Download presentation
Presentation is loading. Please wait.

1
A HIV free new generation in Central Province, Kenya. VIhDA Association Victorio Torres Feced June 24th 2008 Access Campaign – Experts roundtable Hotel Le Grenil, Geneva

3
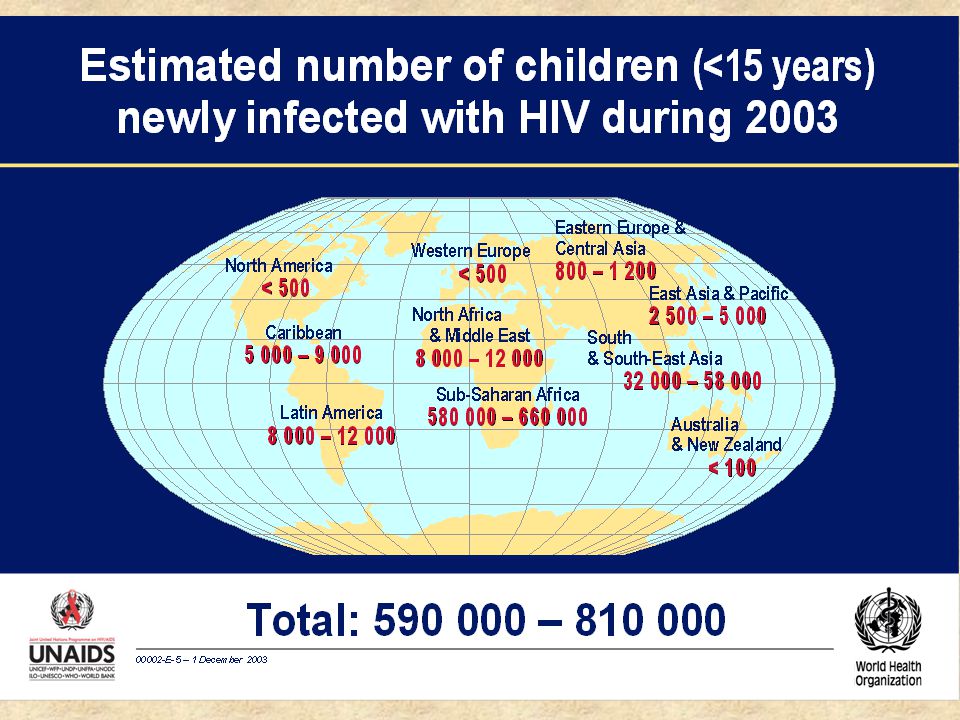
Western & Central Europe200[<400] North Africa & Middle East6900 [3200 – 12 000] Sub-Saharan Africa 470 000 [370 000 – 590 000] Eastern Europe & Central Asia2300 [1400 – 3900] South & South-East Asia 44 000 [23 000 – 75 000] Oceania1100 [400 – 2800] North America500[<1000] Caribbean3700 [2100 – 5800] Latin America5000 [3500 – 8000] East Asia 2300 2300 [1000 – 4100] Total: 540 000 (420 000 – 670 000) Estimated number of children (<15 years) newly infected with HIV, 2005
![Western & Central Europe200[<400] North Africa & Middle East6900 [3200 – ] Sub-Saharan Africa [ – ] Eastern Europe & Central Asia2300 [1400 – 3900] South & South-East Asia [ – ] Oceania1100 [400 – 2800] North America500[<1000] Caribbean3700 [2100 – 5800] Latin America5000 [3500 – 8000] East Asia [1000 – 4100] Total: ( – ) Estimated number of children (<15 years) newly infected with HIV, 2005](http://images.slideplayer.com/13/4075170/slides/slide_3.jpg "Western & Central Europe200[<400] North Africa & Middle East6900 [3200 – ] Sub-Saharan Africa [ – ] Eastern Europe & Central Asia2300 [1400 – 3900] South & South-East Asia [ – ] Oceania1100 [400 – 2800] North America500[<1000] Caribbean3700 [2100 – 5800] Latin America5000 [3500 – 8000] East Asia [1000 – 4100] Total: ( – ) Estimated number of children (<15 years) newly infected with HIV, 2005")
4
Western and Central Europe200[<400] North Africa and Middle East7000 [3300 – 13 000] Sub-saharan Africa 460 000 [360 000 – 580 000] Eastern Europe and Central Asia2800 [1600 – 4700] South and 43 000 [23 000 – 73 000] South East Asia 43 000 [23 000 – 73 000] Oceanía1100 [440 – 2800] North America500[<1000] Caribe2400 [1400 – 3600] Latin America4900 [3500 – 7800] East Asia 2500 2500 [1100 – 4500] Total: 530 000 (410 000 – 660 000) Estimated number of children (<15 years) newly infected with HIV, 2006
![Western and Central Europe200[<400] North Africa and Middle East7000 [3300 – ] Sub-saharan Africa [ – ] Eastern Europe and Central Asia2800 [1600 – 4700] South and [ – ] South East Asia [ – ] Oceanía1100 [440 – 2800] North America500[<1000] Caribe2400 [1400 – 3600] Latin America4900 [3500 – 7800] East Asia [1100 – 4500] Total: ( – ) Estimated number of children (<15 years) newly infected with HIV, 2006](http://images.slideplayer.com/13/4075170/slides/slide_4.jpg "Western and Central Europe200[<400] North Africa and Middle East7000 [3300 – ] Sub-saharan Africa [ – ] Eastern Europe and Central Asia2800 [1600 – 4700] South and [ – ] South East Asia [ – ] Oceanía1100 [440 – 2800] North America500[<1000] Caribe2400 [1400 – 3600] Latin America4900 [3500 – 7800] East Asia [1100 – 4500] Total: ( – ) Estimated number of children (<15 years) newly infected with HIV, 2006")
6
PMTCT national program in Kenya Year 2005 Source: National AIDS Control Council JAPR report 2007 New births1.423.000 HIV infected mothers giving birth64.000 New HIV pediatric infections22.500 Deaths of HIV infected children20.000 Children in need of HAART39.000 Children in need of cotrimoxazole106.000

