Download presentation
Presentation is loading. Please wait.

1
Fluid and Electrolytes in the Critically Ill Peter Gosling PhD FRCPath University Hospital Birmingham NHS Trust ACB South West and Wessex Region Scientific Meeting 12 th July 2005 Clinical Biochemistry in Intensive Care

2
Claude Bernard (1813-1878) ‘ La fixité du milieu intérieur est la condition de la vie libre; ’ Cellular homeostasis Preservation of cellular function Substrate delivery - metabolite removal
 ‘ La fixité du milieu intérieur est la condition de la vie libre; ’ Cellular homeostasis Preservation of cellular function Substrate delivery - metabolite removal")
3
Fluid balance - Normal NaCl 100 N 2 500 Water 2500 ml 390 mosm/L Serum osmolarity 285 mosm/L 1800 100 500

4
Fluid balance: water restriction NaCl 100 N 2 500 Water 2000 700 mosm/L Osmolarity 285 mosm/L 100 500 1000 mL

5
Fluid balance: water loading NaCl 100 N 2 500 ‘Water’ 5000 mL 5000 mL 100 mosm/L Osmolarity 285 mosm/L 100 500 4300 mL

6
Endocrine response to injury: Salt and water retention ADH thirst Water retention Catecholamines vasoconstriction Blood to heart lungs & brain Renin angiotensin II aldosterone Sodium retention Atrial natruietic peptide (Decrease)
")
7
Metabolic response to inflammation Metabolic response to inflammation Proteolysis increased by: Cortisol Tumour necrosis factor IL-1 and IL-6 Glucagon Platelet activating factor Increased urinary nitrogen excretion Sufficient water input required to provide enough urine to excrete solute (Na and urea)
")
8
Urine (Na + K) x 2 plus urea = urine osmolarity
 x 2 plus urea = urine osmolarity")
9
Normal 24 hr fluid and electrolyte balance InputOutput Water2500 mL1800 mL urine 700 mL insensible Sodium100 mmol100 mmol Nitrogen500 mmol500 mmol Other200 mmol200 mmol Total 800 mosmols800 mosmols Urine osmolality 800/1800= 450 mosm/L Urine 40% maximally concentrated

10
Fluid and electrolyte balance 24 hr post major surgery InputOutput Fluid8000 mL1000 mL Urine 1000 mL insensible 1000 mL insensible Sodium1200 mmol50 mmol Nitrogen600 (catabolism) 200 mmol mosmoles4000500 6000 mL positive fluid balance 3500 mosmoles positive balance Requires 7 litres of urine to clear sodium + urea (500 mosm/L maximum concentration)
 200 mmol mosmoles mL positive fluid balance 3500 mosmoles positive balance Requires 7 litres of urine to clear sodium + urea (500 mosm/L maximum concentration)")
12
Post Operative ICU patient N 2 700 mmol (catabolic) Water 500mosm/L Na 50 N 2 400 1000 mL ‘ Normal’ NaCl Colloids Drugs NaCl NaCl 8000 mL NaCl 1200 mmol ‘Sick’ ICU patients often cannot concentrate urine >500 mosm/L
 Water 500mosm/L Na 50 N mL ‘ Normal’ NaCl Colloids Drugs NaCl NaCl 8000 mL NaCl 1200 mmol ‘Sick’ ICU patients often cannot concentrate urine >500 mosm/L")
13
Sodium and chloride overload Sodium and chloride retention Fluid retention Interstital oedema Organ dysfunction – lungs – kidney – gut

14
Concerns about fluid and electrolyte prescribing Hyponatraemia after orthopaedic surgery BMJ 1999;318:1363-64 ‘Appropriateness of fluid regimes’ Variability in post-operative fluid and electrolyte prescription Stoneman et al Br J Clin Pract 1997;51:82-84 ‘Concern about variability in perioperative fluid administration’ Extremes of age: The 1999 report of the National Confidential Enquiry into Perioperative Deaths 1999 Sherry et al. ‘Fluid regimes highlighted’

15
Concerns about fluid and electrolyte prescribing Changes in weight, fluid balance and serum albumin in patients referred for nutritional support Lobo et al Clinical Nutrition 1999;18:197-201 ‘12L mean fluid overload in oedematous patients referred for nutritional support’ Hypernatraemia in the ICU: an indicator of quality of care ? Poldermann et al. Critical Care Medicine 1999;27:1`105-8 ‘Hospital acquired hypernatraemia versus admission hypernatraemia was associated with higher mortality rate’ hypernatraemia was associated with higher mortality rate’

