Download presentation
Presentation is loading. Please wait.

1
Nephrolithiasis and Urinary infections
Dr. Justin Hourmozdi, EM/IM-2 Henry Ford Hospital Emergency Medicine Grand Rounds November 13th 2014

2
Overview Diagnosis and acute management of nephrolithiasis
Urinary tract infections Uncomplicated UTI Complicated UTI Catheter Associated UTI Asymptomatic Bacteriruia UTI in Pregnancy

3
Basic anatomy

4
Kidney stones: Epidemiology
Prevalence: 13% North America Incidence: 7-12 cases per 10,000 persons 70-90% form calcium stones (primarily calcium oxalate). Others are uric acid, struvite and cystine stones.
. Others are uric acid, struvite and cystine stones.")
5
Kidney stones: Risk factors
History of previous kidney stones, obesity, HTN, DM, female, family history, metabolic disorders, myleoproliferative disorders, gastric bypass, high protein diet, dehydration

6
Kidney stones: Presentation
Flank or upper abdominal pain stones moving from renal pelvis to upper ureter Lower abdominal or groin pain lower ureter “colic”, peristalsis of ureter against stone and smooth muscle spasms, also temporary obstruction and distention of renal capsule Hematuria (usually microscopic), dysuria, N/V, gravel urine In a retrospective study of over 450 patients with CT- documented acute nephrolithiasis, hematuria was present in 95% on day one and 65-68% on days three and four
, dysuria, N/V, gravel urine. In a retrospective study of over 450 patients with CT- documented acute nephrolithiasis, hematuria was present in 95% on day one and 65-68% on days three and four.")
7
Kidney stones: DDx Remember to explore a thorough differential even with a classic presentation, especially if the patient is older or no previous history of kidney stones Vascular (acute renal artery occlusion or venous thrombosis, mesenteric ischemia, aortic syndromes), infectious (pyelonephritis, diverticulitis), GI (SBO, pancreatitis, gallbladder disease, appy), GU (ectopic, torsion, PID)
, infectious (pyelonephritis, diverticulitis), GI (SBO, pancreatitis, gallbladder disease, appy), GU (ectopic, torsion, PID)")
8
Kidney stones: CT vs US Multicenter RCT of 2759 patients visiting an ED with symptoms suggestive of nephrolithiasis, and in whom a serious alternative diagnosis was considered unlikely. Patients were randomly assigned to initial imaging with a CT, US performed by a radiologist, or bedside US by an EP. After the initial imaging test was complete, subsequent evaluation and care was at the discretion of the EP. US 54% sensitive (EP) vs 57% (radiologist) vs CT 88%. CT was eventually performed in 41% of those who initially had US performed. The rate of important missed diagnoses that resulted in complications (pyelonephritis or diverticular abscess) was similar and not statistically different between the groups (US=0.5% vs CT=0.3%), ages
 vs 57% (radiologist) vs CT 88%. CT was eventually performed in 41% of those who initially had US performed. The rate of important missed diagnoses that resulted in complications (pyelonephritis or diverticular abscess) was similar and not statistically different between the groups (US=0.5% vs CT=0.3%), ages")
9
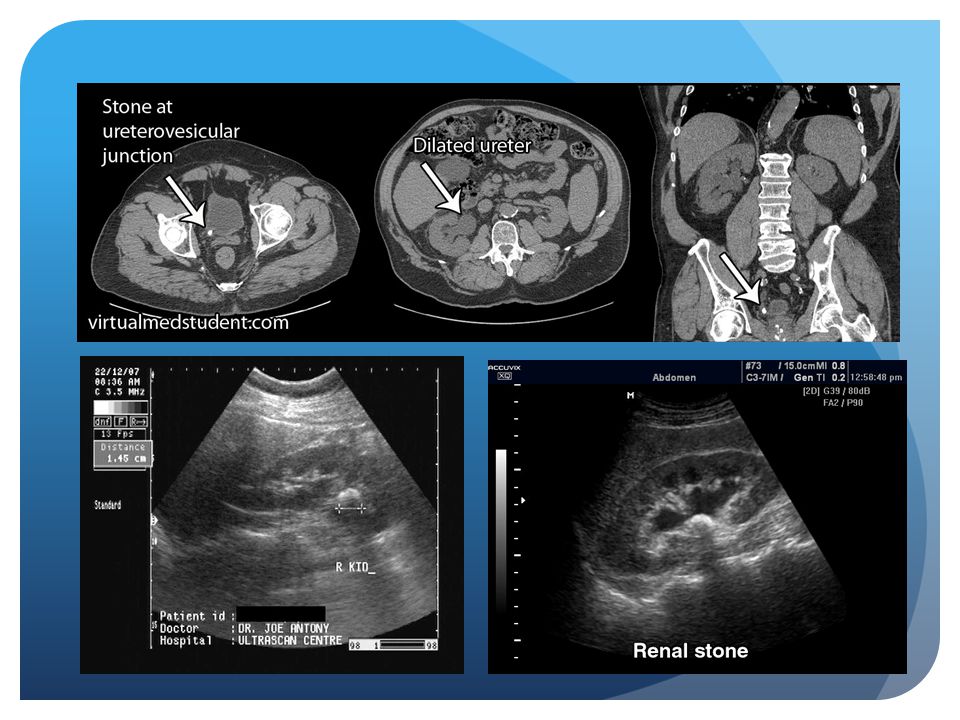
Kidney stones: Diagnosis
Labs: UA, urine preg, basic metabolic panel Imaging: ultrasound and non-contrast CT CT more sensitive than ultrasound but increased cost and radiation (low-dose renal protocol). The sensitivity and specificity of CT is 96-99%. Ureteral dilation on imaging without a stone could signify recent passage of stone
. The sensitivity and specificity of CT is 96-99%. Ureteral dilation on imaging without a stone could signify recent passage of stone.")
11
Kidney stones: Acute management
Pain management: NSAIDs>opioids, better in combination for severe pain, check Cr prior to NSAID prescription Fluids: IVFs if N/V, dehydrated, otherwise aggressive hydration does not improve pain or passage of stone Stone passage: <4mm most will spontaneously pass, >4mm PCP referral for trial a-blocker vs CCB, >9mm Urology referral for possible intervention (SWL vs ureteroscopy)
")
12
Kidney stones: Complications
Urgent urologic consultation is warranted in patients with obstruction, urosepsis, significant acute renal failure, anuria Admission for those with unyielding pain, N/V and inability to take PO medications

