Download presentation
Presentation is loading. Please wait.

1
The Michigan Primary Care Transformation (MiPCT) Project
Overview and Transition of Care Lessons Learned to Date Marie Beisel MSN, RN, CPHQ

2
Disclosure I have no conflict of interest to declare
I do not have any relevant financial relationships with any commercial interests

3
Objectives Describe the Michigan Primary Care Transformation (MiPCT Clinical Model Identify three patient centered medical home care management components associated with positive outcomes Explain the MiPCT transition of care and lessons learned to date

4
CMS Multi-Payer Advanced Primary Care Practice (MAPCP) Demonstration
Centers for Medicare & Medicaid Services is exploring the role of the PCMH in improving US health care Participating in state-based PCMH demonstrations CMS Demo Stipulations Must include Commercial, Medicaid, Medicare patients Must be budget neutral over 3 years of project Must improve cost, quality, and patient experience 8 states selected for participation, including Michigan Michigan start date: January 1, 2012

5
MAPCP Demo: Participating States
Maine practices (year 3) Michigan practices Minnesota 159 practices (year 3) New York practices North Carolina practices Pennsylvania practices Rhode Island practices Vermont practices (year 3) _____________________________________________ TOTAL practices 1,192 (year 3)
 Michigan 410 practices. Minnesota 159 practices 340 (year 3) New York 35 practices. North Carolina 54 practices. Pennsylvania 78 practices. Rhode Island 13 practices. Vermont 110 practices 220 (year 3) _____________________________________________. TOTAL 881 practices 1,192 (year 3)")
6
Michigan: Selected health statistics
45th (of 50 states) in coronary heart disease deaths 41rd in percent of obese adults 34th in infant mortality rate 34th in percent of adults who smoke 34th in overall cancer death rate 20th in percent of adults who exercise regularly 12th in adults receiving colon cancer screening 5th in childhood immunization rate Source: Comparison of Michigan Critical Health Indicators and Healthy People Targets, Michigan Department of Community Health, May 2011
 in coronary heart disease deaths. 41rd in percent of obese adults. 34th in infant mortality rate. 34th in percent of adults who smoke. 34th in overall cancer death rate. 20th in percent of adults who exercise regularly. 12th in adults receiving colon cancer screening. 5th in childhood immunization rate. Source: Comparison of Michigan Critical Health Indicators and Healthy People 2010 Targets, Michigan Department of Community Health, May")
7
The Vision for a Multi-Payer Model
Use the CMS Multi-Payer Advanced Primary Care Practice demo as a catalyst to redesign MI primary care Multiple payers will fund a common clinical model Allows global primary care transformation efforts Support development of evidence-based care models Create a model that can be broadly disseminated Facilitate measurable, significant improvements in population health for our Michigan residents Bend the current (non-sustainable) cost curve Contribute to national models for primary care redesign Form a strong foundation for successful ACO models
 cost curve. Contribute to national models for primary care redesign. Form a strong foundation for successful ACO models.")
8
CMS Multi-Payer Advanced Primary Care Practice (MAPCP) Demonstration
CMS award notification: November 16, 2010 8 states selected for participation, including Michigan Start date: January 1, 2012 Includes Commercial, Medicaid and Medicare patients Financial stipulations Must be budget neutral over 3 years of project Expect improvements in cost, quality, and patient experience

9
MiPCT Practice Participation Criteria
PCMH-designated in 2010, and maintain PGIP or NCQA designation over the 3-year demonstration Part of a participating PO/PHO/IPA Agree to work on the four selected focus initiatives: Care Management Self-Management Support Care Coordination Linkage to Community Services

10
Participating Provider and Payer Partners As of September 2012
# Practices* # POs # Physicians # Payers 387 Practices 36 POs 1650 Physicians 4 (Medicaid*, Medicare, BCBSM**, BCN) *Choice of a 01/01/12 or 04/01/12 start dates; 6 Additional Practices joining in 01/2013. * Medicaid Managed care **BCBSM commercial, BCBSM Medicare Advantage
 *Choice of a 01/01/12 or 04/01/12 start dates; 6 Additional Practices joining in 01/2013. * Medicaid Managed care. **BCBSM commercial, BCBSM Medicare Advantage.")
12
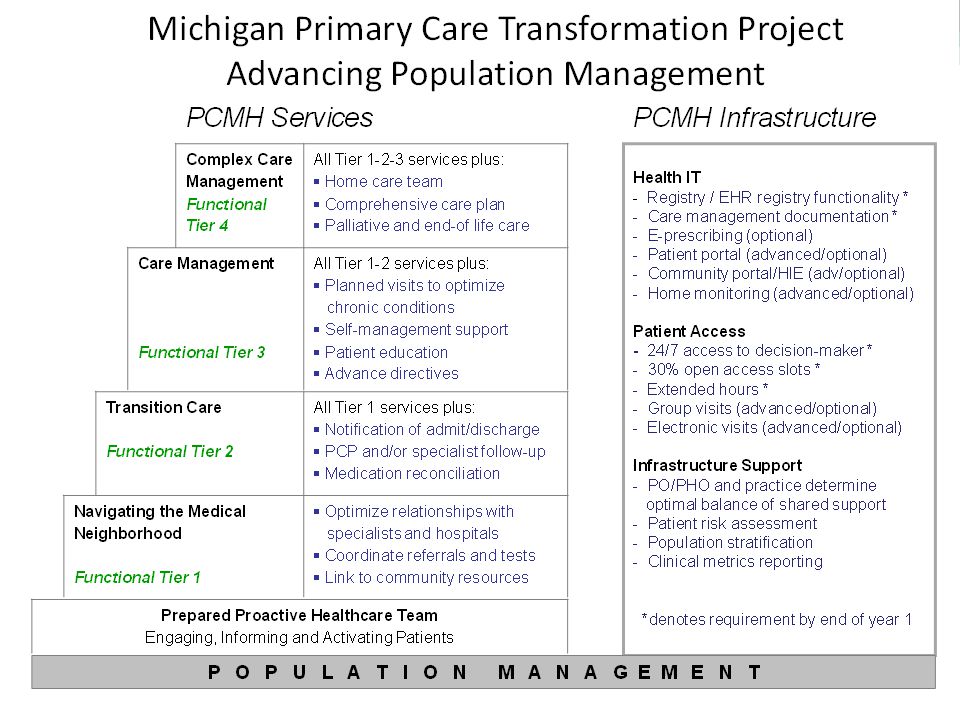
MiPCT Clinical Model: Optimizing Patient Engagement, Improving Population Health