16
Drowning in the brine of an inadequate knowledge base (Lobo et al Clinical Nutrition 2001;20:125-130) PRHOs did 89% the fluid and electrolyte prescribingPRHOs did 89% the fluid and electrolyte prescribing 27% did not know minimum urine 24h output (500- 750 mL) 27% did not know minimum urine 24h output (500- 750 mL) 76% did not know Na + and Cl - content of 0.9% saline (154 mmol/L of each) 76% did not know Na + and Cl - content of 0.9% saline (154 mmol/L of each) 82% did not know Na+daily requirements (60-100 mmol) 82% did not know Na+ daily requirements (60-100 mmol) 98% did not know Na+ content of gelofusine (154mmol/L) 98% did not know Na+ content of gelofusine (154mmol/L) Telephone survey
 PRHOs did 89% the fluid and electrolyte prescribingPRHOs did 89% the fluid and electrolyte prescribing 27% did not know minimum urine 24h output ( mL) 27% did not know minimum urine 24h output ( mL) 76% did not know Na + and Cl - content of 0.9% saline (154 mmol/L of each) 76% did not know Na + and Cl - content of 0.9% saline (154 mmol/L of each) 82% did not know Na+daily requirements ( mmol) 82% did not know Na+ daily requirements ( mmol) 98% did not know Na+ content of gelofusine (154mmol/L) 98% did not know Na+ content of gelofusine (154mmol/L) Telephone survey")
17
Sodium and potassium measurement are our most frequent requests, yet fluid and electrolyte management is poorly understood by medical and nursing staff This is a major challenge for Clinical Biochemistry

18
What are we trying to achieve by giving intravenous fluid ?

19
Fluid Compartments Interstitial fluid 10.5 Litres Blood volume 3.5 litres Cells 28 Litres

20
Fluid shifts in haemorrhage

22
Vasoconstriction & redistribution

23
Fluid shifts in haemorrhage Interstitial fluid mobilisation

24
Fluid shifts in haemorrhage Reduced interstitial fluid

25
Fluid shifts in haemorrhage Intracellular fluid mobilisation

26
Fluid shifts in haemorrhage Reduced intracellular fluid

27
What are we trying to achieve by giving intravenous fluid ? Scenario: Acute blood loss Replacement of RBCs, water and electrolytes - haemostasis

