Download presentation
Presentation is loading. Please wait.

2
Neurocognitive Outcomes of Radiation Therapy in Children Aaron S. Kusano, SM University of Washington School of Medicine

3
Outline Topic Choice Topic Choice Background/Current Practices Background/Current Practices Studies of Neurocognitive Effects Studies of Neurocognitive Effects Predictive Model Research Predictive Model Research Interventions Interventions Conclusion Conclusion

4
Why this topic? Balancing act of treatment objectives Balancing act of treatment objectives Implications in Patient Counseling/Education, Multidisciplinary Care and follow up Implications in Patient Counseling/Education, Multidisciplinary Care and follow up Increasing survival = increasing long term side effects Increasing survival = increasing long term side effects Challenging research Challenging research –growing body of literature –study design –advancing technology and alternate approaches

5
Background Childhood cancer survivors have changes/difficulties in: Childhood cancer survivors have changes/difficulties in: 1)Attention2)Social Skills 3)Social Competence 4)Internalization5)Externalization 6)Social Isolation 7)Mood and Behavioral Disorders 40-100% of long term brain tumor survivors have some form of cognitive dysfunction 40-100% of long term brain tumor survivors have some form of cognitive dysfunction Glauser TA, Packer RJ: Cognitive deficits in long-term survivors of childhood brain tumors. Childs Nerv Syst 7:2-12, 1991 Schultz et al. Behavioral and Social Outcomes in Adolescent Survivors of Childhood Cancer: A report from the Childhood cancer survivor study.

6
Background Survivors of pediatric brain tumors have lower rates of high school graduation and employment relative to the overall population Survivors of pediatric brain tumors have lower rates of high school graduation and employment relative to the overall population There is fairly consistent evidence of increased neurocognitive morbidity with higher treatment doses and younger age at the time of treatment Hoppe-Hirsch E, Brunet L, Laroussinie F, et al: Intellectual outcome in children with malignant tumors of the posterior fossa: Influence of the field of irradiation and quality of surgery. Childs Nerv Syst 11:340-346, 1995 Kelaghan J, Myers MH, Mulvihill JJ, et al: Educational achievement of long-term survivors of childhood and adolescent cancer. Med Pediatr Oncol 16:320-326, 1988 Suc E et al. Brain tumours under the age of three. The price of survival. A retrospective study of 20 long-term survivors. Acta Neurochir (Wien). 1990;106(3-4):93-8
. 1990;106(3-4):93-8.")
7
Pathophysiology Destruction of oligodendrocytes and endothelial cells Destruction of oligodendrocytes and endothelial cells Microvascular changes Microvascular changes –Endothelial injury leads to toxic reactions –Formation of free radicals –Cell swelling, increased vascular permeability, ischemia, edema and cell death Evident on MRI with white and gray matter changes Evident on MRI with white and gray matter changes

8
Medulloblastoma

9
Epidemiology of Medulloblastoma Embryonal tumor Embryonal tumor ~20% of pediatric CNS tumors ~20% of pediatric CNS tumors Median age at presentation 6 years Median age at presentation 6 years 30-40% of patients have CSF spread at time of diagnosis 30-40% of patients have CSF spread at time of diagnosis 5 year survival rates for children with standard risk medulloblastoma approaches 80% 5 year survival rates for children with standard risk medulloblastoma approaches 80%

10
Medulloblastoma Risk Categories Average Risk (2/3) Average Risk (2/3) –Age>3 years –Resection with < 1.5cm 2 residual –No metastasis High Risk (1/3) High Risk (1/3) –Age<3years –Resection > 1.5cm 2 residual –Metastasis
 Average Risk (2/3) –Age>3 years –Resection with < 1.5cm 2 residual –No metastasis High Risk (1/3) High Risk (1/3) –Age<3years –Resection > 1.5cm 2 residual –Metastasis")
11
Current Practices