13
Approach? Relatively young or healthy person with appropriate history and PE, previous history of kidney stones, serious alternative diagnosis unlikely US, UA, Upreg, lytes (+US and +hematuria vs –US and +hematuria vs both -) Older, comorbidities, no history of previous kidney stones, considering alternative diagnoses CT, UA, lytes
 Older, comorbidities, no history of previous kidney stones, considering alternative diagnoses CT, UA, lytes.")
14
Urinary tract infections
Most common bacterial infection 7 million office visits, 1 million ED visit, 100,000 hospitalizations 1/3 women have 1 episode of UTI requiring antibiotics by 24 yo Annual cost of community acquired UTI: $1.6 billion Catheter associated UTI is most common nosocomial infection

15
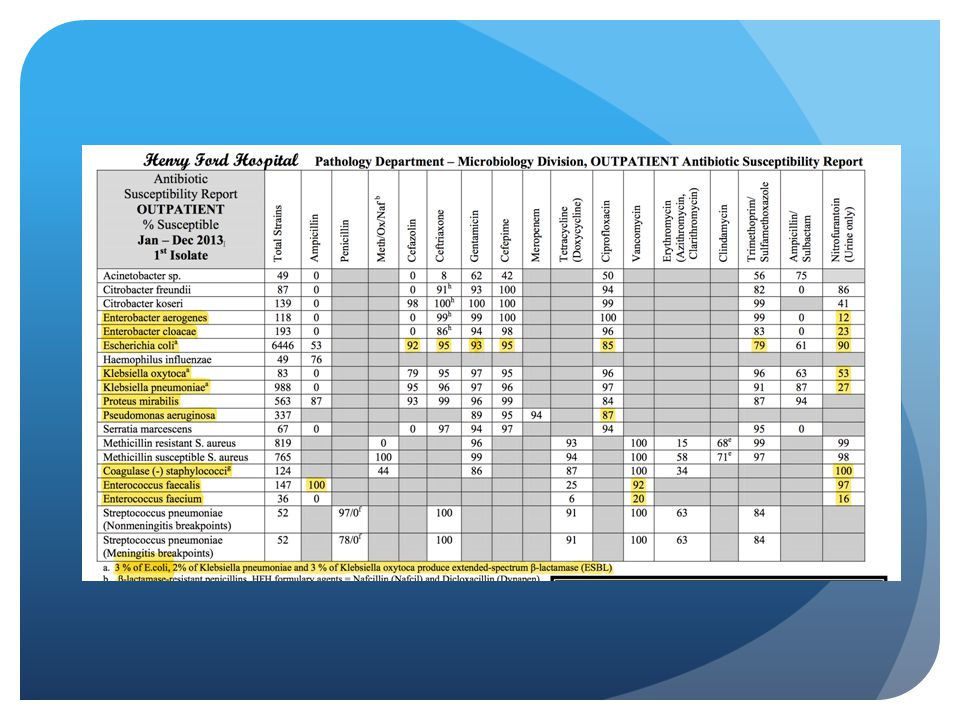
UTI: Microbiology E. Coli- 75-95% Staphylococcus saprophyticus- 5-15%
Young, sexually active females Proteus, Pseudomonas, Klebsiella and Eneterobacter More predominant in those with structural abnormalities, hospital acquired and nursing home patients Corynebacterium urealyticum Immunosuppressed and renal transplant patients Highly antimicrobial resistant but usually sensitive to Vanco Fungal (usually Candida) Indwelling catheter, bladder stasis, immunosuppressed
 Indwelling catheter, bladder stasis, immunosuppressed.")
16
UTI: Labs Laboratory Test Sensitivity Specificity Any coliforms 1.00
0.71 More than 100 coliforms per mL of urine 0.95 0.85 More than 8 WBC/mm3 0.91 0.50 More than 20 WBC/mm3 LE dipstick Nitrite dipstick Sterile pyuria: can occur in patients already taking anti-microbials, contamination fo the urine sample by vaginal leukocytes, chronic internstitial nephritis, nephrolithiasis, uroepithelial tumor

