Download presentation
Presentation is loading. Please wait.

1
1 Open Classroom Series Fall 2013: Policy for a Healthy America Every Wednesday, 6pm – 8pm September 4 through December 4 West Village F, Room 20 Northeastern University School of Public Policy and Urban Affairs

2
This Week (October 2, 2013) School of Public Policy & Urban Affairs | Northeastern University Dr. Adam Powell Healthcare Economist & President, The Payer + Provider Syndicate “The Doctor is in (your pocket): When your smart phone takes care of you” Dr. John Halamka Professor of Medicine, Harvard Medical School; Chief Information Officer, BIDMC
: When your smart phone takes care of you Dr. John Halamka Professor of Medicine, Harvard Medical School; Chief Information Officer, BIDMC.")
4
Challenges in Consumer-Oriented mHealth Adam C. Powell, Ph.D. President, Payer+Provider Syndicate Adjunct of Health Informatics, Northeastern

5
Who here owns one of these devices?

6
Who here is wearing one of these devices?

7
Who here has ever used a fitness app?

8
Who here has used a fitness app this week?

9
Technology is not the challenge For the first time in American history, it is common for people to run around carrying: Wireless radios capable of transmitting data across personal networks, local networks, and global networks An accelerometer, compass, GPS, gyroscope, and camera A networked computer capable of interacting with both other computers and electronic devices

10
Learning goals for today’s lecture Answer three questions: 1.What is mHealth? 2.What are the social challenges in the consumer adoption of mHealth products and services 3.What are the legal challenges in the consumer adoption of mHealth products and services

11
“mHealth is the use of mobile and wireless devices to improve health outcomes healthcare services and health research.” -Official definition used by the NIH Consensus Group

12
Consumer mHealth devices help people… Improve Health and Wellness Track Sleep Track Diet Track Weight Measure Adherence Improve Posture Track Activity

13
What are the barriers to adoption? Homer Simpson is: Obese Physically inactive Likely diabetic Why isn’t he wearing a pedometer?

14
What are the barriers to adoption? Mr. Monk is: Compulsive In his mid-fifties In need of tools for maintaining and improving his fitness Why isn’t he wearing a pedometer?

15
These consumer products often don’t work. Require behavioral changeHave no immediate benefit Require long-term adherence

16
Problem: Requiring behavioral change Getting people in the habit of recording something, with the hope they’ll develop another habit as a result Glucose logging Diet logging Water logging Logging anything…

17
Solution: Integrating with existing behaviors Using technology to enhance existing behaviors, rather than creating new ones Putting a cellular antenna in a glucometer, so that data is automatically shared with providers and apps Putting a WiFi chip in a scale, so that weight is automatically recorded

18
Problem: Having no immediate benefit Suggesting people perform some sort of activity that has no immediate benefit, although it may have long-term benefits Tracking long-term impact wellness activities Prompting people to take preventive medications

19
Solution: Focusing on the short and long term Provide people with both immediate and long-term rewards for their activities, so that they remain engaged Provide social encouragement Provide financial incentives for good behavior in real-time

20
Problem: Requiring adherence Requiring people to continue to do something in order to deliver a benefit Wearing something Logging something Taking something

21
Solution: Anticipating poor adherence People often are non- adherent because they either do not feel they benefit from adhering, or feel they are harmed from adhering Build systems that anticipate low adherence, rather than ones that require good adherence Send reminders if adherence is poor

22
We can’t change human nature, but we can change products. The biggest challenge we now face is in building human- centered designs.

23
There are legal challenges too… RegulationSafety Privacy & security Slow innovation Laissez-faire Easy entry Connectivity Fast innovation

24
When do apps become dangerous? Cardio Buddy claims to be able to tell me my heart rate by looking at my face What if it says I’m not normal, but I am? What if it says I’m normal, but I’m not? What if I make medical decisions based upon my findings?

25
Wearables can provide different readings Lauren Goode of AllThingsD wore five devices at once to measure the distance she walked Each reported something different Pedometer: 2,382 steps Jawbone Up: 2,339 steps Fitbit Flex: 2,290 steps Nike+ FuelBand: 2,103 steps Basis Band: 1,614 steps In some applications, inaccuracy can be fatal.