7
Maragua AIDS care program District population 396,675 - 40% live below poverty line; overall HIV prevalence is 5%. One district hospital, two mission hospitals, five health centres. Two ART initiation sites in the district (the district hospital and one mission hospital), five ART follow up sites. Computerised M+E at the district hospital (FUCHIA MSF-Epicentre®) May 2008: 63,839 people HIV tested since 2002 (4 testing strategies). MOH ART program started in 2004; provides free ARV medications (fixed dose combination) to 2800 patients (15% children).
, five ART follow up sites. Computerised M+E at the district hospital (FUCHIA MSF-Epicentre®) May 2008: 63,839 people HIV tested since 2002 (4 testing strategies). MOH ART program started in 2004; provides free ARV medications (fixed dose combination) to 2800 patients (15% children)..")
8
Roles and responsibilities in the partnership District Health Management Team members: DMoH, DPHN, DTLC, DMLT, DHEO, DAO, DRO, DNO, DPHO, DASCO, Dphar, Medsup.

12
Why investing in optimized replacement feeding (formula +) for mothers opting not to breastfeed in Central Province? It has proved effective in erradicating postnatal pediatric HIV infection in industrialised and middle income countries. Unlike breastfeeding, once RF is AFASS it has no legal implications*. Do infants born to HIV infected mothers have the right of not being breastfed? Breastfeeding is an absolute contraindication if mother is HIV infected in industrialized and middle income countries** How long do we see HIV infected mothers breastfeeding in areas with limited resources? Vision 2030. * Naver et at, J Acquir Immune Defic Syndr 2006;42:484 Y 489 HIV Prevention ACT Penal Code of Kenya section 264 Convention of the Rights of the child: 24(1) article **Nelson textbook of pediatrics. Tropical pediatrics (Oxford University)
 article **Nelson textbook of pediatrics. Tropical pediatrics (Oxford University).")
13
Kenya Health Demographic Survey 2006 (general population): Rates of mothers practising Exclusive Breastfeeding at 6 months : 2,6% Why investing in optimized replacement feeding..?
: Rates of mothers practising Exclusive Breastfeeding at 6 months : 2,6% Why investing in optimized replacement feeding..")
14
Mother to child transmission of HIV-1 infection during exclusive breastfeeding in the first 6 months of life: an intervention cohort study. Coovadia et al. The Lancet 2007; 369:1107-1116.

