Download presentation
Presentation is loading. Please wait.

1
Scott Christensen, MD UC Davis Comprehensive Cancer Center

2
Overview Review recently presented data in neoadjuvant therapy of Her 2+ breast cancer Speculate on future therapeutic implications

3
2011 DATA

5
*No change if pCR by other definitions Increased rates of BCS in T arms

6
*pCR = no invasive disease in breast

9
5 FU 600 mg/m 2 Epi 75 mg/m 2 CTX 600 mg/m 2 q. 3 weeks Paclitaxel 80 mg/m 2 q. 1 week Trastuzumab 4 mg/kg loading dose 2 mg/kg q. 1 week RANDOMIZATIONRANDOMIZATION Lapatinib 1000 mg CDD Lapatinib 1500 mg continuous daily dose (CDD) COREBIOPSYCOREBIOPSY SURGERYSURGERY A B C Cher-Lob Trial Design LVEF HER2+ operable breast cancer Guarneri, V et.al., J Clin Oncol 29: 2011 (suppl; abstr 507)
 COREBIOPSYCOREBIOPSY SURGERYSURGERY A B C Cher-Lob Trial Design LVEF HER2+ operable breast cancer Guarneri, V et.al., J Clin Oncol 29: 2011 (suppl; abstr 507).")
10
TBCRC 006:Neoadjuvant Lapatinib & Trastuzumab Without Chemotherapy : Study Schema Lap (L) + Tras (T) + Endocrine Rx if ER+ 02 812 Bx Lapatinib (1000 mg/day) Trastuzumab (4 mg/kg load, 2 mg/kg q-weekly) Weeks Chang, JCN et.al., J Clin Oncol 29: 2011 (suppl; abstr 505)
 + Tras (T) + Endocrine Rx if ER Bx Lapatinib (1000 mg/day) Trastuzumab (4 mg/kg load, 2 mg/kg q-weekly) Weeks Chang, JCN et.al., J Clin Oncol 29: 2011 (suppl; abstr 505)")
14
pCR Rates with Neoadjuvant anti-HER2 Therapies Pac Pac FEC FEC Pac EC Doc

15
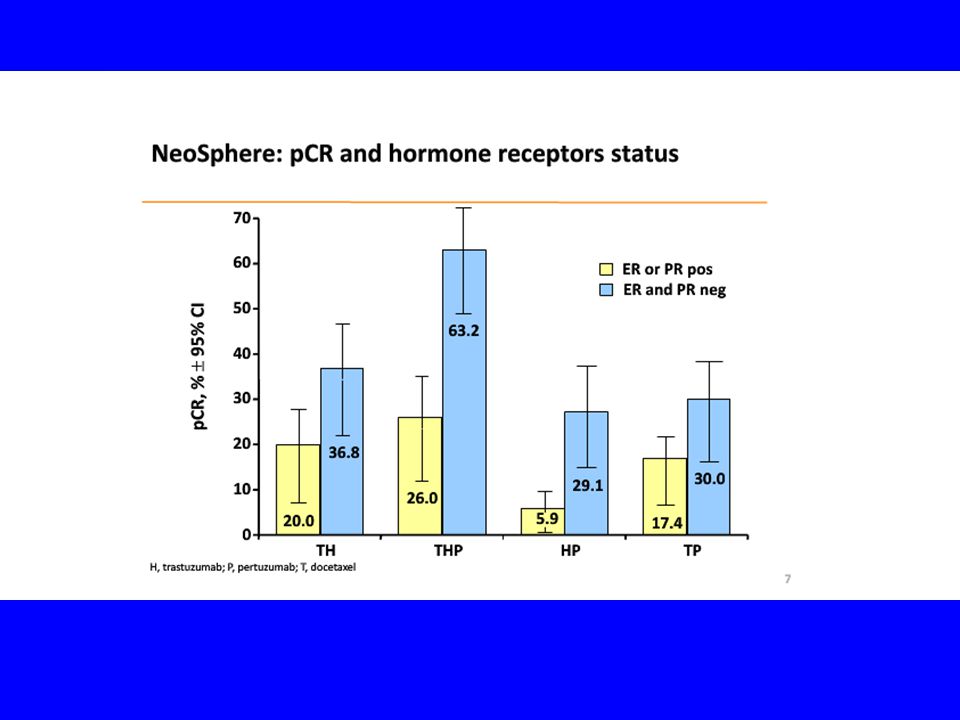
Rates of pCR in HER2+ Tumors by Hormone- receptor Status

