Download presentation
Presentation is loading. Please wait.

1
The effect of maternal drug use on the neonate N. Ambalavanan MD, FAAP Neonatologist

2
Purpose of this presentation u To help you understand the prevalence and risks of drug use in pregnancy u To help you identify the infants at higher risk of drug exposure in fetal and neonatal life u To understand the basis of management of drug exposed infants

3
Exposure of the fetus to drugs u Concepts: l The uterus is NOT a fully protected environment for the fetus, either physically or chemically. Almost every substance used by the mother passes to the fetus. l The fetus is the highest animal in the food chain. l Disorder of organ or structure formation can occur only in the first few weeks of pregnancy (<12 weeks) when organs are forming, while changes in size or destruction of structures are possible in the subsequent months. l Drugs can also cause intellectual or functional disorders.
 when organs are forming, while changes in size or destruction of structures are possible in the subsequent months. l Drugs can also cause intellectual or functional disorders..")
4
Drugs in pregnancy u Classification: l Substances not generally considered drugs: alcohol, cigarettes, coffee, solvents, various chemicals etc. l Non-prescription drugs: E.g. aspirin, ibuprofen (Advil/Motrin), vitamins, products from health food stores etc. l Prescription drugs: E.g. antibiotics, anti-epileptic drugs etc. l Drugs of abuse / Illegal drugs: E.g. cocaine, heroin, amphetamines, marihuana etc.
, vitamins, products from health food stores etc. l Prescription drugs: E.g. antibiotics, anti-epileptic drugs etc. l Drugs of abuse / Illegal drugs: E.g. cocaine, heroin, amphetamines, marihuana etc..")
5
The use of drugs in pregnancy u Although the use of illegal drugs attracts considerable attention, the use of legal drugs and of alcohol or cigarettes is far more widespread. u Pregnancy is a symptom-producing event, and pregnant women usually consume more drugs (and food). u A World Health Organization Survey (1991) of 14,778 women from 22 countries showed that 79% received an average of 3.3 drugs (not including OTC drugs or alcohol/tobacco).
. u A World Health Organization Survey (1991) of 14,778 women from 22 countries showed that 79% received an average of 3.3 drugs (not including OTC drugs or alcohol/tobacco)..")
6
The use of drugs in breast-feeding mothers u Breast feeding is resurgent: l 1930’s :80% breast-fed --> 1950’s: 50% --> 1970’s: 20% -->1990’s: 50% u Breast feeding superior to formula feeds (nutritional, immunologic, and psychological properties), but also carries maternal drugs to baby.
, but also carries maternal drugs to baby.")
7
Substances not generally considered drugs: Alcohol u Alcohol is teratogenic --> Fetal Alcohol Syndrome (FAS) u Incidence: l 1/300-1/2000 (depending on population): Avg. 1/500 l 30-40% of neonates of alcoholic mothers affected. l Most common recognizable cause of mental retardation u Incidence of alcohol abuse in pregnancy may be increasing in recent years (0.7-->1.4%). 20% of alcoholics are women. u Even 1-2 drinks daily (30 cc of absolute alcohol) in early pregnancy may lead to FAS, but 4-5 drinks (60-75 cc) are usually required to cause FAS. No safe limit established.
. 20% of alcoholics are women. u Even 1-2 drinks daily (30 cc of absolute alcohol) in early pregnancy may lead to FAS, but 4-5 drinks (60-75 cc) are usually required to cause FAS. No safe limit established..")
8
Fetal Alcohol Syndrome At least one feature from each of three categories: 1. Prenatal and postnatal retardation - with small-for-age weight, length, and/or head circumference. 2. CNS disorders with signs of abnormal brain functioning, delays in behavioral development, and/or intellectual impairment. 3. At least two of the following: abnormal craniofacial features - small head, small eyes or short eye openings, or a poorly developed philtrum (the grove above the upper lip), thin upper lip, short nose, or flattened mid facial area. Fetal Alcohol Effects Alcohol exposed babies that do not meet all these criteria for FAS.