12
Categories Standard Risk Standard Risk High Risk High Risk Infants Infants

13
Standard Risk Age > 3 years and Age > 3 years and less than 1.5 cm 2 of residual tumor and less than 1.5 cm 2 of residual tumor and No metastasis No metastasis Treatment Treatment –CSI 23.4 Gy with posterior fossa boost to 54 Gy + vincristine, adjuvant chemo –Event free survival at 4 years+85% (CCG/POG A9961) Packer RH, Goldwein J, Nicholson HS, et al: Treatment of chilcren with medulloblastomas with reduced-dose craniospinal radiation therapy and adjuvant chemotherapy: A children’s Cancer Group Study. J Clin Oncol 17:2127-2136 Grill J, Renaux VK, Bulteau C, et al: Longterm intellectual outcome in children with posterior fossa tumors according to radiation doses and volumes. Int J Radiat Oncol Biol Phys 45: 137-145, 1999

14
High Risk Age < 3 years OR Age < 3 years OR greater than 1.5 cm 2 of residual tumor OR greater than 1.5 cm 2 of residual tumor OR metastatic disease metastatic disease Treatment Treatment –CSI 36-39 Gy with posterior fossa boost to 54Gy + vincristine, adjuvant chemo –POG 9031 demonstrated those with M1 disease had event free survival at 5 years of 65%

15
Infants (<3yo) Surgery intensive chemotherapy is primary treatment Surgery intensive chemotherapy is primary treatment Radiotherapy reserved for salvage therapy Radiotherapy reserved for salvage therapy Worse prognosis Worse prognosis –Lower rate of complete resection –Higher rates of leptomeningeal seeding at diagnosis
 Surgery intensive chemotherapy is primary treatment Surgery intensive chemotherapy is primary treatment Radiotherapy reserved for salvage therapy Radiotherapy reserved for salvage therapy Worse prognosis Worse prognosis –Lower rate of complete resection –Higher rates of leptomeningeal seeding at diagnosis")
16
Cognitive Measurement

17
Wide Range Achievement Test (WRAT) Ability to Ability to –Read words –Comprehend sentences –Spell –Math calculations
 Ability to Ability to –Read words –Comprehend sentences –Spell –Math calculations")
18
Weschler Intelligence Scale Full Scale IQ Full Scale IQ Indices Indices –Verbal Comprehension (vocab, comprehension) –Perceptual Reasoning (block design, picture concepts) –Processing Speed (timed coding activities) –Working Memory (repeating codes, sequences)
 –Perceptual Reasoning (block design, picture concepts) –Processing Speed (timed coding activities) –Working Memory (repeating codes, sequences)")
19
DSM-IV Criteria based on IQ Scores 50-55 to 70: Mild Mental Retardation 50-55 to 70: Mild Mental Retardation 35-40 to 50-55: Moderate Mental Retardation 35-40 to 50-55: Moderate Mental Retardation 20-25 to 35-40: Severe Mental Retardation 20-25 to 35-40: Severe Mental Retardation 20-25 and below: Profound Mental Retardation 20-25 and below: Profound Mental Retardation

20
Mulhern(1998)- Neuropsychologic functioning of survivors of childhood medulloblastoma POG 8631/CCG923 POG 8631/CCG923 Treatment of average risk medulloblastomas Treatment of average risk medulloblastomas Hypothesis Hypothesis –Children treated with lower initial radiation levels would experience less intellectual toxicity than those receiving higher levels –Also younger subjects suspected to have poorer outcome Mulhern RK, Kepner JL, Thomas PR, et al: Neuropsychologic functioning of survivors of childhood medulloblastoma randomized to receive conventional or reduced-dose craniospinal irradiation: A Pediatric Oncology Group study. J Clin Oncol 16:1723-1728, 1998

