Download presentation
Presentation is loading. Please wait.

1
Systemic Lupus Erythematosus

2
Case: A 17-year-old girl was admitted with a chief complaint of recurrent fever for three years, a rash for 2 months, and abdominal pain for 5 days. She had suffered from recurrent high grade fever since 1998, accompanied by “necrotic lymphadenitis”. Her condition had improved with prednisone. Two months earlier, she began to notice fevers, dark-red maculopapules( 斑丘疹), Raynaud‘s pheno- menon (雷诺氏现象), and severe alopecia. At the time, laboratory tests showed ANA 1 ∶ 320 (homogeneous pattern), negative anti- dsDNA, and anti-SSA 1 ∶ 64. She was diagnosed with SLE. Butterfly-erythema ( 蝶状红斑)
, Raynaud‘s pheno- menon (雷诺氏现象), and severe alopecia. At the time, laboratory tests showed ANA 1 ∶ 320 (homogeneous pattern), negative anti- dsDNA, and anti-SSA 1 ∶ 64. She was diagnosed with SLE. Butterfly-erythema ( 蝶状红斑).")
3
What is SLE? SLE is the prototypic autoimmune disease belonging to a family of diseases often referred to as "connective tissue diseases" a term deriving from the observation that the connective tissues of multiple organs were abnormal in these diseases in the absence of obvious infection or neoplasm.

4
Cultural diversity SLE strikes women 10 times as often as men, increasing to 15 times as often during childbearing years( 生育期). It occurs worldwide but is most prevalent among people of Asian, Hispanic, or African origin Population studies have shown an incidence ranging from 2 to 50 cases/100,000 with clear variation according to ethnic group.

5
Causes: The exact cause of SLE remains a mystery, but available evidence points to interrelated immunologic, environmental, hormonal, and genetic factors.

6
TT here is an increased frequency of SLE and asymptomatic immunologic abnormalities in close relatives of SLE patients. MM onozygotic twins (同卵双胞胎). EE thnic differences. CC ertain histocompatibility (组织相容性) antigens (HLA) (e.g.: HLA- DR2, DR3) Genetic factors
. EE thnic differences. CC ertain histocompatibility (组织相容性) antigens (HLA) (e.g.: HLA- DR2, DR3) Genetic factors.")
7
Environmental factors Drug induced lupus: procainamide ( 普鲁卡因胺 ), chlorpromazine ( 精神病药 ) Diet: Nutritional factors may modify disease but this has not been adequately studied. Infectious: Viral and other infectious etiologies. 注射用盐酸氯普鲁卡因

8
Certain related factors: UV radiation (紫外线辐射) Hairdye ( 染发剂) HairdyeSunshine
 Hairdye ( 染发剂) HairdyeSunshine")
9
Skin cell T cell UV light APC External Ag B cell Detective IC clearance and regulatory circuits Self Ag ABIC Ab target IC infection Overview of the pathogenesis of SLE Drugs

10
Immune System Genes Exogenous factor Endogenous factor Estrogen Loss self-tolerance (certain antigen) Androgen B cells T suppressor ↓ T help↑ Cytokines(IL-10) Increased Ab production to “auto-antigen” Auto-antibodies Immune complex formation Poor immune complex clearance Excess immune complex depositionInflammationPathology SLE pathogenesismechanism Humoral ImmunityCellular Immunity Genes C 1 ↓ ; RBC CR1↓ ; MPS phagocytosis↓
 Androgen B cells T suppressor ↓ T help↑ Cytokines(IL-10) Increased Ab production to auto-antigen Auto-antibodies Immune complex formation Poor immune complex clearance Excess immune complex depositionInflammationPathology SLE pathogenesismechanism Humoral ImmunityCellular Immunity Genes C 1 ↓ ; RBC CR1↓ ; MPS phagocytosis↓")
11
Pathophysiology: Autoimmunity is believed to be the prime mechanism involved with SLE. The body produces antibodies against components of its own cells, such as the antinuclear antibody (ANA), and immune complex disease follows. Patients with SLE may produce antibodies against many different tissue components, such as red blood cells, neutrophils, platelets, lymphocytes, or almost any organ or tissue in the body.
, and immune complex disease follows. Patients with SLE may produce antibodies against many different tissue components, such as red blood cells, neutrophils, platelets, lymphocytes, or almost any organ or tissue in the body..")
12
Characteristic pathology change 特征性病理改变 Hematoxylin corpuscle (苏木紫小体) @ @ Onionskin( 洋葱皮样) change, spleen central artery and other arteriescentripetal textile fiber proliferation (向心性纤维增生) @ @ verrucous endocarditis (疣状心内膜炎) @ @ glomerulus fluorescent staining( 荧光染色 ) appears the full house to be bright (满堂亮) @ @
 change, spleen central artery and other arteriescentripetal textile fiber verrucous glomerulus fluorescent staining( 荧光染色 ) appears the full house to be")
13
Main symptoms : Weakness Fever more than 80% of the patients have a fever. Skin and mucosal damage 75 -80% of the patients skin or mucosal damage. Photosensitivity (光过敏) Cheek erythema (颊部红斑) Bullous lupus erythematosus (大疱性红斑狼疮 ) Alopecia (脱发)
 Cheek erythema (颊部红斑) Bullous lupus erythematosus (大疱性红斑狼疮 ) Alopecia (脱发).")
14
Cheek erythema (颊部红斑): First in cheek, suddenly appeared for the small light red, bright red or purple spots, gradually expanded to bridge of the nose, and linked into such as butterflies like grouper. Recurrence of this plaque can happen again.