, thin upper lip, short nose, or flattened mid facial area. Fetal Alcohol Effects Alcohol exposed babies that do not meet all these criteria for FAS..")
9
Alabama: General population

10
Alcohol and Alabama (1997) u % of mothers who drank before pregnancy: 39% (42% white, 33% black) u % of mothers who drank during pregnancy: 3.6% (4% white, 2.7% black) This 90% reduction suggestive of awareness of danger u % low birth weight: 7.4% if drinking before pregnancy, 9.6% (30% increase) if drinking during pregnancy
 u % of mothers who drank before pregnancy: 39% (42% white, 33% black) u % of mothers who drank during pregnancy: 3.6% (4% white, 2.7% black) This 90% reduction suggestive of awareness of danger u % low birth weight: 7.4% if drinking before pregnancy, 9.6% (30% increase) if drinking during pregnancy")
11
Alcohol and breast feeding u Alcohol passes freely into breast milk, but acute effects on infant are rare. Chronic effects are uncertain. u American Academy of Pediatrics : Alcohol is usually compatible with breastfeeding. Breastfeeding infants of mothers who regularly use alcohol should be closely monitored. u Infants prenatally exposed to alcohol may have weaker sucking responses u Heavy drinking by the mother can decrease her milk supply, as well as inhibit the milk-ejection reflex.

12
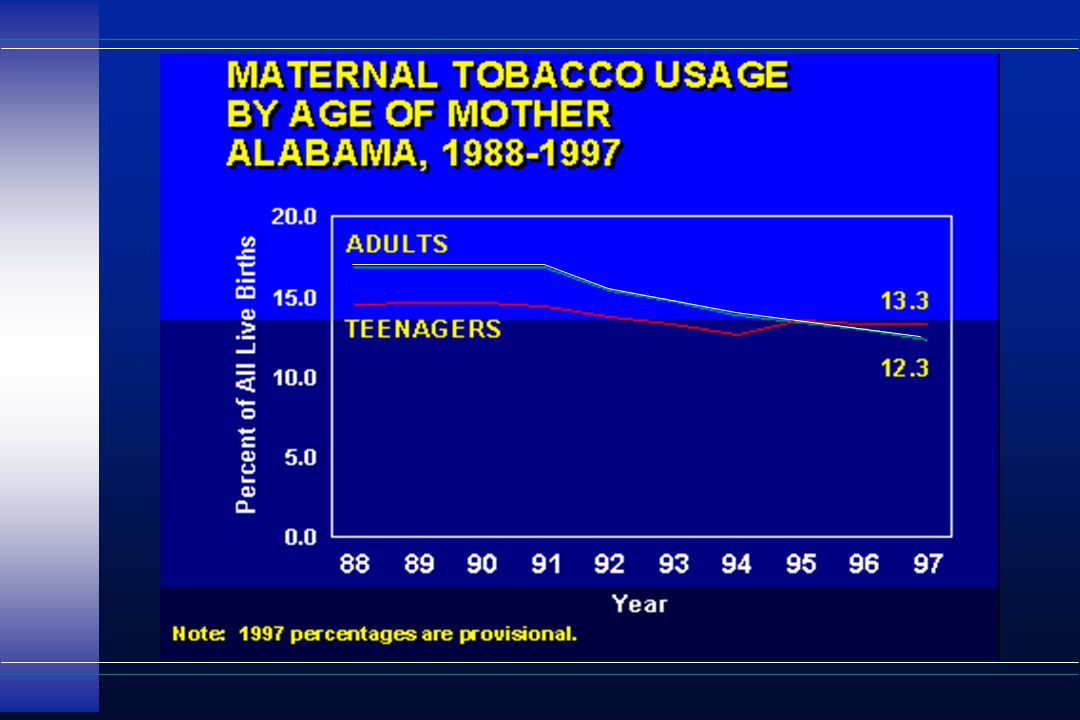
Tobacco u More than 1 in 8 women (13.6%) smoke during pregnancy. 1 in 6 (17.2%) pregnant teens smoke. u Heavy smokers are unlikely to stop during pregnancy u Nicotine (decreases blood flow to placenta and causes fetal hypoxia), carbon monoxide, cyanide etc are among the 4000+ constituents of cigarette smoke that may be hazardous.
 pregnant teens smoke. u Heavy smokers are unlikely to stop during pregnancy u Nicotine (decreases blood flow to placenta and causes fetal hypoxia), carbon monoxide, cyanide etc are among the constituents of cigarette smoke that may be hazardous..")