16
2012 DATA

26
TRYPHAENA

27
Study Endpoints Primary endpoint: – Cardiac safety Symptomatic LVSD (grade ≥3) LVEF declines (≥10 percentage points and below 50%) Secondary endpoints: – Toxicity – pCR – Clinical response rate – Rate of BCS – DFS, OS – Biomarker evaluation Schneeweiss, SABCS 2011, abs #S5-6
 LVEF declines (≥10 percentage points and below 50%) Secondary endpoints: – Toxicity – pCR – Clinical response rate – Rate of BCS – DFS, OS – Biomarker evaluation Schneeweiss, SABCS 2011, abs #S5-6")
28
Eligibility Criteria Centrally confirmed HER2-positive locally advanced, inflammatory, or early-stage breast cancer Primary tumor ≥2 cm Baseline LVEF ≥55% ECOG PS 0 or 1 No previous anticancer therapy or radiotherapy for any malignancy Adequate bone marrow, liver, and renal function Schneeweiss, SABCS 2011, abs #S5-6

29
Baseline Patient Characteristics FEC/HP →THP N=72 FEC →THP N=75 TCHP N=76 Med age, yrs (range)49 (27-77)49 (24-75)50 (30-81) ECOG 065 (91.5%)66 (88.0%)67 (88.2%) ECOG 16 (8.5%)9 (12.0%)9 (11.8%) ER and/or PR +39 (53.4%)35 (46.7%)40 (51.9%) ER and/or PR-34 (46.6%)40 (53.3%)36 (48.1%) Disease Type Operable53 (72.6%)54 (72.0%)49 (63.6%) LABC15 (20.5%)17 (22.7%)24 (31.2%) IBC5 (6.8%)4 (5.3%)4 (5.2%) HER2 IHC 0 and 1+1 (1.4%)0 (0.0%) HER2 IHC 2+5 (6.8%)1 (1.3%)2 (2.6%) HER2 IHC 3+67 (91.8%)74 (98.7%)75 (97.4%) HER2 FISH +69 (94.5%)69 (92.0%)73 (94.8%) HER2 FISH-0 (0.0%)1 (1.3%)2 (2.6%) HER2 unknown4 (5.5%)5 (6.7%)2 (2.6%) Schneeweiss, SABCS 2011, abs #S5-6
49 (27-77)49 (24-75)50 (30-81) ECOG 065 (91.5%)66 (88.0%)67 (88.2%) ECOG 16 (8.5%)9 (12.0%)9 (11.8%) ER and/or PR +39 (53.4%)35 (46.7%)40 (51.9%) ER and/or PR-34 (46.6%)40 (53.3%)36 (48.1%) Disease Type Operable53 (72.6%)54 (72.0%)49 (63.6%) LABC15 (20.5%)17 (22.7%)24 (31.2%) IBC5 (6.8%)4 (5.3%)4 (5.2%) HER2 IHC 0 and 1+1 (1.4%)0 (0.0%) HER2 IHC 2+5 (6.8%)1 (1.3%)2 (2.6%) HER2 IHC 3+67 (91.8%)74 (98.7%)75 (97.4%) HER2 FISH +69 (94.5%)69 (92.0%)73 (94.8%) HER2 FISH-0 (0.0%)1 (1.3%)2 (2.6%) HER2 unknown4 (5.5%)5 (6.7%)2 (2.6%) Schneeweiss, SABCS 2011, abs #S5-6")
31
Other Notable G 3/4 AEs Adverse events FEC/HP →THP N=72 FEC →THP N=75 TCHP N=76 Neutropenia34 (47.2%)32 (42.7%)35 (46.1%) Febrile neutropenia 13 (18.1%) 7 (9.3%)13 (17.1%) Leukopenia14 (19.4%) 9 (12.0%) 9 (11.8%) Diarrhea 3 (4.2%) 4 (5.3%) 9 (11.8%) Schneeweiss, SABCS 2011, abs #S5-6
32 (42.7%)35 (46.1%) Febrile neutropenia 13 (18.1%) 7 (9.3%)13 (17.1%) Leukopenia14 (19.4%) 9 (12.0%) 9 (11.8%) Diarrhea 3 (4.2%) 4 (5.3%) 9 (11.8%) Schneeweiss, SABCS 2011, abs #S5-6")
33
Breast Conserving Surgery When Mastectomy Was Planned* FEC/HP →THP N=46 FEC →THP N=36 TCHP N=37 Achieved (95% CI) 10 (21.7%) (10.9-36.4) 6 (16.7%) (6.4-32.8) 10 (27.0%) (13.8-44.1) Not Achieved36 (78.3%)30 (83.3%)27 (73.0%) * Patients in ITT population w/ T2-3 tumors for whom mastectomy was planned. Schneeweiss, SABCS 2011, abs #S5-6