28
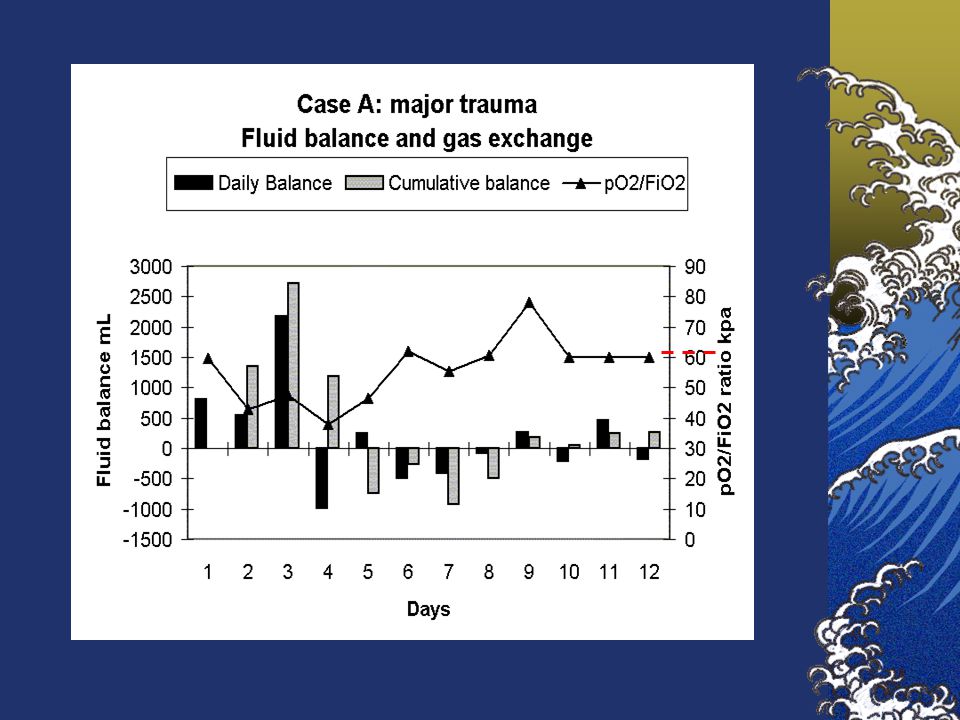
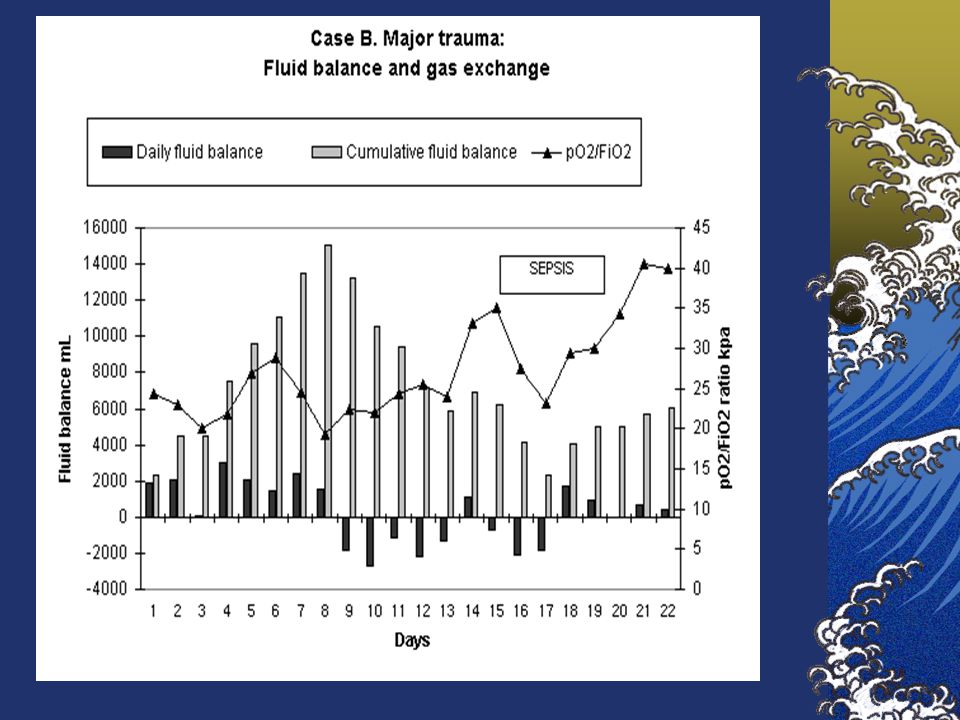
Fluid shifts in trauma, infection, ischaemia-reperfusion injury ‘Inflammation’

29
Fluid shifts in inflammation

30
Fluid shifts in blunt trauma Inflammatory cytokines Neutrophils

31
Fluid shifts in blunt trauma Systemic capillary leak

32
Leak of Water, Na + Cl - Albumin to Interstitium Vasodilatation loss of SVR

33
Hypovolaemia Interstitial oedema

34
Na + Cl Na + Cl -water

35
water

36
Na + and Cl - Loading Fluid retention Severe interstitial oedema Organ dysfunction

37
What are we trying to achieve by giving intravenous fluid ? Scenario: Acute inflammation Blood volume expansion, in the context of vascular dysfunction and leaky capillaries

38
1. Microvascular inflammatory response Two factors influencing choice of fluids

39
Hamster cheek pouch studies Systemic capillary leak to FITC Dextran 150,000 mol wt (Range 10,000 – 500,000) Shearman CP, Gosling P, Simms Br J Surg 1988; 75: 1273 Cheek pouch X 40
 Shearman CP, Gosling P, Simms Br J Surg 1988; 75: 1273 Cheek pouch X 40")
40
Control hamster cheek pouch X40 Following i.v. FITC labelled Dextran 150 kD

41
Cheek pouch 10 mins post laparotomy and chemical peritonitis

42
Cheek pouch 30 mins post laparotomy

43
Scanning EM: normal endothelial cell junction Donald McDonald 1999 X 40,000

44
Scanning EM: 1 minute after substance P

45
Inflammatory mediator release injury

46
Transcapillary escape rate of radiolabelled albumin and serum albumin before and after cardiac bypass surgery Fleck A et al Lancet 1985;I:781-784

47
Capillary leak (microalbuminuria) and inflammatory markers during burns/surgery/trauma Pre op Induct surgery 2h 6h 12h 24h Capillary Leak Interleukin - 6 C-RP SIRS - Organ Failures Normal SIRS – Organ Failures
 and inflammatory markers during burns/surgery/trauma Pre op Induct surgery 2h 6h 12h 24h Capillary Leak Interleukin - 6 C-RP SIRS - Organ Failures Normal SIRS – Organ Failures")
48
2. The effect of the salt and water loading in acute illness Factors influencing choice of fluids

49
Endocrine response to injury: Salt and water retention ADH thirst Water retention Catecholamines vasoconstriction Blood to heart lungs & brain Renin angiotensin II aldosterone Sodium retention Atrial natruietic peptide (Decrease)
")
50
Sodium content of common iv fluids FluidSodiumChloride mmol/L Normal plasma14095 Saline 0.9%154154 Hartmann’s131111 Gelofusine154130 Haemacel145145 4.5% Albumin solution 145145 HAES-steril154154 5% dextrose00 Abnormal !

