dL (men) >50 mg/dL (women) TG: <150 mg/dL Cigarette Smoking Long term smoking cessation.")
45
Obesity Is Caused by Long-Term Positive Energy Balance Fat Stores

46
Caloric Intake 1970 2000 Carbohydrates (fruits, grains, sugars, and vegetables) Pounds consumed per person: 1,497 Pounds consumed per person: 1,775 Protein 588lb Fat & oils 56lb Fruits 241lb Grains 136lb Vegetables 337lb Sugars 139lb Protein 621lb Fat & oils 77lb Fruits 280lb Grains 200lb Vegetables 425lb Sugars 172lb (per Person/Year) Eating more of everything
 Pounds consumed per person: 1,497 Pounds consumed per person: 1,775 Protein 588lb Fat & oils 56lb Fruits 241lb Grains 136lb Vegetables 337lb Sugars 139lb Protein 621lb Fat & oils 77lb Fruits 280lb Grains 200lb Vegetables 425lb Sugars 172lb (per Person/Year) Eating more of everything")
47
Dietary fat promotes Obesity : Evidence from Epidemiology 80 60 50 40 30 20 10 70 20 25 30 35 40 Kuwait Morocco Philippines Mali China IndiaCongo Tunisia Malaysia Australia USA New Caledonia Italy Brazil Russian Federation Kyrgzstan Cuba S. Africa Mauritius Saudi Arabia Dietary Fat (%) Percentage BMI > 25.0 Bray & Popkin, Am. J. Clin. Nutr., 1998 r = 0.88
 Percentage BMI > 25.0 Bray & Popkin, Am. J. Clin. Nutr., 1998 r =")
50
Obesity Treatment Pyramid 50 BMI > 40 35 30 25 DietPhysical Activity Lifestyle Modification Pharmacotherapy Bariatric Surgery BMI ≥ 40 35 30 25 Source: The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. National Institutes of Health. National Heart, Lung, and Blood Institute. October 2000, NIH Publication No. 00-4084.

51
What is a Healthy Diet? Less 20-30 % of total K Carbohydrate: 55% Protein: 15% Fat: 30% Variety Moderation

54
الجهد الفيزيائي KCal \m 2 \ h 35 النوم 50 الوقوف 60 الكتابة 140 المشي 250 ركوب الدراجة 600 الجري السريع

55
What are the Benefits of Physical Activity and Regular Exercise on Obesity? Reduced age-standardized mortality rates Reduced plasma fibrinogen levels Reduced plasminogen activator inhibitor type 1 Reduced platelet aggregation Reduced inflammatory cytokines including CRP Reduction in systemic blood pressure Increased insulin sensitivity Reduced glucose intolerance Reduced serum LDL Reduced serum triglycerides Increased serum HDL Improved endothelial function Reduced dependence of assisted living in latter life Enhanced weight control Increased cardiovascular fitness Increased musculoskeletal fitness 21. Carnethon MR, et al. JAMA. 2005;294:2891-2988.

56
Currently Available Agents Indicated for Treatment of Obesity Generic/Brand NameUsual Dose Mechanism of Action Side Effects Orlistat/Xenical Sibutramine/Meridia Phentermine/ Adipex, Fastin, Ionamin and others 120 mg with each meal 5-15 mg/d 15-37.5 mg per day as a single or split dose Peripheral: Blocks absorption of about 30% of consumed fat Central: Inhibits synaptic reuptake of norepinephrine and serotonin Central: Stimulates release of norepinephrine GI symptoms (oily spotting, flatus with discharge, fecal urgency, oily stools, incontinence) Dry mouth, constipation, headache, insomnia, increased blood pressure, tachycardia CNS stimulation, tachycardia, dry mouth, insomnia, palpitations
 Dry mouth, constipation, headache, insomnia, increased blood pressure, tachycardia CNS stimulation, tachycardia, dry mouth, insomnia, palpitations")
57
What are the Barriers to Obesity Treatment? Obese patients are aware of the need for lifestyle modification to manage weight Difficulty translating advice into practice Unrealistic expectations and goals Lack of skills to manage restraint Lack of support and sound advice

