Download presentation
Presentation is loading. Please wait.

1
Childhood Matters: Health and Early Childhood Experiences
Michael Gardner MD, MPH Hillcrest Chairman and Professor of Obstetrics and Gynecology School of Community Medicine Jennifer Hays-Grudo, PhD George Kaiser Family Foundation Chair in Community Medicine Professor of Internal Medicine

2
Welcome to the womb…

4
You really can blame your mother?

5
Developmental Origins of Adult Health and Disease (DOHaD)
Barker hypothesis (Barker & Osmond, 1986; Barker, 1995) Fetal undernutrition associated with adult obesity, CVD and type II diabetes (Law et al., 1992; Sayer et al., 2004) Fetal undernutrition + rapid “catch-up growth” (Ong, 2006; Stettler et al., 2003, 2005) Thrifty phenotype (Hales & Barker, 2001) Adaptive response for deprived pretnatal environment maladaptive for postnatal environment Developmental Origins of Adult Health and Disease (DOHaD) (Gluckman et al 2005; Taylor & Poston, 2007) Fetal environment either nutritionally deprived or over-rich increases risk for child and adult obesity and its sequelae (Catalano, 2003; Oken & Gillman, 2003; Ehrenberg et al., 2004)
 Fetal undernutrition associated with adult obesity, CVD and type II diabetes (Law et al., 1992; Sayer et al., 2004) Fetal undernutrition + rapid catch-up growth (Ong, 2006; Stettler et al., 2003, 2005) Thrifty phenotype (Hales & Barker, 2001) Adaptive response for deprived pretnatal environment maladaptive for postnatal environment. Developmental Origins of Adult Health and Disease (DOHaD) (Gluckman et al 2005; Taylor & Poston, 2007) Fetal environment either nutritionally deprived or over-rich increases risk for child and adult obesity and its sequelae (Catalano, 2003; Oken & Gillman, 2003; Ehrenberg et al., 2004)")
6
Barker Hypothesis Based on medical archives from Preston, Hertfordshire, and Sheffield, England 16,000 men and women born in Hertfordshire, : ● 2-fold increase in coronary heart disease from largest to smallest BW ● Impaired GT increased from 14% to 40% Barker, et al Clin Sci 1998; 115:118

7
Death Rates From Coronary Artery Disease According to Birthweight

8
Prevelance of Type II DM and Impaired Glucose Tolerance in Men Age 59-70

9
The Nurses Health Study
● 121,701 RNs aged yrs, followed since 1976 ● BW self-reported, validated by birth certificate Rich-Edwards, et al BMJ 1997; 315:396