13
Effects of smoking in pregnancy u Increase in low birth weight (proportional to number of cigarettes) (LBW in Alabama FY 1997: 10.7% in smokers vs. 5.3% in non-smokers (White), and 15.3% vs. 12.8% (Black).) u 40% higher perinatal death (4800 deaths/yr in the US) u Spontaneous abortion: 1.2x /10 cigarettes (141,000/yr) u Active and passive smoking is a risk factor for PPHN. u Significant decrease in IQ (even at 6 yrs age) in multiple studies. u Smoking linked to 2700 SIDS deaths/yr in the US alone.
, and 15.3% vs. 12.8% (Black).) u 40% higher perinatal death (4800 deaths/yr in the US) u Spontaneous abortion: 1.2x /10 cigarettes (141,000/yr) u Active and passive smoking is a risk factor for PPHN. u Significant decrease in IQ (even at 6 yrs age) in multiple studies. u Smoking linked to 2700 SIDS deaths/yr in the US alone..")
21
Caffeine: Coffee, Tea, Cola u One of the most popular “drugs” in the world. u One cup coffee =70-100 mg, tea 40-50 mg, cola 30- 40 mg caffeine u Fetal levels are similar to maternal levels, and may alter fetal sleep patterns u Moderate consumption (1-2 cups coffee/day) are probably safe. High doses (>5-6 cups/day) may cause spontaneous abortion, difficulty in becoming pregnant, and possibly lower birth weight.
 are probably safe. High doses (>5-6 cups/day) may cause spontaneous abortion, difficulty in becoming pregnant, and possibly lower birth weight..")
22
Non-prescription drugs u Aspirin: l The most commonly ingested drug in pregnancy. In 8 surveys of >50,000 patients, aspirin was consumed in >30,000 (61%). l Can cause bleeding, prolonged labor, prolonged gestation in mom. Low dose maternal aspirin (<150 mg/day) may be safe to baby. Higher doses may cause PPHN and bleeding in neonates and should be avoided in pregnancy. l To be used with caution during lactation (small amount in breast milk)
. l Can cause bleeding, prolonged labor, prolonged gestation in mom. Low dose maternal aspirin (<150 mg/day) may be safe to baby. Higher doses may cause PPHN and bleeding in neonates and should be avoided in pregnancy. l To be used with caution during lactation (small amount in breast milk).")
23
Non-prescription drugs (contd.) u Ibuprofen (Advil/Motrin): May lead to PPHN, prolongation of pregnancy. To be avoided in pregnancy, esp 3rd trimester. Safe during breast feeding. u Acetaminophen (Tylenol): Safe for short-term use in regular doses. Toxic at high doses to mom and baby. Compatible with breast feeding. u Anti-histamines e.g. Diphenhydramine (Benadryl): Possibly safe (some reports of malformations). C/I during lactation (babies are sensitive to antihistamines)
: Safe for short-term use in regular doses. Toxic at high doses to mom and baby. Compatible with breast feeding. u Anti-histamines e.g. Diphenhydramine (Benadryl): Possibly safe (some reports of malformations). C/I during lactation (babies are sensitive to antihistamines).")