21
Mulhern et al (1998) Randomized to 36Gy or 23.4Gy craniospinal radiation Randomized to 36Gy or 23.4Gy craniospinal radiation Both groups receiving boost to 54 Gy to posterior fossa Both groups receiving boost to 54 Gy to posterior fossa Patient’s received baseline testing Patient’s received baseline testing Surviving patients in 1996 with no progressive disease were eligible for study Surviving patients in 1996 with no progressive disease were eligible for study
 Randomized to 36Gy or 23.4Gy craniospinal radiation Randomized to 36Gy or 23.4Gy craniospinal radiation Both groups receiving boost to 54 Gy to posterior fossa Both groups receiving boost to 54 Gy to posterior fossa Patient’s received baseline testing Patient’s received baseline testing Surviving patients in 1996 with no progressive disease were eligible for study Surviving patients in 1996 with no progressive disease were eligible for study")
22
Groupings Young (Y): Age < 9 years Young (Y): Age < 9 years Old (O): Age > 9 years Old (O): Age > 9 years Standard dose radiation (SRT): 36 Gy Standard dose radiation (SRT): 36 Gy Reduced Dose (RRT): 23.4 Gy Reduced Dose (RRT): 23.4 Gy Predicted trend of scores: Predicted trend of scores: –Y/SRT < Y/RRT < O/SRT < O/RRT
: Age < 9 years Young (Y): Age < 9 years Old (O): Age > 9 years Old (O): Age > 9 years Standard dose radiation (SRT): 36 Gy Standard dose radiation (SRT): 36 Gy Reduced Dose (RRT): 23.4 Gy Reduced Dose (RRT): 23.4 Gy Predicted trend of scores: Predicted trend of scores: –Y/SRT < Y/RRT < O/SRT < O/RRT")
23
Subjects Of 35 eligible participants, only 22 patients completed follow up testing Of 35 eligible participants, only 22 patients completed follow up testing –Wechsler Scales of Intelligence –Wide Range Achievement Test III Age 4.1-19.0 years (median 8.85) Age 4.1-19.0 years (median 8.85) 13 treated with SRT, 9 treated w/ RRT 13 treated with SRT, 9 treated w/ RRT
 Age years (median 8.85) 13 treated with SRT, 9 treated w/ RRT 13 treated with SRT, 9 treated w/ RRT")
24
Mulhern et al (1998)
")
29
Conclusions Predicted ordering of distributions was seen for Performance IQ, Full Scale and Attention Index Predicted ordering of distributions was seen for Performance IQ, Full Scale and Attention Index Unable to confirm significant differences in IQ change as a function of age or dose Unable to confirm significant differences in IQ change as a function of age or dose Distribution of scores was in the ordered direction for Reading and Arithmetic Distribution of scores was in the ordered direction for Reading and Arithmetic –12/22 subjects were receiving or had received special educations services with similar proportions in each treatment group

30
Limitations Small numbers, low power, dichtomization of continuous variables Small numbers, low power, dichtomization of continuous variables No longitudinal analysis No longitudinal analysis

31
Studies of Neurocognitive Decline

32
Question What is the pattern of neurocognitive loss? What is the pattern of neurocognitive loss? Loss vs. lack of gain vs. both? Loss vs. lack of gain vs. both?