15
Why investing in optimized replacement feeding..? Is early weaning safe? AFASS? Thomas T, et al Rates of diarrhea associated with early weaning among infants in Kisumu, Kenya. CROI 2007, 14th Conference of Retroviruses and Opportunistic Infections, Los Angeles, California, US, 2007 [abstract 774]. Kourtis A et al. Diarrhea in uninfected infants ofHIV-infectedmothers who stop breastfeeding at 6months: The Ban Study Experience. CROI 2007, 14th Conference of Retroviruses and Opportunistic Infections, Los Angeles, California, US, 2007 [abstract 772]. Kafulafula et al. Postweaning gastroenteritis and mortality in HIV-uninfected African infants receiving ARV prophylaxis to prevent MTCT of HIV-1. CROI 2007, 14th Conference of Retroviruses and Opportunistic Infections, Los Angeles, California, US, 2007 [abstract 773]. Onyango C et al. Early breastfeeding cessation among HIV-exposed negative infants and risk of serious gastroenteritis: findings from a perinatal prevention trial in Kampala, Uganda. CROI 2007, 14th Conference of Retroviruses and Opportunistic Infections, Los Angeles, California, US, 2007 [abstract 775]. Coutsoudis A, Pillay K, Spooner E, Coovadia HM, Pembrey L, Newell M-L. Morbidity in children born to women infected with human immunodeficiency virus in South Africa: does mode of feeding matter? Acta Paediatr 2003; 92:890–895.

16
Abrupt and early weaning is a difficult process. By the time of weaning many women are already lost to follow up.

17
Rates of Gastroenteritis Hospitalizations by Infant Age, Comparing CDC HAART Study (KiBS) with Early Weaning to Natural History Study (VT) in Kisumu, Kenya Age in months Age of Weaning in KiBs ( Mary Glenn Fowler MD)
 with Early Weaning to Natural History Study (VT) in Kisumu, Kenya Age in months Age of Weaning in KiBs ( Mary Glenn Fowler MD)")
18
Fallo en el crecimiento a partir de los 6 meses en el estudio KiBS (N=63) comparado con el estudio VT, sin destete precoz (N=440), Kisumu, Kenya (Mary Glenn Fowler MD)
 comparado con el estudio VT, sin destete precoz (N=440), Kisumu, Kenya (Mary Glenn Fowler MD)")
19
P= 0.27 P= 0.007 Kuhn L et al. N Engl J Med. 2008; 359.

20
Mortality and HIV transmission by Mode Feeding in Randomized Breastfeeding vs Formula-Feeding Clinical Trial, Nairobi, Kenya Nduati R, et al. JAMA 2000;283:1167-74 Breastfed (N=191) Formula-Fed (N=193) 37% (Mortality 24%) 21% (Mortality 20%) Overall rate of breast milk transmission was 16.2%; 75% of occurred by 6 months P=0.001
 Formula-Fed (N=193) 37% (Mortality 24%) 21% (Mortality 20%) Overall rate of breast milk transmission was 16.2%; 75% of occurred by 6 months P=")
21
18-Month Probability of Survival by Feeding Group, ANRS DITRAME 1201/1202 and 049a – Uninfected children Becquet et al. PLoS Medicine. 2007;4:0139-0151 18 month survival 3 mo6 mo12 mo18 mos Ditrame Plus (2001-2005) Short-term breastfed 0.97 0.960.95 Formula 0.98 0.96 Ditrame (1995-1999) Long-term breastfed 0.98 0.970.95 Comparison short-term breast vs formula: p= 0.83 Comparison long-term breast vs combined Ditrame Plus: p= 0.79
 Short-term breastfed Formula Ditrame ( ) Long-term breastfed Comparison short-term breast vs formula: p= 0.83 Comparison long-term breast vs combined Ditrame Plus: p=")
22
18-Month Probability of Survival by Feeding Group, ANRS DITRAME 1201/1202 and 049a – Infected Children Becquet et al. PLoS Medicine. 2007;4:0139-0151 18 month survival 3 mo6 mo12 mo18 mos Ditrame Plus (2001-2005) Short-term breastfed 0.920.780.730.61 Formula 0.910.780.56 Ditrame (1995-1999) Long-term breastfed 0.980.770.520.45 Comparison short-term breast vs formula: p= 0.61 Comparison long-term breast vs combined Ditrame Plus: p= 0.25
 Short-term breastfed Formula Ditrame ( ) Long-term breastfed Comparison short-term breast vs formula: p= 0.61 Comparison long-term breast vs combined Ditrame Plus: p=")
23
Given appropriate nutritional counseling and care, access to clean water and a supply of breast-milk substitutes, these alternatives to prolonged breas-feeding can be safe interventions to prevent MTCT of HIV in urban African setting. Becquet et al. PLoS Medicine. 2007;4:0139-0151. Two year morbidity-mortality and alternatives to prolonged breast-feeding among children born to HIV-infected mothers in Cote d´Ivoire. With appropriate education and access to clean water, formula feeding can be a safe alternative to breast-feeding for infants of HIV-1 infected mothers in resource-poor setting. Nduati R, et al. JAMA 2000;283:1167-74. Morbidity and mortality in breastfed and formula-fed infants of HIV-1-infected women (RCT). Replacement feeding is effective in preventing MTCT and can be implemented in areas with access to safe water (Kayhelitsa, SA). Hilderbrand K, Goemaere E, Coetzee D. The prevention of mother-to-child HIV transmission programme and infant feeding practices. S Afr Med J 2003 October;93(10):779-81. Given appropriate support RF can be safe for HIV infected mothers opting not to breastfeed in resource limited settings…
. Replacement feeding is effective in preventing MTCT and can be implemented in areas with access to safe water (Kayhelitsa, SA). Hilderbrand K, Goemaere E, Coetzee D. The prevention of mother-to-child HIV transmission programme and infant feeding practices. S Afr Med J 2003 October;93(10): Given appropriate support RF can be safe for HIV infected mothers opting not to breastfeed in resource limited settings….")
24
The dilema: It is clear what to do to prevent mother to child transmission of HIV in resource limited settings… the question is how to do it?