34
Conclusions Low incidence of symptomatic/asymptomatic LVSD across all arms: – Concurrent admin of HP w/ Epi resulted in similar cardiac tolerability compared with sequential admin or the anthracycline-free regimen Neutropenia, FN, leukopenia, and diarrhea were the most frequent G 3/4 AEs across all arms. High pCR rates (57- 66%) w/ HP, regardless of chemotherapy chosen TRYPHAENA supports ongoing APHINITY study, a Phase III trial to evaluate HP + standard chemo in adjuvant setting. Schneeweiss, SABCS 2011, abs #S5-6
 w/ HP, regardless of chemotherapy chosen TRYPHAENA supports ongoing APHINITY study, a Phase III trial to evaluate HP + standard chemo in adjuvant setting. Schneeweiss, SABCS 2011, abs #S5-6.")
35
AC x 4 Weekly paclitaxel + trastuzumab Surgery Post-op trastuzumab AC x 4 Weekly paclitaxel + lapatinib AC x 4 Weekly paclitaxel + trastuzumab + lapatinib HER2+ palpable breast cancer (No T4 or N2) Randomization Core biopsies for correlative studies US NIH, 2007c. NSABP B-41

36
NSABP B-41 ASC0 2012 pCR rates 519/529 pts,51% node +, 63% HR+ pCR rates: 52.5% AC WP+T 53.2% AC WP+L 62.0% AC WP+T+L Increased rates diarrhea observed in lapatinib treament arms Higher pCR rates in HR- patients Similar rates of g3/4 LV systolic dysfunction Authors concluded substitution of lapatinib effective with acceptable toxicity; combined ant-her2 blockade numerically greater pCR, but not stastically significant Robidoux, A et.al., J Clin Oncol 30, 2012 (suppl; abst LBA506)
")
37
AVANTHER—ASCO 2012 Neoadjuvant phase II study; 44 stage II/III, Her2+; 58% ER+/PR+; 27.8% ER-/PR- Weekly paclitaxel, weekly trastuzumab, q3 wk bevacizumab for 12 weeks 36 patients had surgery at time of presentation; 44.4% pCR noted Rare >g3 AEs; 1 pt with severe HTN Authors concluded regimen safe and effective Abad, M et. Al., J Clin Oncol 30, 2012 (suppl; abst 602)
.")
38
ONGOING TRIALS AND NOVEL AGENTS

