Download presentation
Presentation is loading. Please wait.

1
Update of Transcatheter Closure of Ventricular Septal Defect in China Yong-wen Qin Department of Cardiology, Changhai Hospital, Second Military Medical University, Shanghai

2
1 、 The number and quality of VSD intervention improved during past ten years

3
The first pmVSD patients treated with symmetric occluder (2001.12 , 21) The first post-MI VSD patient treated with symmetric occluder (2001.10) The first cases of VSD intervention in our center
 The first post-MI VSD patient treated with symmetric occluder ( ) The first cases of VSD intervention in our center")
4
Large VSD closure in 2002 large VSD (15mm) closed by 18mm occluder
 closed by 18mm occluder")
5
Development of CHD intervention from 1990s-2011 in China year Patient number *

6
VSD intervention in last 3 years in China ( 394 hospitals ) 200920102011 total160451867122967 ASD552767938089 PDA470554664075 VSD 352142525474 PBPV603680905 Success rate97.24%97.67%98.11% Complication0.2%0.17%0.12% Mortality0.03%0.05%0.02%
 total ASD PDA VSD PBPV Success rate97.24%97.67%98.11% Complication0.2%0.17%0.12% Mortality0.03%0.05%0.02%")
7
2 、 Three kind of VSD devices invented and clinical use in China

8
Modified VSD device in China symmetric occluder thin waist occluder asymmetric occluder

9
Schematic diagram of ventricular septal defect occluder

10
The classification of VSD by ventriculography A tubular B window-like C aneurysmal D infundibular Individualization choice of the occluder according to anatomy of VSD

11
Infundibular VSD symmetric occluder

12
How to choose the occluder according to VSD Intracristal VSD asymmetric occluder

13
Intracristal VSD

14
Symmetric device ---Aortic valve regurgitation asymmetric device ---no aortic valve regurgitation

15
Intracristal VSD

17
Aortic valve regurgitation--- device inclined to one side The direction of left disk marker should be apex

18
Intracristal VSD When the marker turn to apex, aortic valve regurgitation became trace

19
Intracristal VSD No aortic valve regurgitation-- long rim direction pointed to cardiac apex

20
PV VSD Echo: subpulmonary VSD---near PV

21
VSD complicared with aortic valve prolapse

22
VSD 5mm ----- 0 rim device (10mm)
")
23
Postoperation, no aortic regurgitation However, occluder maybe oversized

25
VSD 7mm, near aortic valve

27
Echo: subpulmonary VSD---near PV

28
Device 9mm (L), change to Device 11mm (R)
, change to Device 11mm (R)")
29
no aortic valve regurgitation

31
Multi-hole VSD---device choice multi-hole VSD thin waist occluder

32
One device close three holes

33
VSD2 VSD1 device For VSD2 VSD1 VSD with two holes

34
Two device for two holes

35
Large VSD -1

36
Large VSD -2 14mm A6B2 device

37
Large VSD -3 No aoric valve regurgitation,no TVR

38
PDA device for large VSD

39
20mm PDA device

40
PDA device for large VSD

41
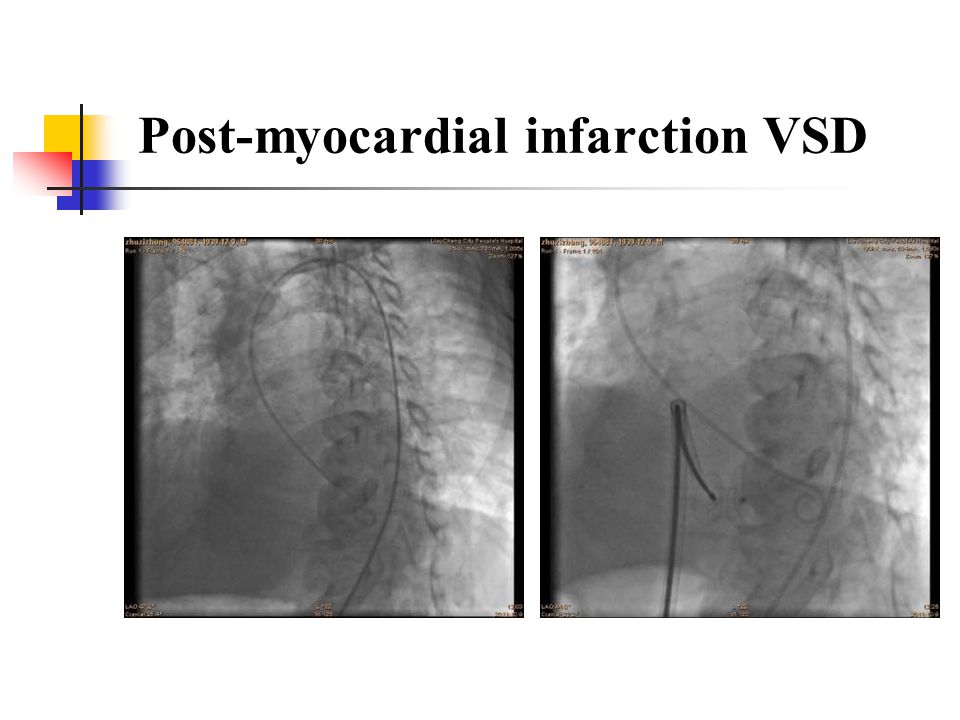
post-myocardial infarction VSDmuscular occluder Post-myocardial infarction VSD