10
The Nurses Health Study
CAD MI Stroke < 2269 g 1.32 1.29 2.29 g 1.15 0.95 1.38 g 1.02 0.92 1.25 g (ref) g 0.99 ≥ 4537 g 0.68 0.66 Rich-Edwards, et al BMJ 1997; 315:396
 g ≥ 4537 g Rich-Edwards, et al. BMJ 1997; 315:396.")
11
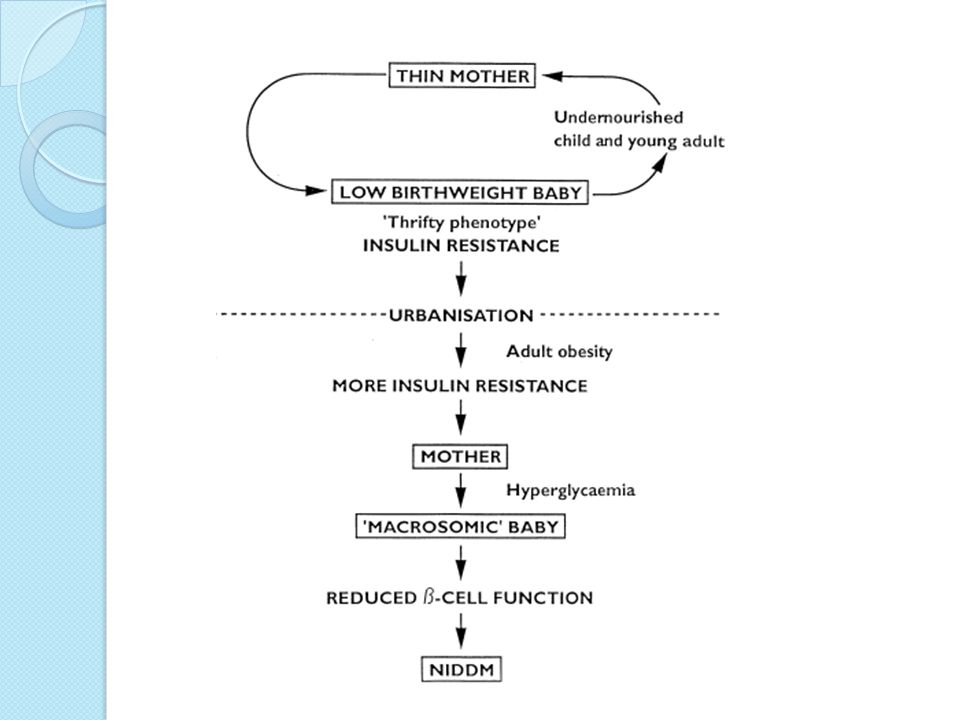
Thrifty Phenotype Hypothesis
During periods of starvation, the fetus reduces insulin secretion, and increases peripheral insulin resistance, thus directing more glucose to the brain and heart, and less to skeletal muscle, etc. Hales and Barker Diabetologica 1992; 35: 595

13
What happens inside matters outside
Antenatal stress associated with: Decreased cognitive function Quebec Ice Storm loss of electricity & water for up to 5 weeks Children had lower MDI scores Lower language development scores These held when controlling for Ob complications, birth weight , post partum depression (LaPlante et al, 2004) Maternal exposure to traumatic events associated with: Schizophrenia (OR – 1.5 in cohort from Dutch famine) Depression in adulthood
 Maternal exposure to traumatic events associated with: Schizophrenia (OR – 1.5 in cohort from Dutch famine) Depression in adulthood.")
14
Chinese Famine Rate of Schizophrenia
Year of birth Adjusted risk P 1959 0.89 ( ) 0.13 1960 2.30 ( ) <0.001 1961 1.93 ( ) 1962 0.95 ( ) 0.28 Proportion of familial cases unchanged (17-18%) St. Clair, et al JAMA 2005; 294:557
 ( ) < ( ) ( ) Proportion of familial cases unchanged (17-18%) St. Clair, et al. JAMA 2005; 294:557.")
15
Childhood behaviors – Mom’s input
In pregnant women in the top 15% of symptoms of anxiety at 32 weeks Children had double the risk of behavioral problems at age 4 and 7 Higher risk for ADHD, depression or conduct disorders Attributable risk may be as high as 15% If true – economic consequences for special education and even incarceration are stunning annual societal ‘‘cost of illness’’ for ADHD is estimated to be between $36 and $52 billion – prenatal stress accounting for $5-7 billion per year

16
Pay attention Oklahoma!

17
How? Epigenetic modifications represent a potential way that “metabolic programming” occurs Alteration in the hypothalamic-pituitary-adrenal axis involving: Mobilizing energy stores Response to stress Inhibiting inflammatory responses during stress Post natal stress is cumulative with prenatal stress leading to increased vulnerability to stressors Prenatal stress can lead to impaired fetal growth Attention disorders and increased anxiety observed

18
Metabolic “Programming” via Genetic Imprinting
● Imprinting turns gene off ● Gene dosage effect- only one gene operational ● Some imprinting reflects gender of transmitting parent ● Many imprinted genes involve metabolism i.e. Igf 2 , Igf 2r, H19

20
Programmed to be ill?

21
Tulsa - We’re Number 1!! Statistics published in Newsweek
Tulsa, Oklahoma Smokers: 24.6% Cigarettes per day: Tried to quit with gum: 26.9% Tried to quit with patch: 32.8% Tried to quit with support program: 7.4%