13
Managing Populations: Stratified Approach to Patient Care and
IV. Most complex (e.g., Homeless, Schizophrenia) III. Complex Complex illness Multiple Chronic Disease Other issues (cognitive, frail elderly, social, financial) II. Mild-moderate illness Well-compensated multiple diseases Single disease I. Healthy Population <1% of population Caseload 15-40 3-5% of population Caseload 50% of population Caseload~1000 Managing Populations: Stratified Approach to Patient Care and Care Management
 III. Complex Complex illness Multiple Chronic Disease Other issues (cognitive, frail elderly, social, financial) II. Mild-moderate illness Well-compensated multiple diseases. Single disease. I. Healthy Population. <1% of population Caseload % of population Caseload % of population Caseload~1000. Managing Populations: Stratified Approach to Patient Care and. Care Management.")
15
MiPCT PO/Practice Expectations
Care management Performed for appropriate high and moderate risk individuals Population management Registry functionality by end of year 1 Proactive patient outreach Point of care alerts for services due Access improvement 24/7 access to clinician 30% same-day access Extended hours

16
Success = Improvements in Population Health + Cost + Patient Experience
Statistical analysis of the effect of work completed by the MiPCT practices: care management, care transitions, community linkages, IT, patient access on quantifiable outcomes, using: Claims data Clinical quality indicators Utilization Hospital readmission rate within 30 days Primary Care treatable ED rate Hospitalization rate - ambulatory care sensitive conditions Reference: MiPCT Clinical Metrics updated resource tab

17
Role Comparison: Moderate Risk Care Manager, Complex Care Manager
Moderate Risk Care Manager (MCM) Complex Care Manager (CCM) Patient Population Moderate risk patients identified by registry, PCP referral for proactive and population management. High risk patients identified by PCP referral and input, risk stratification, patient MiPCT list. Patient Caseload Caseload 500 (approx active patients); one MCM per 5,000 patients. Caseload 150 (approx active patients); one CCM per 5,000 patients. Focus of Care Management Proactive, population management. Work with patients to optimize control of chronic conditions and prevent/minimize long term complications. Targeted interventions to avoid hospitalization, ER visits. Ensure standard of care, coordinate care across settings, help patients understand options. Duration of Care Management Typically a series of 1 to 6 visits Frequency of visits high at times, duration of months
 Complex Care Manager. (CCM) Patient Population. Moderate risk patients identified by registry, PCP referral for proactive and population management. High risk patients identified by PCP referral and input, risk stratification, patient MiPCT list. Patient Caseload. Caseload 500 (approx active patients); one MCM per 5,000 patients. Caseload 150 (approx active patients); one CCM per 5,000 patients. Focus of Care Management. Proactive, population management. Work with patients to optimize control of chronic conditions and prevent/minimize long term complications. Targeted interventions to avoid hospitalization, ER visits. Ensure standard of care, coordinate care across settings, help patients understand options. Duration of Care Management. Typically a series of 1 to 6 visits. Frequency of visits high at times, duration of months.")
18
Evidence-Based Review: PCMH Care Management Components Associated With Positive Outcomes
Care delivery by multidisciplinary teams Care delivery in collaboration with physician’s office Attention to care transitions Medication reconciliation In-person visits along with telephonic encounters Patient selection important - risk stratification plus physician input important to successful interventions

19
MiPCT Care Management Priorities
Care managers work in close proximity to PCP team In PCP office as much as possible Work with PCP team to meet their needs Evidence supports this model as superior to vendor-based Ensure Care Management coverage 2 Care Manager per 5000 MiPCT patients Focus on evidence-based interventions Medication reconciliation Care transitions In-person contact with patients whenever possible Comprehensive care plan for complex patients