27
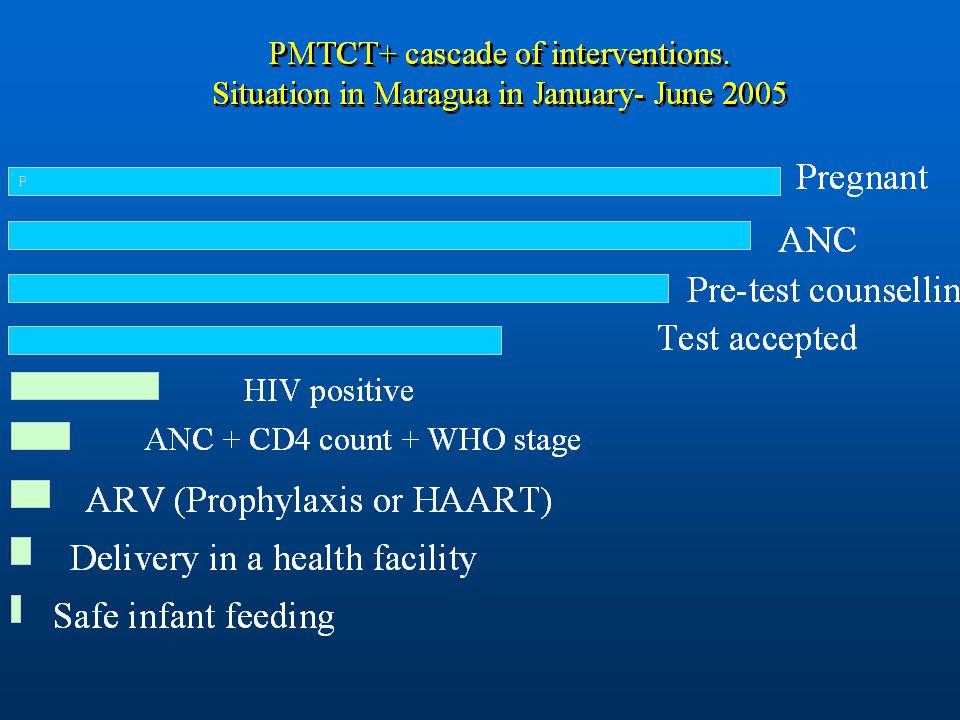
DHMT meeting in June 2005 Challenges identified in comprehensive care for pregnant women and their families: 1.Access to HIV testing: Only 40% of pregnant women (1893 out 4736) are tested for HIV in the 24 ANC clinics in the District. Few ANC nurses trained as HIV counselors and able to prescribe ARV (stigma is also with the Health care worker). 2.Access to HIV comprehensive care: Only 14 out of 82 HIV + pregnant women were registered in comprehensive care clinic (83% of drop out), 8 had a CD4 done (9%), 4 received HAART (4.8%). No clinicians in MCH department. Women droped out from the referral system. No PSS. 3.No M&E system in place to trace mothers sequentially (seen in various departments during pregnancy, delivery, breastfeeding). 4.Infant formula was not available in the MoH system. Early diversification is the cultural norm. 5.No viral tests to monitor overall impact of the intervention.
. 2.Access to HIV comprehensive care: Only 14 out of 82 HIV + pregnant women were registered in comprehensive care clinic (83% of drop out), 8 had a CD4 done (9%), 4 received HAART (4.8%). No clinicians in MCH department. Women droped out from the referral system. No PSS. 3.No M&E system in place to trace mothers sequentially (seen in various departments during pregnancy, delivery, breastfeeding). 4.Infant formula was not available in the MoH system. Early diversification is the cultural norm. 5.No viral tests to monitor overall impact of the intervention..")
28
83% 17%