22
Smoking in Pregnancy Decreased fetal growth Increase in Preterm Birth
Increase in placental abruption

24
Children Born with IUGR (< 2.5K):
↓ Nephron number Fewer glomeruli ↓ Renal volumes Adult glomeruli : 1,400,000 / kidney in controls 700,000 / kidney in HTN Rostand Nephol Dial Transplant 2003; 18:1434

25
Smoking effects Children exposed to tobacco prenatally:
Decreased memory skills at age 6 Deficits in auditory processing Effects more pronounced then children who were exposed prenatally only to marijuana smoking (those children have decreased “executive function”)
")
26
Alcohol Fetal Alcohol Syndrome – associated with 6 or more drinks per day Leads to neurologic impairment Post natal growth restriction Microcephaly

27
Alcohol – other effects
alcohol ingestion during pregnancy represents a risk factor in terms of later alcohol-related problems in offspring hypothesis that low to moderate levels of maternal ethanol intoxication during late pregnancy set the opportunity for fetal learning about ethanol

28
Meth exposure Meth-exposed children scored lower on measures of visual motor integration, attention, verbal memory and long-term spatial memory children exposed to Meth prenatally exhibit smaller subcortical volumes

29
Maternal Obesity Higher rates of macrosomia
Higher rates of pregnancy induced hypertension Higher rates of Gestational Diabetes (a precursor for Type 2 DM)
")
30
DULCE Program Provides culturally competent group prenatal care for Diabetic mothers Education emphasizes diet and life style changes (i.e. just a 20 minute walk a day can smooth out blood sugars) Teaches self reliance in managing DM Early review of findings shows a decrease in LGA babies in the Group prenatal care as compared to traditional care
 Teaches self reliance in managing DM. Early review of findings shows a decrease in LGA babies in the Group prenatal care as compared to traditional care.")
31
SUMMARY ●The intrauterine environment exerts a permanent influence on postnatal metabolism and growth ●The mother’s fetal life can affect the development of her own offspring ●Influential factors include calories, content of diet, micronutrients, stressors

32
Welcome to your childhood…

33
Poverty, children and health: Oklahoma

34
Two complementary theories
Critical periods (latency model) Barker hypothesis Organogenesis Fewer beta cells in pancreas – type 2 diabetes Fewer nephrons - hypertension Cumulative experiences (pathways model) Allostasis and allostatic load Behavioral responses
 Barker hypothesis. Organogenesis. Fewer beta cells in pancreas – type 2 diabetes. Fewer nephrons - hypertension. Cumulative experiences (pathways model) Allostasis and allostatic load. Behavioral responses.")
35
Accumulation of insults
Poverty and health Childhood SES Critical periods Adult SES Accumulation of insults Childhood health Adult health Conroy K et al. JDBP 2010;31:

36
Allostasis and Allostatic Load
The stress response and development of allostatic load are illustrated. Perception of stress is influenced by one’s experiences, genetics, and behavior. When the brain perceives an experience as stressful, physiologic and behavioral responses are initiated leading to allostasis and adaptation. Over time, allostatic load can accumulate, and the overexposure to neural, endocrine, and immune stress mediators can have adverse effects on various organ systems, leading to disease. McEwen 1998

37
Let’s look at that again

38
Adverse Childhood Experiences (ACE) study
Felitti V, Anda R et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. Am J Prev Med 1998;14: 9,508 Kaiser-Permanente adults 7 categories of childhood exposure Abuse: psychological, physical, sexual Dysfunction: substance abuse, mental illness, domestic violence, criminality 10 health risk factors Smoking, obesity, inactivity, depressed mood, suicide attempts, alcoholism, drug abuse, parenteral drug abuse, >50 sexual partners, history of STDs. Disease conditions: Ischemic heart disease, cancer, stroke, COPD, diabetes, hepatitis, skeletal fractures, general health rating