43
Postoperative residual perimembranous VSD Transcatheter closure of postoperative residual perimembranous VSD

44
PS and large VSD VSD 17mm, device 24mm

45
3 、 Conduction Block complicated with VSD Intervention: experience in china

46
anthorsampleAVB%cAVB%PPMonsetrecovery Song et al 328 27(8.2%) 8012h-614-20d Xie et al 644 16(2.5%) 623-6d8-10d Wang et al 364 20(5.5%) 403-14dNA Zhang et al 232 17(7.3%) 1204-6d4-27d Wu et al 112 22(19.6%) 005d Zhu et al 358 23(6.4%) 501-8d6-10d Liu et al 210 41(19.5) 617d21d Yu et al 112 37(33%) 803-9d3-7d Qin et al 203 11(5.4%) 102-5d5-10d Past Literature Review in China
 8012h d Xie et al (2.5%) 623-6d8-10d Wang et al (5.5%) dNA Zhang et al (7.3%) d4-27d Wu et al (19.6%) 005d Zhu et al (6.4%) 501-8d6-10d Liu et al (19.5) 617d21d Yu et al (33%) 803-9d3-7d Qin et al (5.4%) 102-5d5-10d Past Literature Review in China")
47
Clinial trial data of Amplatzer VSD device Catheter Cardiovasc Interv. 2006, 68(4):620-8. (n=100) J Am Coll Cardiol. 2006, 47(2): 319-25. (n=35) Eur Heart J. 2007, 28: 2361. (n=430) N: 565 Success rate 91-95 % 3rd AVB 2-8 % PPM 12 (3.8 % ) death1
: (n=100) J Am Coll Cardiol. 2006, 47(2): (n=35) Eur Heart J. 2007, 28: (n=430) N: 565 Success rate % 3rd AVB 2-8 % PPM 12 (3.8 % ) death1.")
48
The data on VSD occluder in China from 21 centers (N=9311, 2007) Success rate 96.45% Death 0.05% (5) Transient cAVB 0.63% (59) PPM 0.09% (8)
 Success rate 96.45% Death 0.05% (5) Transient cAVB 0.63% (59) PPM 0.09% (8)")
49
2011 registry data in China 5474 cases with vsd in 394 hospital in china PPM 1case

50
The data from Changhai hospital (2001-2012) 2001-2002, 196 cases underwent percutaneous procedure (using symmetry device), no cAVB 2003-2006, among 300 cases (Symmetry, Eccentric 、 thin waist devices), 11 cases complicated transient 3rd degree AVB, permanent pacemaker occur in 1 case 2007-2012, sequence 550 cases with Symmetry, Eccentric,thin waist devices, cAVB occur 1 patient
 , 196 cases underwent percutaneous procedure (using symmetry device), no cAVB , among 300 cases (Symmetry, Eccentric 、 thin waist devices), 11 cases complicated transient 3rd degree AVB, permanent pacemaker occur in 1 case , sequence 550 cases with Symmetry, Eccentric,thin waist devices, cAVB occur 1 patient")
51
The possible reason of increase AVB from 2003 to 2006 ? Patients: patients non-selected, consecutive patients admitted Doctors: personnel stability, and operation technology maturity Indication: increased intracristal multi-holes and aneurysm type VSD Devices: Application of asymmetric occluder

52
Device waist length and AVB 2001--2003---more than 3.5 mm---no case with AVB 2003--2006---less than 2.5mm---12/300 with AVB 2007--2012---more than 3.5mm---no case with AVB

53
Chinese device shape at immediate compared with amplatzer devices amplatzer devicesShape change AVB device shape at immediate

54
3 rd AVB

55
My opinion is that device is key factor for conduction block. Device tension---flex Contact area with the septal Size --- waist diameter Length of waist The risk factor of AVB

56
Choose the proper device size Avoid oversized device AVB seems to be fewer in symmetric occluder. “Nice” occluder Individualized choice of occluder for pts Very experienced hands Major success experience on prevention of AVB

57
Other Risk factors for the Occurrence of AVB Type of VSD: perimembranous VSD inlet VSD (behind the septal leaflet of tricuspid valve)
")
58
The VSD intervention is safe, effective and an alternative method to surgery or first choice in China

59
Wire-Maintaining Technique Using this novel technique, the reconstruction of ‘‘arteriovenous wire loop’’ could be avoided in patients requiring device replacement. QIN, et al. CCI 75:66 – 71 (2010) 4 、 Useful technique in intervention of VSD
 4 、 Useful technique in intervention of VSD.")
60
Large VSD (22mm) Wire-Maintaining Technique
 Wire-Maintaining Technique")
61
How to choose the patient for VSD closure- ---TTE three views the apical 5-chamber view LV long axis l view Aortic short axis view Compared to TEE, TTE is enough!

62
Thank you

Similar presentations










>")





>")
: CERA TRIAL Zhi-wei.>")