29
Action plan (June 05) Vision: An HIV free generation by the end of 2006 Motto: As simple as possible with minimal input and maximal output. 1.Training of nurses from MCH in DTC and HAART. 2.Employment of 9 more staff in an initial phase, 12 in a second phase (MoH contracts). 3.Group pretest counseling and Opt out instead of Opt in strategy. 4.Visual teaching aids (flannel graphs) to facilitate understanding of the disease. 5.A vehicle to cover West part of the District on Wednesdays and East part on Thursdays to collect all CD4 samples so pregnant women are not referred to central lab. 6.MCH Nurses to manage women in WHO stage I and II with more than 350 CD4 (prophylaxis with ZDV and NVP). Stage III or IV and CD4<350 are seen by clinician (in the MCH) and receive HAART. 7.Infant formula to be available in Nutrition department 8.DNA-PCR at 6 weeks 9.M2M to provide psyshosocial support and counselling 10.All services are free for HIV + clients including deliveries and hospital bills 11.FUCHIA as the tool to monitor the intervention
. 3.Group pretest counseling and Opt out instead of Opt in strategy. 4.Visual teaching aids (flannel graphs) to facilitate understanding of the disease. 5.A vehicle to cover West part of the District on Wednesdays and East part on Thursdays to collect all CD4 samples so pregnant women are not referred to central lab. 6.MCH Nurses to manage women in WHO stage I and II with more than 350 CD4 (prophylaxis with ZDV and NVP). Stage III or IV and CD4<350 are seen by clinician (in the MCH) and receive HAART. 7.Infant formula to be available in Nutrition department 8.DNA-PCR at 6 weeks 9.M2M to provide psyshosocial support and counselling 10.All services are free for HIV + clients including deliveries and hospital bills 11.FUCHIA as the tool to monitor the intervention.")
30
All pregnant women encouraged to attend ANC in a health facility as soon as possible All pregnant women booking ANC services in a Health facility (levels 2,3,4,5 and 6) are offered HIV testing (opt-out) To all HIV infected pregnant women: computerized file opened, counselling, WHO staging, CD4 count, antenatal profile, LLITN, support groups for every 20 mothers, M2M, NHIF card, nutrition support All HIV infected pregnant women: encouraged to deliver in the hospital, free deliveries for mothers with no NHIF card, mothers on HAART to continue, mothers on AZT receive SD-NVP. All exposed infants SD-NVP + AZT. Intensive counselling for all mothers, especially those tested intrapartum (M2M). CD4 count < 350: HAART, prophylaxis and treatment of OI CD4 count > 350: AZT from 28 weeks, prophylaxis and treatment of OI. SD- NVP adding (AZT+3TC for 3 days) Mothers who opt TO breastfeed Exclusive breastfeeding (EBF) for 6 months or as long as the mothers can manage, then supported weaning with infant formula, counselling and safe water kit. Supply of infant formula up to 1 year of age then discharged Computerized file opened with multiple variables DNA-PCR at 6 weeks and before stopping EBF If still BF at 9, 12 and 18 months antibody test if HIV positive DNA-PCR to confirm (national protocol). CD4 count every 6 months and WHO staging for mother and HAART as per national guidelines Treatment and prophylaxis of OI for mothers Cotrimoxazole prophylaxis for infants up to confirmed HIV negative result Family planning Counselling on: disclosure, partner involvement, safe infant feeding, on-going counselling Support groups (for every 20 mothers as per Karatina model) Nutritional support Infants with HIV positive results assessed for OI and HAART Immunizations and follow up in the MCH clinic (under 5) as per national guidelines (including vit A and multivit). Mothers who opt NOT to breastfeed: Mothers provided with safe water kit and infant formula during last trimester of pregnancy and up to 1 year of age then discharged Computerized file opened with multiple variables DNA-PCR at 6 weeks, if HIV negative confirmatory test at 9 m (according to national protocol). CD4 count every 6 months and WHO staging for mother and HAART as per national guidelines Treatment and prophylaxis of OI for mothers Cotrimoxazole prophylaxis for infants up to confirmed HIV negative result Family planning Counselling on: disclosure, partner involvement, safe infant feeding, on-going counselling Support groups (for every 20 mothers as per Karatina model) Nutritional support Infants with HIV positive results assessed for OI and HAART Immunizations and follow up in the MCH clinic (under 5) as per national guidelines (including vit A and multivit) P R E G N A NC Y DELIVERY I N F A N T F E E DI N G Model of care for pregnant women living with HIV and their infants
. CD4 count < 350: HAART, prophylaxis and treatment of OI CD4 count > 350: AZT from 28 weeks, prophylaxis and treatment of OI. SD- NVP adding (AZT+3TC for 3 days) Mothers who opt TO breastfeed Exclusive breastfeeding (EBF) for 6 months or as long as the mothers can manage, then supported weaning with infant formula, counselling and safe water kit. Supply of infant formula up to 1 year of age then discharged Computerized file opened with multiple variables DNA-PCR at 6 weeks and before stopping EBF If still BF at 9, 12 and 18 months antibody test if HIV positive DNA-PCR to confirm (national protocol). CD4 count every 6 months and WHO staging for mother and HAART as per national guidelines Treatment and prophylaxis of OI for mothers Cotrimoxazole prophylaxis for infants up to confirmed HIV negative result Family planning Counselling on: disclosure, partner involvement, safe infant feeding, on-going counselling Support groups (for every 20 mothers as per Karatina model) Nutritional support Infants with HIV positive results assessed for OI and HAART Immunizations and follow up in the MCH clinic (under 5) as per national guidelines (including vit A and multivit). Mothers who opt NOT to breastfeed: Mothers provided with safe water kit and infant formula during last trimester of pregnancy and up to 1 year of age then discharged Computerized file opened with multiple variables DNA-PCR at 6 weeks, if HIV negative confirmatory test at 9 m (according to national protocol). CD4 count every 6 months and WHO staging for mother and HAART as per national guidelines Treatment and prophylaxis of OI for mothers Cotrimoxazole prophylaxis for infants up to confirmed HIV negative result Family planning Counselling on: disclosure, partner involvement, safe infant feeding, on-going counselling Support groups (for every 20 mothers as per Karatina model) Nutritional support Infants with HIV positive results assessed for OI and HAART Immunizations and follow up in the MCH clinic (under 5) as per national guidelines (including vit A and multivit) P R E G N A NC Y DELIVERY I N F A N T F E E DI N G Model of care for pregnant women living with HIV and their infants.")
31
EPI, < 5 yrsGroup counseling and HIV testing ANC, clinical care, individual counselling, IEC, replacement feeding, HAART, blood removal, clinician on call Family planning 4 mtr. Integration of HIV care services in MCH department in the District Hospital “MCH is a department run by nurses, if HIV positive pregnant and postnatal mothers are not to be referred to the HIV clinic, a clinician on permanent basis or on call is required”