24
Non-prescription drugs u Avoid anti-diarrheal agents, laxatives. Anti-acid agents e.g Ranitidine (Zantac), Famotidine (Pepcid) are generally safe. u Diabetics and asthmatics need special attention. Some drugs cause more problems. u Avoid vaccines unless they are essential. u Avoid cough medicines, diuretics. u Avoid hormones esp. steroids and their derivatives (health food stuff like DHEA), radiation
, Famotidine (Pepcid) are generally safe. u Diabetics and asthmatics need special attention. Some drugs cause more problems. u Avoid vaccines unless they are essential. u Avoid cough medicines, diuretics. u Avoid hormones esp. steroids and their derivatives (health food stuff like DHEA), radiation.")
25
Non-prescription drugs (contd.) u Vitamins: l Folic Acid: Essential vitamin - prevents NTDs. Necessary to take if considering pregnancy! l Vitamin A: High doses cause malformations. Acne medications (isotretinoin) are very dangerous. Vitamin A is essential, but not more than 8,000 IU/day. l Vitamin D: High intakes may be associated with supravalvular aortic stenosis. Use of multivitamins up to RDA is recommended. Mega- doses may cause problems and should be avoided.
 are very dangerous. Vitamin A is essential, but not more than 8,000 IU/day. l Vitamin D: High intakes may be associated with supravalvular aortic stenosis. Use of multivitamins up to RDA is recommended. Mega- doses may cause problems and should be avoided..")
26
Prescription drugs u Risk varies with drug ingested, dose, stage of pregnancy, interactions with other drugs, individual variation etc. u Risk of not taking the drug versus risk of taking the drug needs to be considered. u Many drugs have not been studied in adequate detail in pregnant humans (extrapolation from animal studies useful only to a point), so current knowledge is unreliable. (Catch-22 situation)
, so current knowledge is unreliable. (Catch-22 situation).")
27
Prescription drugs u Antibiotics: Most penicillins/cephalosporins are usually safe. Quinolones (e.g. Ciproflox), aminoglycosides (e.g. Streptomycin, Gentamycin) are to be avoided. u Anti-hypertensives: ACE inhibitors (Captopril, Enalapril) are usually avoided. u Anticonvulsants: Valproate, Phenytoin etc can cause malformations.
, aminoglycosides (e.g. Streptomycin, Gentamycin) are to be avoided. u Anti-hypertensives: ACE inhibitors (Captopril, Enalapril) are usually avoided. u Anticonvulsants: Valproate, Phenytoin etc can cause malformations..")
28
Illegal drugs (drug abuse): National u More than 5 million American women of childbearing age use illicit drugs (1 million use cocaine, 3.8 million marijuana) u 7.5% of women in labor (+) for at least one drug (Rhode Island Dept of Public Health) u 15% of pregnant women in Florida (+) for alcohol or drug use u Prevalence of drug use similar in different areas of the country, regardless of hospital or size of population
: National u More than 5 million American women of childbearing age use illicit drugs (1 million use cocaine, 3.8 million marijuana) u 7.5% of women in labor (+) for at least one drug (Rhode Island Dept of Public Health) u 15% of pregnant women in Florida (+) for alcohol or drug use u Prevalence of drug use similar in different areas of the country, regardless of hospital or size of population")
29
Illegal drugs (drug abuse) in Alabama l Positive screen in 12.9% of women (11% in pregnant, 15.6% in those not pregnant) l No difference urban (12.8%) vs. rural (13.1%) l No difference “high-risk” vs. “low-risk” obstetric groups l + marijuana > in whites (16%) and non-pregnant (14%) vs. black (7.1%) and pregnant (9.3%) women l + cocaine screen > in non-white (1.9%) and single (1.8%) vs. white (0.9%) women l No difference in + cocaine screen between trimesters (Am J Obstet Gynecol 1991; 165:924-7. n=5010, of which 2970 pregnant)
 l No difference high-risk vs. low-risk obstetric groups l + marijuana > in whites (16%) and non-pregnant (14%) vs. black (7.1%) and pregnant (9.3%) women l + cocaine screen > in non-white (1.9%) and single (1.8%) vs. white (0.9%) women l No difference in + cocaine screen between trimesters (Am J Obstet Gynecol 1991; 165: n=5010, of which 2970 pregnant).")