20
MiPCT Clinical Resources
Care Manager Development Care Management Resource Center - Web-based resource for care managers and POs National and local evidence-based training models Care management implementation guide Team Development Facilitated learning opportunities for practice teams Examples: Learning Collaboratives, webinars and seminars Physician Engagement “Town hall” meetings to be scheduled Profile success of physician/care manager partnerships

21
MiPCT Care Manager Training Details
Complex care manager training Partnership with Geisinger Health System Clinical leads: three weeks in Pennsylvania One week didactic training Two week preceptorship Care managers: One week didactic training in MI, ongoing webinars/support Moderate care manager training Chronic care model, self-management support MiPCT-approved programs identified throughout state

22
Year One MiPCT – Statewide Care Management Progress to Date
In 2012 over 350 Care Managers (CMs) hired and completed required training Building infrastructure in partnership with POs CM Work station at office practice location CM Documentation tools Process to bill for CM visits Ongoing Care Manager training, coaching, mentoring Patient education materials
 hired and completed required training. Building infrastructure in partnership with POs. CM Work station at office practice location. CM Documentation tools. Process to bill for CM visits. Ongoing Care Manager training, coaching, mentoring. Patient education materials.")
23
Year One MiPCT – Statewide Care Management Progress to date
Building Infrastructure cont. Delivery of Care Management at the practice level Staff members roles defined PCP referrals to Care Manager Communication- PCP, CM, staff members Building volume of G code and CPT codes submitted Care Managers are building caseloads Started with transitions of care for HCM, CCM Expand to enroll complex and moderate patients

24
Care Management Delivery by the Practice
PCMH meetings monthly, action plan, follow up PO and Practice Leadership Care Manager and PCP partnership Patient Office staff – defined roles and responsibilities Information technology, support Planned patient care i.e. huddles, processes, work flow, policies

25
2013 Priorities Care managers fully integrated into practices
Target PCMH interventions to patients from all participating payers Distribute multi-payer lists and Data dashboard reports Bill G-codes/CPT codes on BCBSM/BCN patients Use registry for proactive population management Focus on efficient and effective health care Avoid unnecessary services/hospitalizations Assess practice utilization patterns Ensure adequate clinic access to meet demands

26
MiPCT Team and PO Leaders Work Together to Define Care Management Activity
Define standard work Gather and share examples of standard work developed by POs and practices CCM Responsibilities with detailed description of processes and action step, available end of March Conduct “go sees” – ongoing by Master Trainers, Clinical Leads Gather and share best practice processes, resources, tools, staff job descriptions Continue to identify gaps – assist with developing solutions

27
MiPCT Transition of Care Intervention
Care Manager conducts Transition of Care follow up phone call within hours post hospital discharge Then weekly x 4 – phone visit Address: Medication reconciliation Follow up - PCP appt., specialist appt., tests Social support Assessment – barriers Red flags Access to PCP office – “how to”

28
MiPCT TOC Lessons Learned Primary Care Practice
Across the state practices continue to partner with hospitals to receive the discharge notification Notification to Primary care practices of hospital discharge varies widely: not occurring consistently Fax Electronic ADT Some MiPCT POs/practices are using IT resources to link the ADT to the MiPCT patient list – notifies Care Manager and practice real time It is ALL about relationships Care Managers, Practice Leaders and Physician Organization Leaders initiate communication across the continuum Hospitals – Discharge Planners, Care Managers Skilled Nursing Facilities Home Health Agencies Health Plan Care Managers

29
MiPCT Transition of Care (TOC) Workgroup
Areas identified to address High Volume of TOC Some care managers have high volume of patients discharged from the hospital Not able to consistently call every patient within hrs. post hospitalization Challenges balancing patient caseload: TOC, following up on new referrals, and managing caseload Some care managers are part time and/or support multiple practices Outcome of TOC work group: recommendation to risk stratify patients discharged from the hospital, continue work to define practice team members responsibilities Some care managers are including ER follow up phone visits Evidence based tool to stratify patients at high risk for hospital re-admission tool can be used in ambulatory care setting Care Manager is able to collect the data elements for the tool by reviewing the patient’s hospital discharge summary ease of use, time to complete - supports efficiency

30
Michigan Care Management Resource Center web site Public section Job Descriptions CCM, MCM MiPCT Implementation Guide Evidence based interventions, tools Private section for CCMs, HCMs CCMs and HCMs will receive User ID and Password upon completion of the MiPCT CCM course Contains Geisinger licensed tools

32
Contact Information Marie Beisel MSN, RN, CPHQ Office phone:

Similar presentations

 Project - Webinar #3 Complex Care Manager Training and Care Management Documentation Updates MiPCT Team.>")
 Project Annual Summit October 2013 MiPCT Overview and Updates 1.>")

 Project 2013 Annual Summit Sharing Care Management Best Practice & Building the Care Manager Caseload.>")


 Project All-Partner Launch Event March 13, 2012 1.>")





 Project: December PGIP Meeting Update MiPCT Team December 2, 2011 1.>")