32
HIV testing uptake in ANC for first visit pregnant women District Hospital

33
Safe water Kit 85% of mothers opted for using a feeding bottle despite of being counselled on the cup, (n=99) Mugo et al, TUPEB107 Sydney 2007 IAS Conference Methods: What makes replacement feeding safe in areas with limited resources?
 Mugo et al, TUPEB107 Sydney 2007 IAS Conference Methods: What makes replacement feeding safe in areas with limited resources")
34
Results Infants of HIV+ mothers followed in MCH clinic n=217 Infants initiated on RF at birth n=146 Postnatal enrolment: 19 infants from CM to RF 16 infants from BF to RF Mean duration CM: 23 days Mean duration BF: 31 days 48 infants still active at the time of the analysis Mean follow-up: 86 days DNA-PCR results available: 9 No HIV+ results 127 infants discharged Mean duration RF: 143 days DNA-PCR results available: 109 1 HIV+ result (0.9%) Total infants initiated on RF N=181 Total infants receiving RF n=175 3 infants defaulted 3 infants died (2 HIV+) Figure 1. Replacement feeding program cohort profile, Maragua District Hospital CM=cow’s milk, BF=breast fed, RF=replacement feeding

35
Replacement feeding program in Karatina District Distribution according to support groups. Period Sept 06 – May 08 No aditional human resources needed in this program 85% of HIV infected mothers opted not to breastfeed their infants 59% of partners support RF. Since April 2007 no new HIV infections.