30
Identification of substance abuse u It is a misconception that substance abuse occurs only in lower socio-economic groups u Many pregnant women are unaware of adverse effects that may occur, and may not volunteer a history of illicit drug use if they fear that their baby and other children may be taken away from them u It is the responsibility of the health care team to identify, educate, counsel, and manage pregnant women and their neonates with substance abuse problems

31
Identification of illicit drug use u Patient-reported history not adequate: sensitivity 6.3%, specificity 98% u Tobacco and alcohol use pattern: sensitivity better (16.4%) but still not adequate u Suspected preterm labor: 17% (+) UDS (cocaine 10% ) u Benefit vs. cost and pitfalls of universal screening?

32
Suggested guidelines for drug screening of the neonate u Urine, meconium, or hair analysis should be performed if: A) Mothers have a history of any one of: 1) H/o of drug abuse in present or past pregnancy 2) Limited prenatal care ( 18 wks GA in preterm infants) 3) H/o of Hepatitis B, HIV, Syphilis, Gonorrhea 4) H/o prostitution 5) Unexplained placental abruption / premature labor
 Mothers have a history of any one of: 1) H/o of drug abuse in present or past pregnancy 2) Limited prenatal care ( 18 wks GA in preterm infants) 3) H/o of Hepatitis B, HIV, Syphilis, Gonorrhea 4) H/o prostitution 5) Unexplained placental abruption / premature labor")
33
Suggested guidelines for drug screening of the neonate B) Infants who exhibit any one of the following: 1) Unexplained neurological complications (e.g. intracranial hemorrhage/infarction, seizures) 2) Evidence of possible drug withdrawal ( e.g. hypertonia, irritability, trembling, muscle rigidity, constipation or diarrhea) 3) Unexplained IUGR ( modified from Wagner et al: The impact of prenatal drug exposure on the neonate: Obstet & Gynecol Clin North Am 25 (1):169-194, 1998)
 2) Evidence of possible drug withdrawal ( e.g. hypertonia, irritability, trembling, muscle rigidity, constipation or diarrhea) 3) Unexplained IUGR ( modified from Wagner et al: The impact of prenatal drug exposure on the neonate: Obstet & Gynecol Clin North Am 25 (1): , 1998).")
34
How effective is screening? u Urine Drug Screening (UDS) most often used: l Can detect cocaine (up to 8 hrs in mom, 72 hrs in baby), opiates (morphine and heroin up to 48 hrs), amphetamines (48 hrs), barbiturates (short acting 48 hrs, long acting 7 days), and benzodiazepines (variable). (Can also be used to detect marijuana and alcohol but not usually done) u Meconium analysis: meconium is a reservoir for drugs from 18 wks GA to delivery. However, more expensive ($90 vs. $20 for UDS) and technically difficult. u Hair analysis: Useful till 3 months age. Timing possible.
 most often used: l Can detect cocaine (up to 8 hrs in mom, 72 hrs in baby), opiates (morphine and heroin up to 48 hrs), amphetamines (48 hrs), barbiturates (short acting 48 hrs, long acting 7 days), and benzodiazepines (variable). (Can also be used to detect marijuana and alcohol but not usually done) u Meconium analysis: meconium is a reservoir for drugs from 18 wks GA to delivery. However, more expensive ($90 vs. $20 for UDS) and technically difficult. u Hair analysis: Useful till 3 months age. Timing possible..")
35
Marihuana (pot/joint/reefer) Cannabis sativa. 400 chemicals. 61 cannabinoids. - 9-tetrahydrocannabinol (THC) main agent. u Second commonest substance abused (after tobacco). u Seriousness underestimated since it is not usually considered a “hard” drug u Difficult to estimate effect of Marihuana alone (polydrug use, variation in amount smoked, differences in strength of cigarettes, social factors)
 main agent. u Second commonest substance abused (after tobacco). u Seriousness underestimated since it is not usually considered a hard drug u Difficult to estimate effect of Marihuana alone (polydrug use, variation in amount smoked, differences in strength of cigarettes, social factors).")