33
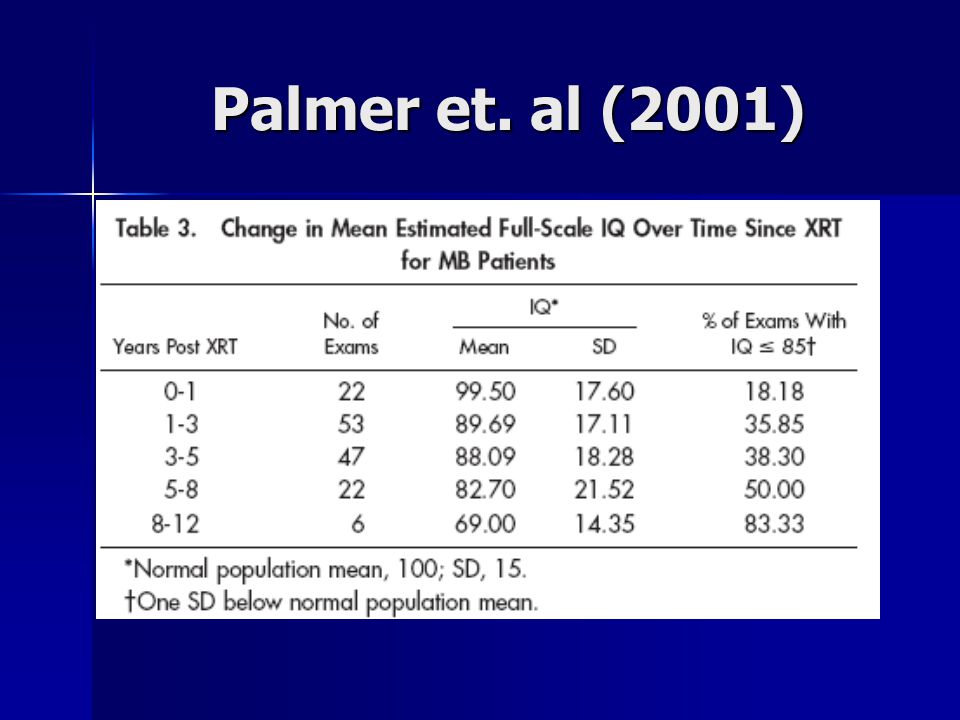
Palmer et al. ( 2001 )- Patterns of Intellectual Development Among Survivors of Pediatric Medulloblastoma: A Longitudinal Analysis Children could lose previously acquired information and skills, similar to adult dementia conditions Children could lose previously acquired information and skills, similar to adult dementia conditionsOR Children could continue to acquire new information and skills but at a slower rate than healthy age-related peers Children could continue to acquire new information and skills but at a slower rate than healthy age-related peers Palmer et al. ( Patterns of Intellectual Development Among Survivors of Pediatric Medulloblastoma: A Longitudinal Analysis Journal of Clinical Oncology, Vol 19, No 8 (April 15), 2001: pp 2302-2308
- Patterns of Intellectual Development Among Survivors of Pediatric Medulloblastoma: A Longitudinal Analysis Children could lose previously acquired information and skills, similar to adult dementia conditions Children could lose previously acquired information and skills, similar to adult dementia conditionsOR Children could continue to acquire new information and skills but at a slower rate than healthy age-related peers Children could continue to acquire new information and skills but at a slower rate than healthy age-related peers Palmer et al. ( Patterns of Intellectual Development Among Survivors of Pediatric Medulloblastoma: A Longitudinal Analysis Journal of Clinical Oncology, Vol 19, No 8 (April 15), 2001: pp")
34