36
Results Períod: September 2005 to January 2008 3 Public Hospitals: Maragua (rural), Karatina (semi-urban), Nyeri (urban). 577 infants included in the replacement feeding program (RF) DNA-PCR results available in 402 infants - 214 (53.2%) infants completed 6 months of RF - 163 (40.5%) still active - 10 (2.4%) died - 15 (3.7%) Lost to follow up Received breastmilk before inclusion in RF program: 44 (10.9%) infants, 9 (18%) HIV positive. Never exposed to breastmilk: 358 (89.1%), 11 (3.1%) HIV positive. OR (IC95): 7.88 (2.77-22.29) p<0.001. Mortality rates in the first 6 months of life: 20% for HIV infected infants and 1.6% for HIV negative infants. OR (IC95): 15.67 (3.30-72.1) p<0.001. Morbility: URTI: 76 episodes (13.1%), and diarrhoea in 23 (4 %) episodes.
 DNA-PCR results available in 402 infants (53.2%) infants completed 6 months of RF (40.5%) still active - 10 (2.4%) died - 15 (3.7%) Lost to follow up Received breastmilk before inclusion in RF program: 44 (10.9%) infants, 9 (18%) HIV positive. Never exposed to breastmilk: 358 (89.1%), 11 (3.1%) HIV positive. OR (IC95): 7.88 ( ) p< Mortality rates in the first 6 months of life: 20% for HIV infected infants and 1.6% for HIV negative infants. OR (IC95): ( ) p< Morbility: URTI: 76 episodes (13.1%), and diarrhoea in 23 (4 %) episodes..")
37
Period evaluated January-December 2007 for 344 HIV infected children included in the HAART program and for 142 pairs (mothers and infants) included in the comprehensive PMTCT program. Costs included in the analysis: medications (ARV and opportunistic infections OI), replacement feeding up to 9 months, safe water kit, labour costs, laboratory and transport costs. Costs not included: In patient department admissions, costs related to human resources, trainings and infrastructures such as the construction of a paediatric HIV clinic, psychosocial, home based care and costs related to disabilities. Cost of 1 year treatment (HAART):150,2 USD Cost of PMTCT+ package:576,5 USD Financial costs of treating and preventing pediatric HIV infection during one year. The experience of Maragua, a rural district in Central Kenya
, replacement feeding up to 9 months, safe water kit, labour costs, laboratory and transport costs. Costs not included: In patient department admissions, costs related to human resources, trainings and infrastructures such as the construction of a paediatric HIV clinic, psychosocial, home based care and costs related to disabilities. Cost of 1 year treatment (HAART):150,2 USD Cost of PMTCT+ package:576,5 USD Financial costs of treating and preventing pediatric HIV infection during one year. The experience of Maragua, a rural district in Central Kenya.")
38
Findings from an assesment conducted in 2 District Hospitals with no RF during the scaling up process. M. Manzi, R Zachariah, R Teck et al. High acceptability of voluntary counselling and HIV testing but unacceptable loss to follow up in a PMTCT program in rural Malawi: scaling up requires a different way of acting. Tropical Medicine and International Health. Vol 10, No 12, 1242-1250 Dec 2005. 3 infants were discharged after completing the national HIV testing algorithm (Kiambu).
..")
39
Laboratory CCC-HIV clinic Pharmacy MCH- Antental and postnatal clinics High Risk clinic PMTCT office Registration. ANC card Nutrition Flow of HIV positive pregnant women in the hospital

40
Safety and Efficacy of a Replacement Feeding Program for Prevention of Mother to Child Transmission (PMTCT) of HIV in a Resource Limited Rural Setting: The Experience of Maragua District, Central Province, Kenya 4 th IAS Conference. Sydney 2007. Abstract TUPEB107

41
Capsule Summary CCO Official Conference Coverage of the 4th International AIDS Society Conference on HIV Pathogenesis, Treatment, and Prevention Formula Feeding Helps Prevent MTCT and Considered Safe in Resource-Limited Settings Posting Date: August 21, 2007 Summary of Key Conclusions Low morbidity and mortality with replacement (formula) feeding Low rate of mother-to-child transmission (MTCT) of HIV with combination of replacement feeding for infants and antiretroviral drugs May provide a safe alternative to breastfeeding in preventing vertical transmission of HIV-1 infection Hoosen Coovadia, MBBS, MD Mauro Schechter, MD, PhD Richard E. Chaisson, MD