26
mHealth solutions have varying levels of risk MinimalHigh weight measurement glucose measurement logging heart rate measurement sleep tracking activity tracking diagnostic interpretation treatment recommendations

27
The regulation of mHealth apps has been a work in progress Q1 ‘11 Q2 ‘11 Q3 ‘11 Q4 ‘11 Q1 ‘12 Q2 ‘12 Q3 ‘12 Q4 ‘12 Q1 ‘13 Q2 ‘13 Q3 ‘13 Q4 ‘13 FDA approves its first medical app FDA issues Draft Guidance about medical app regulation FDA announces that it has approved over 100 apps FDA launches an inquiry into an unapproved urinalysis app FDA issues Final Guidance about medical app regulation

28
The FDA is taking a risk- based approach to regulation Regulated apps either: -Are intended to be used as an accessory to a regulated medical device -Transform a mobile platform into a regulated medical device Based on the Mobile Medical Applications Guidance for Industry and Food and Drug Administration Staff document, released by the FDA on September 25, 2013

29
The FDA will exercise discretion in regulating apps that pose minimal risk Help patients/users self-manage their disease or condition without providing specific treatment suggestions Provide patients with simple tools to organize and track their health information Provide easy access to information related to health conditions or treatments Help patients document, show or communicate potential medical conditions to health care providers Automate simple tasks for health care providers Enable patients or providers to interact with Personal Health Records (PHR) or Electronic Health Record (EHR) systems. Based on the Mobile Medical Applications Guidance for Industry and Food and Drug Administration Staff document, released by the FDA on September 25, 2013

30
Tons of mHealth apps pose more than a minimal risk

31
However, many apps are benign

32
There are both pros and cons to FDA involvement Pros: Increases investor and developer confidence and public safety Creates a barrier to entry Makes apps more able to get payer reimbursement Cons: Makes the FDA the regulator, rather than another entity (e.g. the ONC) Blocks entry by small firms Increases payer obligation to pay for apps
 Blocks entry by small firms Increases payer obligation to pay for apps.")
33
Why are these issues popping up now? Underneath the Radar Small number of users Small firms, small investments “Beta” – not fully trusted Mainstream Many users Big firms, big investments High-quality expected You Are Here

34
What challenges lie ahead? Developing human-centered products that account for the realities of behavior Formalizing regulations so products are trusted, and bigger development investments can be made

35
mHealth is finally growing up mHealth is not new Smartphones have enabled mHealth to reach a level of maturity and practicality previously not possible Today’s mHealth applications will soon seem crude as the industry attracts greater investment

36
Do you have any questions?Adam C. Powell, Ph.D. President Payer+Provider Syndicate powell@payerprovider.com (617) 939-9168
")
38
Connecting Patients, Providers, and Payers John D. Halamka MD

39
The US Healthcare IT Program Improving quality, safety, efficiency, and reducing health disparities Engaging patients and families in their health care Improving care coordination Improving population and public health Ensuring adequate privacy and security protections for personal health information

41
Physician Goals Core ObjectiveMeasure 1. CPOE Use CPOE for more than 60% of medication, 30% of laboratory, and 30% of radiology 2. E-RxE-Rx for more than 50% 3. DemographicsRecord demographics for more than 80% 4. Vital SignsRecord vital signs for more than 80% 5. Smoking StatusRecord smoking status for more than 80% 6. InterventionsImplement 5 clinical decision support interventions + drug/drug and drug/allergy 7. LabsIncorporate lab results for more than 55% 8. Patient ListGenerate patient list by specific condition 9. Preventive Reminders Use EHR to identify and provide reminders for preventive/follow-up care for more than 10% of patients with two or more office visits in the last 2 years

42
Physician Goals Core ObjectiveMeasure 10. Patient Access Provide online access to health information for more than 50% with more than 5% actually accessing 11. Visit SummariesProvide office visit summaries for more than 50% of office visits 12. Education ResourcesUse EHR to identify and provide education resources more than 10% 13. Secure Messages More than 5% of patients send secure messages to their EP 14. Rx Reconciliation Medication reconciliation at more than 50% of transitions of care 15. Summary of Care Provide summary of care document for more than 50% of transitions of care and referrals with 10% sent electronically and at least one sent to a recipient with a different EHR vendor or successfully testing with CMS test EHR 16. Immunizations Successful ongoing transmission of immunization data 17. Security Analysis Conduct or review security analysis and incorporate in risk management process

43
Hospital Goals Core ObjectiveMeasure 1. CPOE Use CPOE for more than 60% of medication, 30% of laboratory, and 30% of radiology 2. DemographicsRecord demographics for more than 80% 3. Vital SignsRecord vital signs for more than 80% 4. Smoking StatusRecord smoking status for more than 80% 5. Interventions Implement 5 clinical decision support interventions + drug/drug and drug/allergy 6. LabsIncorporate lab results for more than 55% 7. Patient ListGenerate patient list by specific condition 8. eMAReMAR is implemented and used for more than 10% of medication orders

44
Hospital Goals Core ObjectiveMeasure 9. Patient Access Provide online access to health information for more than 50% with more than 5% actually accessing 10. Education ResourcesUse EHR to identify and provide education resources more than 10% 11. Rx ReconciliationMedication reconciliation at more than 50% of transitions of care 12. Summary of Care Provide summary of care document for more than 50% of transitions of care and referrals with 10% sent electronically and at least one sent to a recipient with a different EHR vendor or successfully testing with CMS test EHR 13. ImmunizationsSuccessful ongoing transmission of immunization data 14. LabsSuccessful ongoing submission of reportable laboratory results 15. Syndromic Surveillance Successful ongoing submission of electronic syndromic surveillance data 16. Security Analysis Conduct or review security analysis and incorporate in risk management process