39
ACE results Childhood stressors linked to adult health risk behaviors
Childhood stressors linked to disease conditions (OR) diabetes (1.6), COPD (3.9), fractures (1.6), hepatitis (2.3), self-rated poor health (2.2) Strong dose-response relationship between number of childhood stressors and each of 10 behavioral RFs (p<.05) and for heart disease, cancer, COPD, hepatitis, fractures, poor self-rated health (not for stroke or diabetes). Risk Factors Stressors >4 56% 1% 14% 7%
 diabetes (1.6), COPD (3.9), fractures (1.6), hepatitis (2.3), self-rated poor health (2.2) Strong dose-response relationship between number of childhood stressors and each of 10 behavioral RFs (p<.05) and for heart disease, cancer, COPD, hepatitis, fractures, poor self-rated health (not for stroke or diabetes). Risk Factors. Stressors. >4. 56% 1% 14% 7%")
40
More recent follow-up At least 1 ACE was reported by 64% of respondents. For persons with ≥ 4 ACEs, the risk of panic reactions, depressed affect, anxiety, and hallucinations were increased 2.5-, 3.6-, 2.4 and 2.7-fold, respectively The mean number of comorbid outcomes in the study sample was 2.1 (range: 0–14); means are adjusted for age, sex, race, and educational attainment. The trend in the means is significant (P<0.0001); vertical error bars represent 95% confidence intervals Anda et al Eur Arch Psychiatry Clin Neurosci (2006) 256 : 174–186
; means are adjusted for age, sex, race, and educational attainment. The trend in the means is significant (P<0.0001); vertical error bars represent 95% confidence intervals. Anda et al Eur Arch Psychiatry Clin Neurosci (2006) 256 : 174–186.")
41
Implications of ACE Study
“Clearly, further research and training are needed to help medical and public health practitioners understand how social, emotional, and medical problems are linked throughout the lifespan. Such research and training would provide physicians with the confidence and skills to inquire and respond to patients who acknowledge these types of childhood exposures. The magnitude of the difficulty of introducing the requisite changes into medical and public health research, education, and practice can be offset only by the magnitude of the implications that these changes have for improving the health of the nation.” Felitti et al.. Am J Prev Med 1998;14:

42
Health and stress in Tulsa families
Tulsa Educare – 2 sites Yearly parent interviews at Child’s health “What happened to you last year” – 18 items 247 parents Interviews conducted by family support specialists Data analyzed for links to child health Health issues Allergies Asthma Eczema Obesity (0) 4 categories of stressors Financial Relationship ACE Life Changes
 4 categories of stressors. Financial. Relationship. ACE. Life Changes.")
43
Preschool health by demographics
Total No health issue At least one health issue X2 p Gender 1.6 0.211 Male 141 (57.1%) 101 (59.8%) 40 (51.3%) Female 106 (42.9) 68 (40.2%) 38 (48.7) Age: M (SD) 2.5 (1.2) 2.5 (1.3) 2.3 (1.1) 1.1 0.255 Race 22.0 <0.001 White 27 (10.9%) 17 (10.1%) 10 (12.8%) Black 94 (38.1%) 50 (29.6%) 44 (56.4%) Biracial 17 (6.9%) 11 (6.5%) 6 (7.7%) Other* 109 (44.1%) 91 (53.8%) 18 (23.1%) Ethnicity 15.4 Hispanic 105 (42.5%) 86 (50.9%) 19 (24.4%) Non-Hispanic 142 (57.5%) 83 (49.1%) 59 (75.6%) *95 of the 105 Hispanic parents selected race as “other”
 101 (59.8%) 40 (51.3%) Female. 106 (42.9) 68 (40.2%) 38 (48.7) Age: M (SD) 2.5 (1.2) 2.5 (1.3) 2.3 (1.1) Race < White. 27 (10.9%) 17 (10.1%) 10 (12.8%) Black. 94 (38.1%) 50 (29.6%) 44 (56.4%) Biracial. 17 (6.9%) 11 (6.5%) 6 (7.7%) Other* 109 (44.1%) 91 (53.8%) 18 (23.1%) Ethnicity Hispanic. 105 (42.5%) 86 (50.9%) 19 (24.4%) Non-Hispanic. 142 (57.5%) 83 (49.1%) 59 (75.6%) *95 of the 105 Hispanic parents selected race as other")
44
Family stress and child health
81% of healthy children had at least one stressor (M=2.6 [SD=2.4]) 95% of children with a health problem had at least one stressor (M=3.5 [SD=2.3]) (all p values < 0.05)
 95% of children with a health problem had at least one stressor (M=3.5 [SD=2.3]) (all p values < 0.05)")
45
Health problem by stress category
Children with asthma, allergies and eczema were more likely to have experienced a family stress in the past year Children with health problems were more likely to have stressors from multiple categories (2.1) than healthy children (1.5)
 than healthy children (1.5)")
46
Tulsa Children’s Project
Based at Tulsa Educare Community-based participatory research Multiple partners Interdisciplinary design Highly integrated set of interventions Funded by George Kaiser Family Foundation