58
Effect of Mediterranean-style diet in the metabolic syndrome 180 pts with metabolic syndrome randomized to Mediterranean-style vs. prudent diet for 2 years Those in intervention group lost more weight (-4kg) than those in the control group (+0.6kg) (p<0.01), and significant reductions in CRP and Il-6. After 2 years, 40 pts in intervention group still had features of metabolic syndrome compared to 78 pts in the control group Esposito K et al. JAMA 2004; 292(12): 1440-6.
 than those in the control group (+0.6kg) (p<0.01), and significant reductions in CRP and Il-6. After 2 years, 40 pts in intervention group still had features of metabolic syndrome compared to 78 pts in the control group Esposito K et al. JAMA 2004; 292(12):")
59
Therapeutic Lifestyle Changes Nutrient Composition of TLC Diet NutrientRecommended Intake Saturated fat Less than 7% of total calories Polyunsaturated fatUp to 10% of total calories Monounsaturated fat Up to 20% of total calories Total fat25–35% of total calories Carbohydrate50–60% of total calories Fiber20–30 grams per day Protein Approximately 15% of total calories CholesterolLess than 200 mg/day Total calories (energy)Balance energy intake and expenditure to maintain desirable body weight/ prevent weight gain
Balance energy intake and expenditure to maintain desirable body weight/ prevent weight gain")
60
Orlistat Indications Among obese patients who meet the criteria for anti-obesity drug therapy, orlistat is most likely to benefit those who: –Do not feel hungry –Are not preoccupied with food –Eat out or order-in often –Have increased cardiovascular disease risk or multiple cardiovascular risk factors –Are older –Take multiple medications Orlistat is taken 3 times daily with meals

61
052104156208 -6.4 -4.4 *** orlistat and waist circumference ***p<0.0001 vs placebo + lifestyle 0 -2 -4 -6 -8 -10 -12 Change in waist circumference (cm) Placebo + lifestyleXenical + lifestyle Week Torgerson et al Submitted
 Placebo + lifestyleXenical + lifestyle Week Torgerson et al Submitted")
62
Sjostrom et al. 9th ICO, Sao Paulo 2002. Poster Presentation XENDOS results Cumulative incidence of MD2 Incidence of T2D (%) p=0.0032 0265278104130156182208 0 2 4 6 8 10 Weeks 9.0% 6.2% RR 37% Hazard ratio reduction vs placebo plus lifestyle Placebo + lifestyleXenical + lifestyle
 p= Weeks 9.0% 6.2% RR 37% Hazard ratio reduction vs placebo plus lifestyle Placebo + lifestyleXenical + lifestyle.")
63
Total cholesterol in XENDOS ***p<0.001 vs placebo + lifestyle -7.9% -2.3% *** 521041562080 Week 0 -5 -10 -15 Placebo + lifestyleXenical + lifestyle Change in total cholesterol (%) Torgerson et al Submitted
 Torgerson et al Submitted")
64
Currently Available Agents Indicated for Treatment of Obesity Generic/Brand NameUsual Dose Mechanism of Action Side Effects Orlistat/Xenical Sibutramine/Meridia Phentermine/ Adipex, Fastin, Ionamin and others 120 mg with each meal 5-15 mg/d 15-37.5 mg per day as a single or split dose Peripheral: Blocks absorption of about 30% of consumed fat Central: Inhibits synaptic reuptake of norepinephrine and serotonin Central: Stimulates release of norepinephrine GI symptoms (oily spotting, flatus with discharge, fecal urgency, oily stools, incontinence) Dry mouth, constipation, headache, insomnia, increased blood pressure, tachycardia CNS stimulation, tachycardia, dry mouth, insomnia, palpitations
 Dry mouth, constipation, headache, insomnia, increased blood pressure, tachycardia CNS stimulation, tachycardia, dry mouth, insomnia, palpitations")
65
Orlistat (Alphastat) Pancreatic lipase inhibitor that blocks the absorption of up to one third of ingested fat. In addition to helping reduce weight, orlistat has been shown to also: – lower plasma low-density lipoprotein cholesterol (LDL) cholesterol levels. –The decline in LDL cholesterol is greater than that expected due to weight loss alone. –Lower HgbA1C in diabetic patients
 cholesterol levels. –The decline in LDL cholesterol is greater than that expected due to weight loss alone. –Lower HgbA1C in diabetic patients.")
66
Orlistat (Alphastat) Indications Among obese patients who meet the criteria for anti-obesity drug therapy, orlistat is most likely to benefit those who: –Do not feel hungry –Are not preoccupied with food –Eat out or order-in often –Have increased cardiovascular disease risk or multiple cardiovascular risk factors –Are older –Take multiple medications Orlistat is taken 3 times daily with meals
 Indications Among obese patients who meet the criteria for anti-obesity drug therapy, orlistat is most likely to benefit those who: –Do not feel hungry –Are not preoccupied with food –Eat out or order-in often –Have increased cardiovascular disease risk or multiple cardiovascular risk factors –Are older –Take multiple medications Orlistat is taken 3 times daily with meals")
67
Orlistat [Diabetes Care 27(1):33-40, 2004. © 2004 American Diabetes Association, Inc.] EGP = endogenous glucose production and Rd = glucose utilization