45
Patient Profile Screen

46
Patient Profile Screen, cont’d

47
Problems

48
Medications

49
Medication History and Reconciliation

50
Reports

51
External Reports

52
Orders

53
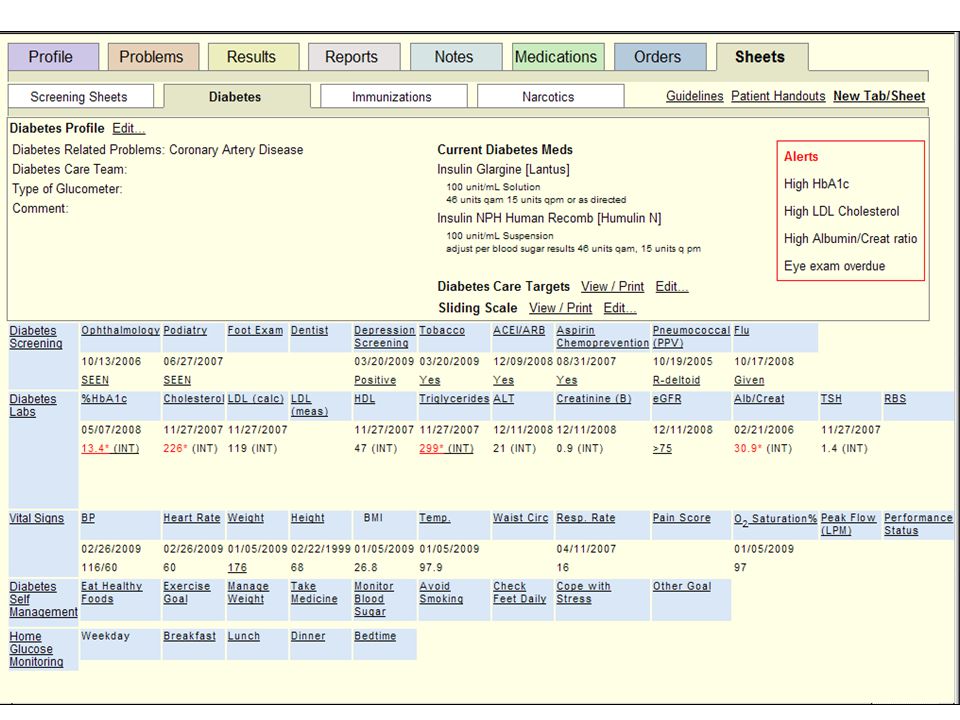
Sheets

55
Care Plans

56
Health Information Exchange eCW EHX NEHEN SafeHealth MD Fallon ClinicUMass Memorial Statewide HISP PKI/certificate mgmt Web portal Provider/entity directory Audit log MD BIDMC Partners Direct gateway services EOHHS NwHIN MassHealth DPH Atrius

57
57 Updated plan Original high-level plan from 12/11/2011 Updated plan as of 10/23/2012

58
Self Service Web Interface

59
- Patient-Level Information Assets BIDPO QDC

60
- Massachusetts eHealth Collaborative Slide title © MAeHC. All rights reserved. Provider Measure Scorecard

61
Decision Support Service Providers

62
School of Public Policy & Urban Affairs | Northeastern University Dr. Adam Powell Healthcare Economist & President, The Payer + Provider Syndicate Any Questions? Dr. John Halamka Professor of Medicine, Harvard Medical School; Chief Information Officer, BIDMC Open Classroom Series Fall 2013: Policy for a Healthy America October 2, 2013 - “The Doctor is in (your pocket): When your smart phone takes care of you.”
: When your smart phone takes care of you. .")
63
Next Week (October 9, 2013) School of Public Policy & Urban Affairs | Northeastern University “Is there a doctor in the house? Maybe not, but will it matter?” Timothy Hoff Associate Professor of Management, Organizational Development, Healthcare Systems, and Healthcare Policy, Northeastern School of Public Policy and Urban Affairs Gregory Sawin Physician (Family Medicine with OB and Primary Care); Assistant Clinical Professor, Tufts University School of Medicine; Clinical Instructor, Harvard Medical School
; Assistant Clinical Professor, Tufts University School of Medicine; Clinical Instructor, Harvard Medical School.")
64
64 Open Classroom Series Fall 2013: Policy for a Healthy America Every Wednesday, 6pm – 8pm September 4 through December 4 West Village F, Room 20 Northeastern University School of Public Policy and Urban Affairs

Similar presentations











>")