47
TCP Partners TCP Annie Van Hanken Monica Basu GKFF Harvard CDC
UT-Austin OU SCM OU Educ OU SW FCS Tulsa Educare Jack Shonkoff Bill Beardslee Snow, Yoshikawa Chris King Bob Glover Jennifer Hays-Grudo Jerry Root Juell Homco Diane Horm, Lisa Monroe Julie Miller-Cribbs Natalie O’Reilley Trishia Pratt Candice Weed Ruth Slocum Elizabeth Miranda Caren Calhoun, Vicki Wolfe Master Teachers

48
Intervention Model Current Situation Short-term outcomes
Children prepared to succeed in school (foundation for life-long success) Low-income families Children (0-5) enrolled in Tulsa Educare Education Medical Home Nutrition Physical activity Early Childhood Education Health Healthy Competent Children in Healthy Competent Families Social- Emotional Health Low-opportunity communities EduCareers: Adult Education and Workforce Training Parents actively improving their own & their children’s life circumstances Re the intervention component, I made a distinction between education and health care on the one hand and mental health and economic security on the other. It seems to me that we have two components with a geographic center of gravity (high quality education and good health care) and two modifier-type variables (good mental health/psychosocial functioning and economic security). Economic security Reduction in inter-generational poverty Current Situation Short-term outcomes Long-term outcome Intervention
 Low-income families. Children (0-5) enrolled in Tulsa Educare. Education. Medical Home. Nutrition. Physical activity. Early Childhood Education. Health. Healthy Competent Children in Healthy Competent Families. Social- Emotional Health. Low-opportunity communities. EduCareers: Adult Education and Workforce Training. Parents actively improving their own & their children’s life circumstances. Re the intervention component, I made a distinction between education and health care on the one hand and mental health and economic security on the other. It seems to me that we have two components with a geographic center of gravity (high quality education and good health care) and two modifier-type variables (good mental health/psychosocial functioning and economic security). Economic security. Reduction in inter-generational poverty. Current Situation. Short-term outcomes. Long-term outcome. Intervention.")
49
Integrated components
Improve quality of classroom experience Enhance curriculum and Professional development for teachers and staff Provide opportunities for parents Adult education Workforce training Promote physical health Health promotion for parents and staff Improved access to care through on-site clinic

50
Early Childhood Education
Developed and implemented new curriculum – Catherine Snow from Harvard Graduate School of Education Conducted monthly full or half-day professional development sessions with master teachers and Harvard consultants Assisted teachers in developing plans for improved outdoor play program Expected long-term outcomes: improved language skills in children improved effectiveness in teachers