42
Lessons learned It is possible to effectively implement WHO recommendations and achieve good HIV free survival in the public sector. MoH overall coordinator and partners supporting MoH program. HIV infected mothers should be supported in their choice: Ungent need to remove the Affordability of the AFASS criteria. Integration of HIV care in MCH services reduces referrals of HIV infected pregnant women to other departments and improves quality of care Postnatal care in 4 programs recommending breastfeeding with no support for HIV+ mothers opting not to breastfeed is almost non existant. Urgent need for MoH and partners to sit and understand why. Exposure to breast milk is associated with high rates of HIV transmission and HIV infection is associated with high risk of mortality. Weaning from RF is easier than from EBF. The risk of mixing RF with other feeds, (no BF) does not increase HIV infection (ERF is not an absolute must).
 does not increase HIV infection (ERF is not an absolute must)..")
43
Lessons learned (ii) Small support groups (up to 20 mothers), M2M and distribution of milk in a community set up increases partner involvement. PMTCT and PMTFT when discordant couples are found (positive prevention). Infant formula will always have to be there. 7-10% of infants could not breastfeed due to multiple pregancies, not enough milk (low CD4 and advanced infection) and mother´s death or abandonment. Programs already providing pediatric HAART should also have replacement feeding as an option for mothers opting not to breastfeed Availability of RF accelerates acceptance and disclosure of HIV infection. Case holding is very high in postnatal clinics compared to mothers breastfeeding because no support is given to them. Supporting HIV infected mothers who choose not to breastfeed their infants is safe and highly effective in preventing pediatric infections in areas with limited resources. Many of them are already giving animal milk due to lack of support. The potential role of the HIV infected mothers remain understimated as access to RF is less than 1% in SSA today (excluding South Africa and Botswana).
. Infant formula will always have to be there. 7-10% of infants could not breastfeed due to multiple pregancies, not enough milk (low CD4 and advanced infection) and mother´s death or abandonment. Programs already providing pediatric HAART should also have replacement feeding as an option for mothers opting not to breastfeed Availability of RF accelerates acceptance and disclosure of HIV infection. Case holding is very high in postnatal clinics compared to mothers breastfeeding because no support is given to them. Supporting HIV infected mothers who choose not to breastfeed their infants is safe and highly effective in preventing pediatric infections in areas with limited resources. Many of them are already giving animal milk due to lack of support. The potential role of the HIV infected mothers remain understimated as access to RF is less than 1% in SSA today (excluding South Africa and Botswana)..")
44
Challenges Feeding bottle versus cup. Majority of mothers prefer the bottle despite being counselled on the cup. Is it possible to implement such a policy?* RF programs have been threatened because of fear of spill over to HIV negative mothers. Exclusive breastfeeding campaign needs a different approach with more political commitment (e.g. realistic maternity leave). *Cup-Feeding Not Recommended Over Bottle-Feeding as a Supplement to Breast-Feeding Cochrane Database Syst Rev. Published online April 18, 2007.
. *Cup-Feeding Not Recommended Over Bottle-Feeding as a Supplement to Breast-Feeding Cochrane Database Syst Rev. Published online April 18,")
45
Challenges (ii) We found no studies taken to improve safety in RF in areas with limited resources although it is the common practise in developed world. Are we still in the aftermath of the 70’s when infant formula was irresponsibly marketed (era pre HIV epidemic)? International code of marketing breast-milk substitutes (1981). No infant formula in MCH clinics (negative impact: e.g.Maragua experience with IF distributed in CCC). 1977 1974
. International code of marketing breast-milk substitutes (1981). No infant formula in MCH clinics (negative impact: e.g.Maragua experience with IF distributed in CCC)")
46
Challenges (iii) Urgent need of a low cost, high quality, generic infant formula with local production and duty free. General fear to take a risk and try to do in Africa what has proved effective in the developed world rather than suboptimal recommendations than keep us discussing for long and not solving the problem. MSF-CAME big role to play...

47
Infant feeding and MSF Major challenges/obstacles in having safe replacement feeding available: 1The quality of water. MSF has a Wat/San unit. 2Advocacy for best practises also in SSA. Generic infant formula. CAME?

48
Thank you for your attention

Similar presentations

















: What Will it Take to Eliminate MTCT? Jessica Rodrigues Presentation for UNICEF Written.>")


 Programs in 7 countries: Rosalind Carter, PhD Epidemiologist, PMTCT, Pediatrics.>")