Palmer et. al (2001) 44 Patients 44 Patients –Histologically confirmed MB before age 17 –More than 1 psychological follow up with testing –No evidence of progressive disease CSI Dosages CSI Dosages –33 treated with 35.2-38.4 –7 treated with 23.4-25Gy –4 treated with >40Gy All received posterior fossa boost 49.2-55.8 All received posterior fossa boost 49.2-55.8
 44 Patients 44 Patients –Histologically confirmed MB before age 17 –More than 1 psychological follow up with testing –No evidence of progressive disease CSI Dosages CSI Dosages –33 treated with –7 treated with Gy –4 treated with >40Gy All received posterior fossa boost All received posterior fossa boost")
35
Median 3 examinations per patient Median 3 examinations per patient Age Range at treatment: 1.73-12.88 (mean 7.84) Age Range at treatment: 1.73-12.88 (mean 7.84) Years since XRT: 1.9-12.6 (mean 5.2) Years since XRT: 1.9-12.6 (mean 5.2) Palmer et. al (2001)
.")
41
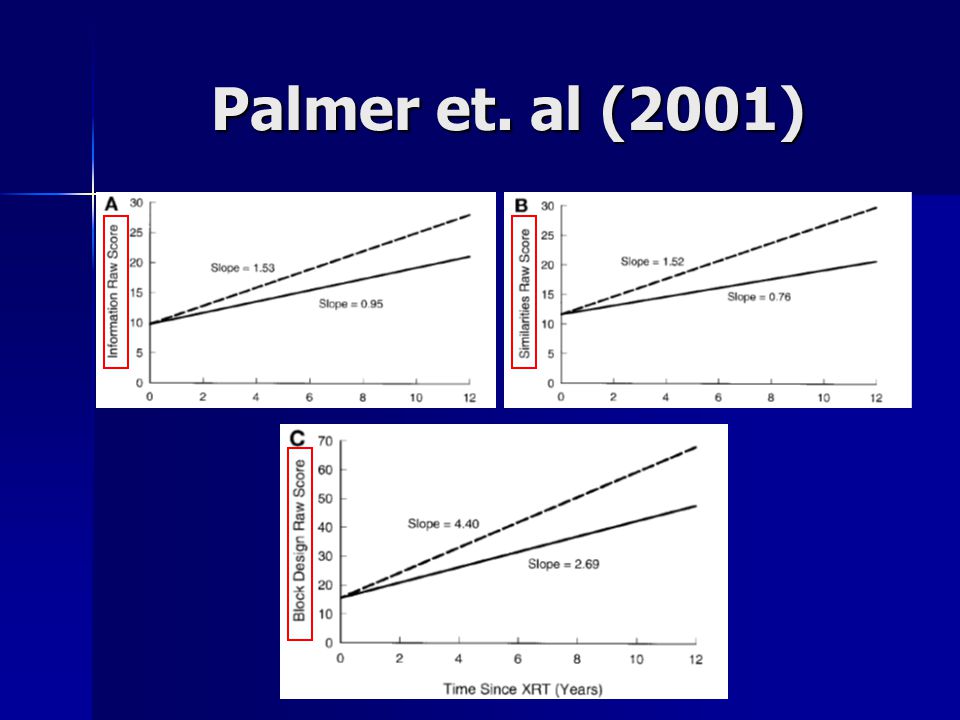
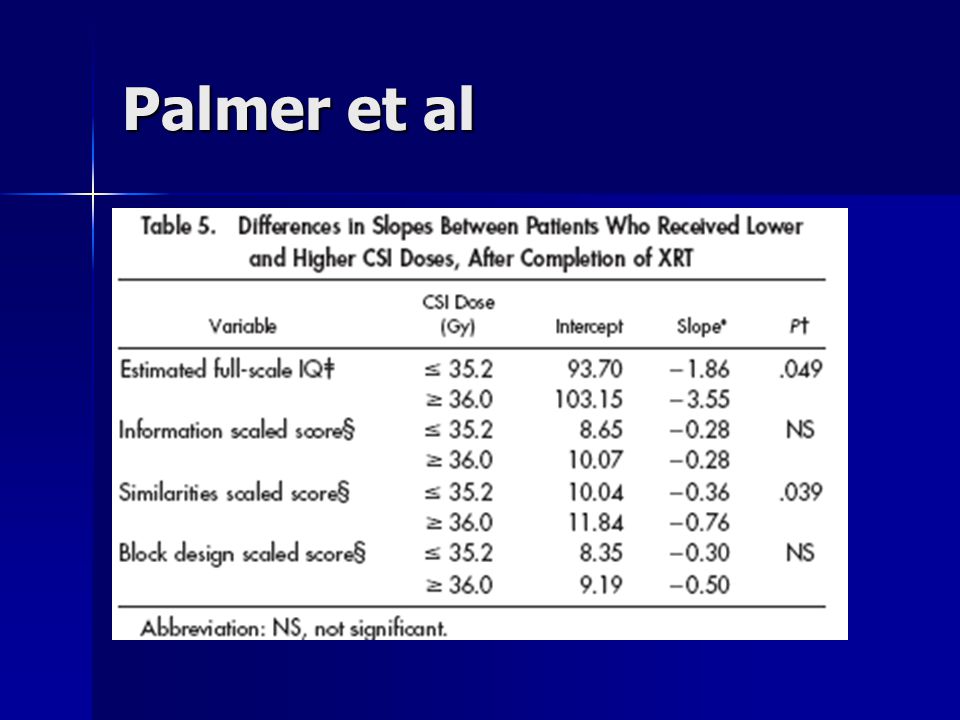
Conclusion of Palmer Paper Declining pattern of functioning over time since completion of XRT Declining pattern of functioning over time since completion of XRT Patients continue to acquire new knowledge but at a fraction of the rate Patients continue to acquire new knowledge but at a fraction of the rate Age at XRT ( 8.02) was an effect modifier Age at XRT ( 8.02) was an effect modifier CSI dose ( 36.0) were significantly different in their effects on IQ CSI dose ( 36.0) were significantly different in their effects on IQ
 was an effect modifier Age at XRT ( 8.02) was an effect modifier CSI dose ( 36.0) were significantly different in their effects on IQ CSI dose ( 36.0) were significantly different in their effects on IQ")
42
As technology changes, can we develop better predictive models for cognitive decline?