51
Health and Health Promotion
Dr. Charlie Homer/NICHQ coaching Increased clinic hours Hired bilingual staff Health promotion Weekly yoga & Zumba classes (parents) Bi-monthly yoga classes (staff) Monthly parent nutrition “make and take” classes Monthly health workshops RECESS instructors in class Expected long-term outcomes: Increase utilization of clinic within community Improved health and fitness in Educare community
 Bi-monthly yoga classes (staff) Monthly parent nutrition make and take classes. Monthly health workshops. RECESS instructors in class. Expected long-term outcomes: Increase utilization of clinic within community. Improved health and fitness in Educare community.")
52
EduCareers: adult education and workforce training for parents
Three options for parents: Nursing cohort: 9 Adult Education ESL: 30 GED: 8 Ind’l Career Coaching: 4 Established partnerships: TCC and TTC Workforce Oklahoma Union Public Schools Support meetings, gas cards, incentives, child care Family Literacy class Expected long-term outcomes: Increased earned income/career opportunities in parents Increased educational achievement in both generations

53
Nursing cohort 9 of 9 passed certification exam for CNA
8/9 completing CNA III classes at TCC 7/9 passed first block of LPN classes (Medical Terminology, Anatomy & Physiology 1 and 2) with A averages Will start clinical blocks Fall 2011
 with A averages. Will start clinical blocks Fall")
54
Mental health Expected long-term outcomes:
Emphasized socioemotional development in curriculum Taught teachers to recognize and address parental depression (Bill Beardslee’s program Family Connections) Built relationships with Educare teachers, staff, parents and community Assessed staff perceptions of Educare (physical, socio-emotional safety in variety of contexts) Trained nursing cohort in life skills (building relationships, solving problems, resolving conflict, etc.) Provided additional mental health support for parents and children as appropriate (K. Coon) Expected long-term outcomes: Improve interactions among teachers, parents, peers & children Reduce negative impact of depression on children Reduce staff absences and turnover
 Built relationships with Educare teachers, staff, parents and community. Assessed staff perceptions of Educare (physical, socio-emotional safety in variety of contexts) Trained nursing cohort in life skills (building relationships, solving problems, resolving conflict, etc.) Provided additional mental health support for parents and children as appropriate (K. Coon) Expected long-term outcomes: Improve interactions among teachers, parents, peers & children. Reduce negative impact of depression on children. Reduce staff absences and turnover.")
55
Welcome to your future…

56
tulsa county gini coefficient 2000 median income: $41,666 denmark 24.7
eur. union 31.0 canada 32.1 usa 45.0 oklahoma 46.0 mexico 46.1 tulsa county 47.4 swaziland 50.4 city of tulsa 50.4 peru 52.0 namibia 76.0 Data from the US Census Bureau and the CIA Factbook.

57
Social determinants of health
The World Health Organization Commission defined social determinants of health as the conditions in which people are born, grow, live, work and age, including the health system.” “The structural determinants and conditions of daily life constitute the social determinants of health and are responsible for a major part of health inequities between and within countries” (WHO Commission on Social Determinants of Health, Final Report, 2008). WHO Commission on Social Determinants of Health, final report, 2008.
. WHO Commission on Social Determinants of Health, final report,")
58
Interventions to address SDH
Downloading: what do we know? (health outcomes tied to SDH: education and income) Seeing fresh: what are we not seeing? (programs don’t address root causes, not coordinated) What do we sense is needed? (partners, communication, trust) What are we called we do? (build relationships, develop organic programs) What would it look like? (user friendly, responsive) Let’s try it.
 Seeing fresh: what are we not seeing (programs don’t address root causes, not coordinated) What do we sense is needed (partners, communication, trust) What are we called we do (build relationships, develop organic programs) What would it look like (user friendly, responsive) Let’s try it.")
59
Usual approach to health problems
values governments insurers health care churches Typical Disciplines Clinical medicine Behavioral science Public health Nutrition Exercise science family built environment schools genes behavior Individual To date, efforts to increase health and wellness have been limited to programs that focus on ONE level—usually just a component of one level—at a time. Why? Funding limitations, conceptual limitations Result is a hodge-podge of wellness efforts: some programs that work, some that don’t, no progress in actually improving health status of given set of individuals anywhere. A very inefficient system for improving health of a population. Imagine if space program in the 1960s were allowed to be conducted using the current grant funding mechanisms—peer group committees giving a little money here, a little money there, hoping that the recipients share their information at various academic meetings and in journal articles, with no coordinated effort to pull all the pieces of the enterprise together. physical resources Environment Systems retailers Policy norms workplace Culture school boards regulatory agencies