68
Orlistat – Side effects Because it blocks intestinal absorption of fat it can result in diarrhea and steatorrhea This is minimized by maintaining a strict low fat diet (<30% of diet) Another concern is the loss of fat soluble vitamins with a potential for malnutrition. To prevent this, recommend a daily multivitamin for all patients on this therapy

69
XENDOS results Effect of orlistat on body weight -4.1 kg -6.9 kg p<0.001 vs placebo 052104156208 -12 -9 -6 -3 0 Placebo + lifestyleXenical + lifestyle Week Weight change (kg) Sjostrom et al. 9th ICO, Sao Paulo 2002. Poster Presentation

70
052104156208 -6.4 -4.4 *** Xenical and waist circumference ***p<0.0001 vs placebo + lifestyle 0 -2 -4 -6 -8 -10 -12 Change in waist circumference (cm) Placebo + lifestyleXenical + lifestyle Week Torgerson et al Submitted
 Placebo + lifestyleXenical + lifestyle Week Torgerson et al Submitted")
71
Sjostrom et al. 9th ICO, Sao Paulo 2002. Poster Presentation XENDOS results Cumulative incidence of type 2 diabetes Incidence of T2D (%) p=0.0032 0265278104130156182208 0 2 4 6 8 10 Weeks 9.0% 6.2% RR 37% Hazard ratio reduction vs placebo plus lifestyle Placebo + lifestyleXenical + lifestyle
 p= Weeks 9.0% 6.2% RR 37% Hazard ratio reduction vs placebo plus lifestyle Placebo + lifestyleXenical + lifestyle.")
72
Total cholesterol in XENDOS ***p<0.001 vs placebo + lifestyle -7.9% -2.3% *** 521041562080 Week 0 -5 -10 -15 Placebo + lifestyleXenical + lifestyle Change in total cholesterol (%) Torgerson et al Submitted
 Torgerson et al Submitted")
Similar presentations









 describes relative weight for height: weight (kg)/height (m 2 ) Overweight = 25–29.9 BMI Obesity = >30 BMI.>")










 and Drug Therapy in Different Risk Categories Risk Category LDL Goal (mg/dL)>")



 are obese. 17% (12.5 million) of children 2—19 years are obese. Top leading.>")