43
Merchant et al. (2006) Modelling Radiation Dosimetry to Predict Cognitive Outcomes Some studies had shown no difference in cognitive decline when comparing doses Some studies had shown no difference in cognitive decline when comparing doses –Conventional boost treatments to the entire posterior fossa 40% of the entire brain receiving prescribed dose of 54-55.8 Gy (Mulhern et al 2004) In an effort to reduce radiation dose and volume, attention now focuses on the manner in which the primary site is treated In an effort to reduce radiation dose and volume, attention now focuses on the manner in which the primary site is treated Merchant et al. Modeling Radiation dosimetry to predict cognitive outcomes in pediatric patients with CNS embryonal tumors including medulloblastoma. Int. J. Radiation Oncology bio. Phys. Vol 65, No 1, pp 210-221, 2006
 Modelling Radiation Dosimetry to Predict Cognitive Outcomes Some studies had shown no difference in cognitive decline when comparing doses Some studies had shown no difference in cognitive decline when comparing doses –Conventional boost treatments to the entire posterior fossa 40% of the entire brain receiving prescribed dose of Gy (Mulhern et al 2004) In an effort to reduce radiation dose and volume, attention now focuses on the manner in which the primary site is treated In an effort to reduce radiation dose and volume, attention now focuses on the manner in which the primary site is treated Merchant et al. Modeling Radiation dosimetry to predict cognitive outcomes in pediatric patients with CNS embryonal tumors including medulloblastoma. Int. J. Radiation Oncology bio. Phys. Vol 65, No 1, pp ,")
44
Volume, not just dose SJMB96 trial- Patients treated with 23.4 Gy CSI with conformal posterior fossa radiation to 36 Gy and conformal primary site radiation to 55.8 Gy had IQ decline of 2.4 points per year SJMB96 trial- Patients treated with 23.4 Gy CSI with conformal posterior fossa radiation to 36 Gy and conformal primary site radiation to 55.8 Gy had IQ decline of 2.4 points per year Similar patients treated with 23.4 Gy CSI and conventional posterior fossa radiation to 55.8 Gy had decline of 5.2 IQ points per year Similar patients treated with 23.4 Gy CSI and conventional posterior fossa radiation to 55.8 Gy had decline of 5.2 IQ points per year