60
Ecological model of intervention
attitudes government agencies Academic Disciplines Behavioral sciences Clinical medicine Health promotion Education Social work Economics Public health Public policy /law Architecture/ Urban design Marketing & media funders economic environment health care churches physical resources family schools Community partners Individual What is needed is a comprehensive effort to understand the ways that each element supports healthy living and wellness. How? Surest way to understand something is to try to change it. A scientific discipline built around the assumptions that a) healthy lifestyles are essential for good health and quality of life (i.e., even if a pill is developed to improve weight loss, people must move their bodies to have healthy bones, muscles and joints, people must be stimulated intellectually to have good brain function, babies must be held to develop social attachments, etc.) There are no short-cuts to health and wellness AND b) Healthy living must be built in to the fabric of a community in order to make it part of an individual’s lifestyle. Health and wellness will come about when the lifestyles that result in good health are at least as attractive as lifestyles that result in illness. This requires a coordinated, systematic and scientific involvement of all aspects of society. retailers Systems built environment Environment norms Policy school boards Culture values
 healthy lifestyles are essential for good health and quality of life (i.e., even if a pill is developed to improve weight loss, people must move their bodies to have healthy bones, muscles and joints, people must be stimulated intellectually to have good brain function, babies must be held to develop social attachments, etc.) There are no short-cuts to health and wellness. AND. b) Healthy living must be built in to the fabric of a community in order to make it part of an individual’s lifestyle. Health and wellness will come about when the lifestyles that result in good health are at least as attractive as lifestyles that result in illness. This requires a coordinated, systematic and scientific involvement of all aspects of society. retailers. Systems. built environment. Environment. norms. Policy. school boards. Culture. values.")
61
TCP: Highly integrated engagement of community partners with common goals
Educare admin, staff and parents Psychologists & social workers Physicians & mental health Clinical medicine & health promotion Education Social work Economics Public policy /law Architecture/ Urban design Marketing & media built environment churches family economic environment funders attitudes schools Individual health care school boards physical resources values What is needed is a comprehensive effort to understand the ways that each element supports healthy living and wellness. How? Surest way to understand something is to try to change it. A scientific discipline built around the assumptions that a) healthy lifestyles are essential for good health and quality of life (i.e., even if a pill is developed to improve weight loss, people must move their bodies to have healthy bones, muscles and joints, people must be stimulated intellectually to have good brain function, babies must be held to develop social attachments, etc.) There are no short-cuts to health and wellness AND b) Healthy living must be built in to the fabric of a community in order to make it part of an individual’s lifestyle. Health and wellness will come about when the lifestyles that result in good health are at least as attractive as lifestyles that result in illness. This requires a coordinated, systematic and scientific involvement of all aspects of society. vendors government agencies Systems norms Environment Policy Culture
 healthy lifestyles are essential for good health and quality of life (i.e., even if a pill is developed to improve weight loss, people must move their bodies to have healthy bones, muscles and joints, people must be stimulated intellectually to have good brain function, babies must be held to develop social attachments, etc.) There are no short-cuts to health and wellness. AND. b) Healthy living must be built in to the fabric of a community in order to make it part of an individual’s lifestyle. Health and wellness will come about when the lifestyles that result in good health are at least as attractive as lifestyles that result in illness. This requires a coordinated, systematic and scientific involvement of all aspects of society. vendors. government agencies. Systems. norms. Environment. Policy. Culture.")
63
Post-natal nutritional programming
Gluckman & Hanson, 2004

64
Developmental Origins of Adult Health and Disease Hypothesis
From McMillen & Robinson 2005

65
McMillen & Robinson 2005

Similar presentations






 Research: Implications Heather Larkin, MSW, PhD Assistant Professor, University at Albany Thank you to Dr. Vincent.>")
 Childhood poverty is a major problem in the US –Over 22% of children in the US live in poverty as compared to 9% in.>")













 This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau.>")