17
UTI: Uncomplicated Cystitis
Premenopausal, nonpregnant women with no urological abnormalities or comorbidities Absence of flank pain, fever, other signs of pyelonephritis Can one of the recommended antimicrobials below be used considering: Availability, Allergies, Tolerance, Local Resistance Patterns, Cost (if no then Cipro x3d or B-lactam except amoxicillin/amp x5-7d) Macrobid 100 mg BID x 5 days (avoid if early pyelo is suspected, contraindicated for CrCl<60) Bactrim 160/800 mg (one DS tab) BID x 3 days (avoid if resistance prevalence is known to exceed 20% or if used for UTI in previous 3 months) Fosfomycin 3 gm single dose (avoid if early pyelo is suspected) *If mild case of cystitis caused by ESBL: Macrobid or Fosfomycin
 Macrobid 100 mg BID x 5 days (avoid if early pyelo is suspected, contraindicated for CrCl<60) Bactrim 160/800 mg (one DS tab) BID x 3 days (avoid if resistance prevalence is known to exceed 20% or if used for UTI in previous 3 months) Fosfomycin 3 gm single dose (avoid if early pyelo is suspected) *If mild case of cystitis caused by ESBL: Macrobid or Fosfomycin.")
18
UTI: Uncomplicated Pyelonephritis
Premenopausal, nonpregnant women with no urological abnormalities or comorbidities. Presence of flank pain, fever, other signs of pyelonephritis Cipro 500 mg BID x 7 days *avoid if >10% resistance pattern, if >10%, an initial IV dose ceftriaxone or 24-h dose of an aminoglycoside is recommended (Level B) Bactrim 160/800 mg BID x days *if known prior susceptibility, if empiric, an initial IV dose of ceftriaxone or 24-h dose aminoglycoside is recommended (Level B) Hospitalized, 7-14 day tx: Cipro, Ceftriaxone, Cefepime, Zosyn, Aminoglycoside, Carbapenem depending on susceptibilities or suspicion
 Bactrim 160/800 mg BID x days *if known prior susceptibility, if empiric, an initial IV dose of ceftriaxone or 24-h dose aminoglycoside is recommended (Level B) Hospitalized, 7-14 day tx: Cipro, Ceftriaxone, Cefepime, Zosyn, Aminoglycoside, Carbapenem depending on susceptibilities or suspicion.")
19
UTI: Uncomplicated Pyelonephritis
Who do I image? Generally a clinical diagnosis, but scan if suspicion for complication (abscess, renal stone, obstruction), immunosuppressed/comorbidities, failure to respond to appropriate antibx after hours, or other possible significant diagnoses considered. Ultrasound or MRI if unable to have IV contrast. Always scan men.
, immunosuppressed/comorbidities, failure to respond to appropriate antibx after hours, or other possible significant diagnoses considered. Ultrasound or MRI if unable to have IV contrast. Always scan men.")
20
UTI: Complicated Cystitis and Pyelonephritis
Extremes of age, pregnant, or male (consider STIs or prostatitis) Anatomic or functional abnormalities of urinary tract, obstruction Concurrent kidney stone, foreign body (catheter, stents) Immunosuppressed, comorbid medical conditions Recent instrumentation, hospital acquired, h/o MDR organisms Pyelonephritis was complication (abscess, papillary necrosis) Severe sepsis, septic shock 1-2 week treatment course: Ceftriaxone, Cipro OR Cefepime, Zosyn, Aminoglycoside, Carbapenem depending on susceptibilities or suspicion Aminoglycoside: consider adding initial dose if severe sepsis/shock Vancomycin or Ampicillin: consider adding if suspect MRSA or enterococcus (NH/hospital acquired, indwelling catheter, elderly men/BPH, recent instrumentation or renal transplant)