45
Goal: Model the effects of the entire distribution of dose to specific volumes of brain on longitudinal IQ after radiation therapy Goal: Model the effects of the entire distribution of dose to specific volumes of brain on longitudinal IQ after radiation therapy Merchant et al. (2006)
.")
46
Patients 39 patients, newly diagnosed embryonal tumors 39 patients, newly diagnosed embryonal tumors –14 average risk (<1.5cm 2 residual, M0) –25 high risk
 –25 high risk")
47
Treatment Avg Risk: 23.4 Gy CSI, conformal posterior fossa boost to 36Gy and conformal primary-site boost to 55.8Gy Avg Risk: 23.4 Gy CSI, conformal posterior fossa boost to 36Gy and conformal primary-site boost to 55.8Gy High Risk: 36-39.6 Gy CSI with conformal primary-site boost to 55.8 Gy. High Risk: 36-39.6 Gy CSI with conformal primary-site boost to 55.8 Gy.

48
Testing Neurocognitive testing performed at Neurocognitive testing performed at –Post surgery –1 year –2 years –5 years

49
Dosimetry Composite Radiation Dosimetry Composite Radiation Dosimetry –Merged 3D CSI dosimetry with 3D Primary site dosimetry Normal volume contours made for Normal volume contours made for –Total (entire) brain –Supratentorial brain –Infratentorial brain –Temporal lobes Dose volume data then extracted Dose volume data then extracted
 brain –Supratentorial brain –Infratentorial brain –Temporal lobes Dose volume data then extracted Dose volume data then extracted")
50
Statistical Analysis Linear Mixed Model with Random Coefficients Linear Mixed Model with Random Coefficients –IQ = dependent variable –Distribution of dose divided into intervals –Covariates Fractional volume receiving dose over specified interval Fractional volume receiving dose over specified interval Age, extent of disease, risk classification Age, extent of disease, risk classification

51
Part 1 Determine effect of dose-volume distribution on the change in IQ score over 5 different volumes of brain tissue Determine effect of dose-volume distribution on the change in IQ score over 5 different volumes of brain tissue –Total Brain –Supratentorial Brain –Infratentorial Brain –Temporal lobes (right and left)
")
52
Example: Total Brain age= years time= months

53
Total Brain Volume Supratentorial Infratentorial

54
Left Temporal Lobe Right Temporal Lobe

55
Mean Dose

56
Supratentorial model application

57
Conclusions of Merchant et al. Prediction of outcomes on basis of CSI dose alone will lose relevance over time Prediction of outcomes on basis of CSI dose alone will lose relevance over time –They’re approach is but one, requiring further validation Limitations Limitations –Assumption of linearity –Limited follow up –Inability to account for other factors that might affect patient outcome

58
So what can we do?

59
Cognitive Remediation Luria-the brain is not a static organ and functional reorganization of neuro pathways can occur after a CNS insult Luria-the brain is not a static organ and functional reorganization of neuro pathways can occur after a CNS insult NIH consensus statement in 1998 supports use of cognitive rehabilitation NIH consensus statement in 1998 supports use of cognitive rehabilitation Educational intervention has been shown to be effective in addressing academic delays in children treated with cranial radiation for ALL Educational intervention has been shown to be effective in addressing academic delays in children treated with cranial radiation for ALL Anderson VA et. Al. Cognitive and academic outcome following cranial irradiation and chemotherapy in children: A longitudinal study. Br J Cancer 82:255-262

60
Ecological Importance of educating patients, caretakers, PCPs and teachers Importance of educating patients, caretakers, PCPs and teachers Classroom accommodations Classroom accommodations Impact of child’s disease on the family Impact of child’s disease on the family

61
Pharmacotherapy Mulhern et al. (2004) study of 83 ALL and BT survivors Mulhern et al. (2004) study of 83 ALL and BT survivors Methylphenidate Methylphenidate –Double blind, 3 week home crossover study –Placebo vs. 0.3mg/kg vs. 0.6mg/kg Compared to placebo, parents and teachers reported attentional and social improvements Compared to placebo, parents and teachers reported attentional and social improvements Ultimate effect on academic achievement? Ultimate effect on academic achievement? Mulhern RK et al. Short-term efficacy of methylphenidate: a randomized, double-blind, placebo-controlled trial among survivors of childhood cancer. J Clin Oncol. 2004 Dec 1;22(23):4795-803
 study of 83 ALL and BT survivors Methylphenidate Methylphenidate –Double blind, 3 week home crossover study –Placebo vs. 0.3mg/kg vs. 0.6mg/kg Compared to placebo, parents and teachers reported attentional and social improvements Compared to placebo, parents and teachers reported attentional and social improvements Ultimate effect on academic achievement. Ultimate effect on academic achievement. Mulhern RK et al. Short-term efficacy of methylphenidate: a randomized, double-blind, placebo-controlled trial among survivors of childhood cancer. J Clin Oncol Dec 1;22(23):")
62
Conclusions Clear association between radiation therapy and cognitive decline Clear association between radiation therapy and cognitive decline Decline appears to be progressive Decline appears to be progressive Continued research with larger sample sizes and validation of predictive models Continued research with larger sample sizes and validation of predictive models Important point to address initially and during follow up Important point to address initially and during follow up