36
Marihuana : effects on the baby u No definite proof of malformations u May be associated with growth retardation u May be associated with abnormal neurological development (inconsistent finding) u May be associated with prematurity (very doubtful) u Effects more likely to occur with heavier use
 u May be associated with prematurity (very doubtful) u Effects more likely to occur with heavier use")
37
Cocaine (crack/coke) u Alkaloid derivative of Erythroxylon coca u Inhibits re-uptake of sympathomimetics (Epinephrine, NE, DA), causing rapid heart rate, hypertension, vasoconstriction u Cocaine easily passes into fetus through placenta u Decreases blood flow to uterus, decreases fetal oxygenation and intestinal blood flow.
 u Alkaloid derivative of Erythroxylon coca u Inhibits re-uptake of sympathomimetics (Epinephrine, NE, DA), causing rapid heart rate, hypertension, vasoconstriction u Cocaine easily passes into fetus through placenta u Decreases blood flow to uterus, decreases fetal oxygenation and intestinal blood flow.")
38
Cocaine: effects on the baby u Lower birth weight, smaller head size (smaller brain), shorter length, greater risk of IUGR, and genito-urinary and cardiac defects u Lower scores on neonatal and childhood developmental exams u Increased risk for necrotizing enterocolitis, even in term babies u Increased risk for SIDS u Increased risk for cerebral stroke/hemorrhage
, shorter length, greater risk of IUGR, and genito-urinary and cardiac defects u Lower scores on neonatal and childhood developmental exams u Increased risk for necrotizing enterocolitis, even in term babies u Increased risk for SIDS u Increased risk for cerebral stroke/hemorrhage")
39
Amphetamines (Meth/crystal/rock) u Stimulant drugs which work in a manner similar to cocaine u Problems similar to cocaine/polydrug use: LBW, prematurity, abruption, neonatal withdrawal. Case series of congenital brain hemorrhage/infarction. u Lower scores in neurodevelopment (infancy) and aggressive behavior (at 8 yrs of age) noted. u LSD often diluted with amphetamines. Direct effect of LSD alone difficult to determine.
 and aggressive behavior (at 8 yrs of age) noted. u LSD often diluted with amphetamines. Direct effect of LSD alone difficult to determine..")
40
Morphine/Heroin/Methadone/Demerol u 9000 babies are born to narcotic addicts each year in the US. In 1992, 88,000 women were using heroin regularly. u Withdrawal symptoms are the main risk (40-80%). Symptoms: Abnormal sleep pattern, irritability, seizures, fever, sweating, tachypnea, sneezing, excessive sucking, poor feeding, loose stools, vomiting. Symptoms may occur much later and last longer (2-30 days) with methadone
. Symptoms: Abnormal sleep pattern, irritability, seizures, fever, sweating, tachypnea, sneezing, excessive sucking, poor feeding, loose stools, vomiting. Symptoms may occur much later and last longer (2-30 days) with methadone.")
41
Narcotics: effects on the baby u Increased incidence of low birth weight, IUGR, prematurity. u 2-4 fold higher risk for SIDS u Long-term developmental abnormalities (lower scores on IQ & language tests even when placed in foster homes) u Associations include an increased risk for sexually transmitted diseases, hyperbilirubinemia, and poor social situation (true for all drugs of abuse)
 u Associations include an increased risk for sexually transmitted diseases, hyperbilirubinemia, and poor social situation (true for all drugs of abuse).")
42
Management of the drug-exposed neonate u More general than specific: l Decreased environmental stimulation l Swaddling l Darkened environment l Small frequent feeds u Withdrawal symptoms: Phenobarbital often used. If exposed to only opiates, tincture of opium/paregoric can be used u Social evaluation a MUST! Improvement of future social environment the best long-term treatment.

Similar presentations






>")

>")
