51
Effects of Saline Loading Hyperchloraemic metabolic acidosis Hyperchloraemic metabolic acidosis Hyperosmolar states Hyperosmolar states Stimulation of ADH - fluid retention Stimulation of ADH - fluid retention Renal vasoconstriction – fluid retention Renal vasoconstriction – fluid retention Nausea, vomiting, abdo pain, hyperventilation, Nausea, vomiting, abdo pain, hyperventilation, headaches, thirst headaches, thirst Hartmann AF, Senn MJE 1932 J Clin Invest 11:337-44 Waters JH et al Anesthesiology 2000:93:1184-7 Williams EL et al Anesthesia & Analgesia 1999;88:999-1003 Skellett S et al. Arch Dis Child 2000;;83:514-6 Healey MA et al J Trauma;45:894-9

53
Normal sodium intake 100 mmol/24h

56
‘Volume therapy should be directed towards maximum effect with minimum sodium, chloride and water loading’ ‘Before a patient can recover they must excrete the water, sodium and chloride given during resuscitation’

57
Properties of resuscitation fluids 0.9 % Abnormal Saline 58 Da Volume expansion lasts 10 mins Massive sodium, chloride and water load Very large volumes required Saline cannot be excreted easily Interstitial oedema

58
Properties of resuscitation fluids 4% Gelatine 30,000 Da Volume expansion lasts 1-2 hours Sodium, chloride and water load Large volume required

59
Properties of resuscitation fluids 4.5% Albumin 68,000 Da Volume expansion lasts 2-4 hours Sodium, chloride and water load Large volume required Normally 60% of albumin is in interstitial space More albumin leaks out during inflammation

60
Properties of resuscitation fluids HES 200,000 Da 0.5 substitution Volume expansion lasts 6-18 h Anti-inflammatory, less capillary leak Compared with crystalloid- only, gelatine or albumin less Na + Cl - and H 2 O

61
40 patients elective AAA Gelatine n = 20 eloHES n = 20 Comparison of Gelatine with eloHES in Aortic Surgery in Aortic Surgery Rittoo et al Br J Surg 2001

62
Lung function during AAA Rittoo et al Brit J Anaesth 2004;92:61-6

63
Capillary leak in AAA patients Medians (Mann Whitney)
")
66
Gastric tonometry during AAA Rittoo D et al.Cardiovasc Surg. 2002;10:128-33.

67
Serum creatinine lower in eloHES and Voluven groups

68
Serum urea lower in eloHES and Voluven groups

69
PRCTs of hydroxyethyl starch for acute volume replacement

70
Recent clinical study Model: 66 elderly (>65y) patients undergoing major abdominal surgery Fluids: Hydroxyethyl starch (130 kD) v Ringers lactate v 0.9% saline Outcome: In starch group 50% less fluid compared with both crystalloid groups. Lower CRP, IL-6 and IL-8 lower ELAM-1 and ICAM Boldt J et al Influence of different volume replacement strategies on inflammation and endothelial activation in the elderly undergoing major abdominal surgery. Intensive Care Med. 2004 Mar;30(3):416-22. Epub 2004 Jan 08.
: Epub 2004 Jan 08..")
71
‘Fluid therapy should be directed not only to effective volume expansion of a leaky circulation but also to microvascular protection’

72
Reasons for fluid therapy Preserve oxygen delivery to tissues Correct hypovolaemia Correct hypovolaemia Maintain cardiac output Maintain cardiac output Optimise gas exchange Optimise gas exchange Replace electrolytes & water Replace electrolytes & water Maintain urine output Maintain urine output Colloids + RBCs Crystalloids Identify what is the goal Choose fluid which best achieves the goal

73
Things to Remember It is very easy to give salt & water to critically ill patients, and very difficult to remove Fluid therapy is often poorly taught, poorly understood and poorly done Sodium and chloride overload is a major problem in critically ill patients Urine electrolyte measurement is essential for fluid management in the critically ill

Similar presentations