63
Thanks!

64
Additional Slides

65
Palmer et al

67
Ris et al. (2001) Ris et al. (2001) Intellectual Outcome After Reduced-Dose Radiation Therapy Plus Adjuvant Chemotherapy for Medulloblastoma: A Children’s Cancer Group Study Ris et al. (2001) Ris et al. (2001) Intellectual Outcome After Reduced-Dose Radiation Therapy Plus Adjuvant Chemotherapy for Medulloblastoma: A Children’s Cancer Group Study. J Clin Oncol 19:3470-3476.
 Intellectual Outcome After Reduced-Dose Radiation Therapy Plus Adjuvant Chemotherapy for Medulloblastoma: A Children’s Cancer Group Study Ris et al. (2001) Ris et al. (2001) Intellectual Outcome After Reduced-Dose Radiation Therapy Plus Adjuvant Chemotherapy for Medulloblastoma: A Children’s Cancer Group Study. J Clin Oncol 19:")
68
Recently, treatment protocols have been developed to reduce this morbidity. This can be accomplished by simply decreasing the overall dose of RT to the brain or by combining such reductions in RT dose with adjuvant chemotherapy. Such approaches have shown promise in producing survival and tumor recurrence rates comparable to those of conventional therapy Deutsch M, Thomas PR, Krischer J, et al: Results of a prospective randomized trial comparing standard dose neuraxis irradiation (3600 cGy/20) with reduced neuraxis irradiation (2340 cGy/13) in patients with low-stage medulloblastoma: A combined Children’s Cancer Group-Pediatric Oncology Group Study. Pediatr Neurosurg 24:167-177, 1996 Bailey CC, Gnekow A, Wellek S: Prospective randomised trial of chemotherapy given before radiotherapy in childhood medulloblastoma: International Society of Paediatric Oncology (SIOP) and the (German) Society of Paediatric Oncology (GPO)—SIOP II. Med Pediatr Oncol 25:166-178, 1995
 with reduced neuraxis irradiation (2340 cGy/13) in patients with low-stage medulloblastoma: A combined Children’s Cancer Group-Pediatric Oncology Group Study. Pediatr Neurosurg 24: , 1996 Bailey CC, Gnekow A, Wellek S: Prospective randomised trial of chemotherapy given before radiotherapy in childhood medulloblastoma: International Society of Paediatric Oncology (SIOP) and the (German) Society of Paediatric Oncology (GPO)—SIOP II. Med Pediatr Oncol 25: ,")
69
Script your long term side effect discussion for… 7 year old boy, newly diagnosed medulloblastoma 7 year old boy, newly diagnosed medulloblastoma

70
Script your long term side effect discussion for… 7 year old boy, newly diagnosed medulloblastoma 7 year old boy, newly diagnosed medulloblastoma 65 year old woman, newly diagnosed CNS lymphoma 65 year old woman, newly diagnosed CNS lymphoma

71
Pharmacotherapy Meyers et al.- 30 patients with malignant gliomas exhibiting neurobehavioral slowing Meyers et al.- 30 patients with malignant gliomas exhibiting neurobehavioral slowing All patients met the DSM IV criteria for personality change secondary to medical condition All patients met the DSM IV criteria for personality change secondary to medical condition 5 mg of MPH BID and titrated up by 10mg every 2 weeks 5 mg of MPH BID and titrated up by 10mg every 2 weeks Dramatic improvement in psychomotor speed, memory, executive functioning, mood and ADLs were seen even in with progressive disease. Dramatic improvement in psychomotor speed, memory, executive functioning, mood and ADLs were seen even in with progressive disease. Meyers CA, Weitzner MA, Valentine AD, Levin VA. Methylphenidate therapy improves cognition, mood, and function of brain tumor patients. J Clin Oncol. 1998 Jul;16(7):2522-7.
:")
Similar presentations





















 Treated with Anti Vascular Endothelial Growth Factor (VEGF)>")