15
SLE CLINIC FEATURES ( 1 ) GENERAL Lethargy Fever Weight loss Lymphadenopathy DERMATOLOGICAL Vasculitis Alopecia Discoid Panniculitis Photosensitivity MUSCULOSKELETAL Arthralgia/Arthritis Myalgia/Myositis Tenosynovitis GASTROINTESTINAL Anorexia Nausea Abdominal pain Hepato/splenomegaly
 GENERAL Lethargy Fever Weight loss Lymphadenopathy DERMATOLOGICAL Vasculitis Alopecia Discoid Panniculitis Photosensitivity MUSCULOSKELETAL Arthralgia/Arthritis Myalgia/Myositis Tenosynovitis GASTROINTESTINAL Anorexia Nausea Abdominal pain Hepato/splenomegaly")
16
SLE CLINIC FEATURES (2) RENAL@@ Proteinuria Haematuria Casts Nephrotic syndrome CARDIOPULMONARY Shortness of breath Pleurisy Pleural effusion Cardiomegaly Pericarditis CEREBRAL Migraine Anxiety/depression Psychosis Seizures Cranial/Peripheral HEMATOLOGICAL Anemia-iron deficient Anemia-haemolytic Lymphopenia Thrombocytopenia
 Proteinuria Haematuria Casts Nephrotic syndrome CARDIOPULMONARY Shortness of breath Pleurisy Pleural effusion Cardiomegaly Pericarditis CEREBRAL Migraine Anxiety/depression Psychosis Seizures Cranial/Peripheral HEMATOLOGICAL Anemia-iron deficient Anemia-haemolytic Lymphopenia Thrombocytopenia")
18
Diagnosis: Test results that may indicate SLE include complete blood count with differential possibly showing anemia and a decreased white blood cell count platelet count, which may be decreased erythrocyte sedimentation rate, which is often elevated serum electrophoresis, which may show hypergammaglobulinemia.

19
Drugs for SLE Corticosteroids ( 糖皮质激素 ): most commonly used. It can suppress inflammation and are commonly used in controlling SLE. Immunosuppressive Drugs ( 免疫 抑制剂 ): CTX( 环磷酰胺 ), AZA( 硫唑嘌呤 ) IVIG( 丙种球蛋白 ) 免疫抑制剂
: CTX( 环磷酰胺 ), AZA( 硫唑嘌呤 ) IVIG( 丙种球蛋白 ) 免疫抑制剂.")
21
LE cell (狼疮细胞) @ @

22
脾动脉 “ 洋葱皮样 ” 改变 @ @

23
心瓣膜疣状赘生物 @ @

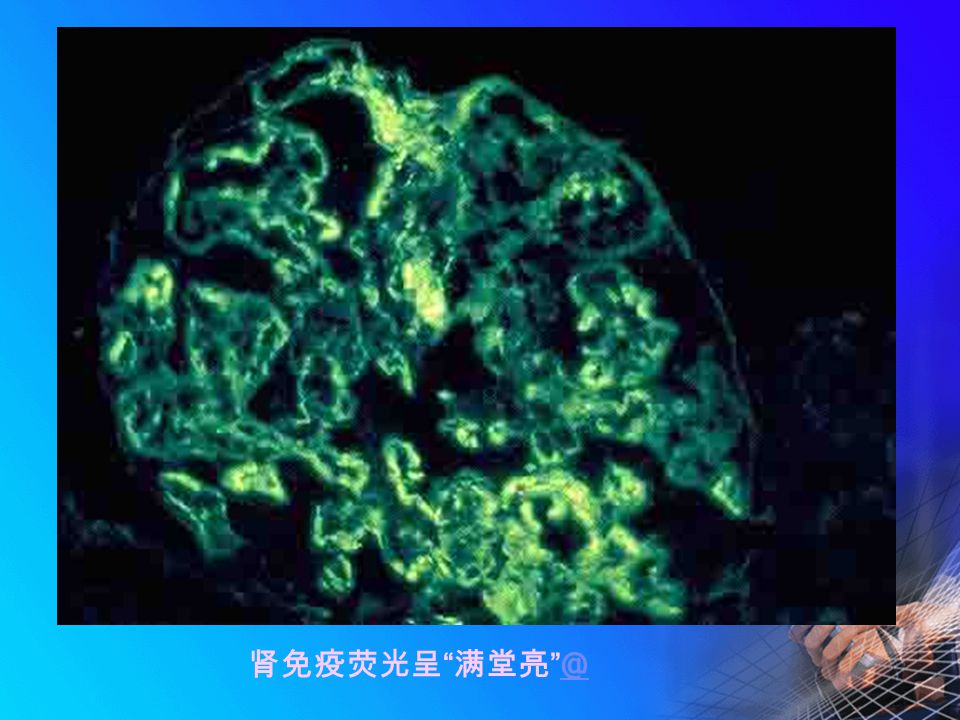
24
肾免疫荧光呈 “ 满堂亮 ” @ @
25
狼疮性肾炎 @ @

26
狼疮性肾炎(系膜型)狼疮性肾炎(膜型) @ @

Similar presentations




>")
. Definition Epidemiology Pathophysiology Clinical features Classification and diagnosis Treatment Prognosis Lupus related syndromes.>")

>")





. 鸡的急性、高度接触传染性的呼吸道疾病。 特征是病鸡咳嗽、喷嚏、气管发生罗音,产蛋 减少、蛋的品质下降。 肾病变型肾肿大、尿酸盐沉积。 腺胃型.>")