39
(paclitaxel 80 mg/m 2 /wks x 16) CALGB 40601 HER2+ Neoadjuvant Trial Schema SURGERYSURGERY dd AC x 4 Trastuzumab x 1 year Endocrine/RT Rx prn Trastuzumab Trastuzumab + lapatinib Lapatinib US NIH, 2009a.
 CALGB HER2+ Neoadjuvant Trial Schema SURGERYSURGERY dd AC x 4 Trastuzumab x 1 year Endocrine/RT Rx prn Trastuzumab Trastuzumab + lapatinib Lapatinib US NIH, 2009a.")
40
Novel Agents: HER2 HER1/2 TKI Pan HER TKI HER1/2/VEGFR TKI HER2 dimerization inhibitor Bispecific antibody Conjugated antibodies HSP90 inhibitors IGF-1R inhibitors (mAb, TKI) HDAC inhibitors PI3K inhibitors Akt inhibitors mTOR inhibitors HER2 vaccines Lapatinib, HKI-272, BIBW 2992, PKI-166 Canertinib, BMS-599626 XL647, AEE788 Pertuzumab Ertumaxomab Trastuzumab-MCC-DM1, trastuzumab-A-Z-CINN, 310- paclitaxel Tanespimycin, alvespimycin, CNF2024, IPI-504, AUY922, SNX5422 CP-751871, EM164, IMC-A12, NVP-ADW742, INSM-18 Vorinostat, LBH589, PXD101, NVP-LAQ824, depsipeptide, CI-994, MS-275 SF1126, BEZ235, XL147, XL765 Perifosine, XL418 Rapamycin, temsirolimus, everolimus, deforolimus
 HDAC inhibitors PI3K inhibitors Akt inhibitors mTOR inhibitors HER2 vaccines Lapatinib, HKI-272, BIBW 2992, PKI-166 Canertinib, BMS XL647, AEE788 Pertuzumab Ertumaxomab Trastuzumab-MCC-DM1, trastuzumab-A-Z-CINN, 310- paclitaxel Tanespimycin, alvespimycin, CNF2024, IPI-504, AUY922, SNX5422 CP , EM164, IMC-A12, NVP-ADW742, INSM-18 Vorinostat, LBH589, PXD101, NVP-LAQ824, depsipeptide, CI-994, MS-275 SF1126, BEZ235, XL147, XL765 Perifosine, XL418 Rapamycin, temsirolimus, everolimus, deforolimus")
41
Neratinib (HKI-272) Oral pan-ErbB receptor tyrosine kinase inhibitor Phase I/II study evaluating efficacy of combination neratinib plus trastuzumab in ErB2+ advanced breast cancer – Primary end point: 16-week PFS – 33 patients evaluable ORR: 27% PFS: 47% Median PFS: 19 weeks – No DLTs – Most common AEs Diarrhea Nausea Vomiting
 Oral pan-ErbB receptor tyrosine kinase inhibitor Phase I/II study evaluating efficacy of combination neratinib plus trastuzumab in ErB2+ advanced breast cancer – Primary end point: 16-week PFS – 33 patients evaluable ORR: 27% PFS: 47% Median PFS: 19 weeks – No DLTs – Most common AEs Diarrhea Nausea Vomiting")
42
ASCO 2012

43
CONCLUSIONS

44
Impact on Clinical Care Encouraging results from newly reported trials are continuing to establish a role for neoadjuvant therapy of Her2+ breast cancer Combination anti Her2 directed treatment is emerging as a potential standard of care What is the relevance of pCR endpoint in differing breast cancer subsets (TN, Her 2+/ER+, Her 2+/ER-, ER+/Her 2- lum A/B)? Beware of phase II trials and use of pCR as surrogate for DFS and OS In neoadjuvant and adjuvant settings, trastuzumab is standard therapy

Similar presentations













 vs FOLFIRI plus bev>")



 Phase III trial comparing AC (x4)taxane (x4) with taxane (x8) as adjuvant therapy for node-positive breast cancer: Results of N-SAS-BC02.>")
 on the Efficacy.>")


 versus FOLFOX4 in Patients with Advanced Colorectal Carcinoma Previously Treated.>")
 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")
 Treated with Anti Vascular Endothelial Growth Factor (VEGF)>")
: a randomised phase 3 trial Speaker: 陳鴻明.>")





: investigational agents TTP = median time to disease progression OS = median overall survival.>")
>")