 Anatomic or functional abnormalities of urinary tract, obstruction. Concurrent kidney stone, foreign body (catheter, stents) Immunosuppressed, comorbid medical conditions. Recent instrumentation, hospital acquired, h/o MDR organisms. Pyelonephritis was complication (abscess, papillary necrosis) Severe sepsis, septic shock. 1-2 week treatment course: Ceftriaxone, Cipro OR Cefepime, Zosyn, Aminoglycoside, Carbapenem depending on susceptibilities or suspicion. Aminoglycoside: consider adding initial dose if severe sepsis/shock. Vancomycin or Ampicillin: consider adding if suspect MRSA or enterococcus (NH/hospital acquired, indwelling catheter, elderly men/BPH, recent instrumentation or renal transplant)")
23
UTI: Elderly May be afebrile or have only a low grade temp; may also present with altered mental status, lethargy, or have generalized weakness. 20% of elderly patients with acute pyelonephritis have no fevers, predominant symptoms are generalized, GI or pulmonary

24
UTI: atheter Associated
Most common healthcare associated infection worldwide Approximately 20% of hospital-acquired bacteremias arise from the urinary tract, and the mortality associated with this condition is about 10% Risk factors: females, diabetes, age, duration of use, UTI in past 12 months, non-sterile technique, underlying neurological disease E Coli still most common, but increased rates of Pseudomonas, Proteus, Enterococcus, Staphylococcus and antibiotic resistance. A healthcare associated, or hospital acquired infection (nosocomial infection), is defined as an infetion that is not present when a patient is admitted to a hospital or healthcare facility. If the infection develops in patient 48 hours or more after admission to hospital or within 30 day after discharge. Duration of catherization is the most important risk factor; as 97% of UTIs in the ICU setting is associated with an indwelling urinary catheter; bacteruria develops at an average rate of 3-10% per day of catheterization w/ 26% of patients getting bacteriuria uin patient’s with a catheter in place for 2-10 days More than 3 risk factors associated with increased risk of having Candida, Klebsiella, or pseudomonas as the causative risk factor Most HAUTI associated with structural or functional abnormalities
, is defined as an infetion that is not present when a patient is admitted to a hospital or healthcare facility. If the infection develops in patient 48 hours or more after admission to hospital or within 30 day after discharge. Duration of catherization is the most important risk factor; as 97% of UTIs in the ICU setting is associated with an indwelling urinary catheter; bacteruria develops at an average rate of 3-10% per day of catheterization w/ 26% of patients getting bacteriuria uin patient’s with a catheter in place for 2-10 days. More than 3 risk factors associated with increased risk of having Candida, Klebsiella, or pseudomonas as the causative risk factor. Most HAUTI associated with structural or functional abnormalities.")
25
UTI: Catheter Associated
UTI symptoms: new onset or worsening of fever (most common symptom), SIRS, altered mental status, malaise, or lethargy with no other identified cause; flank pain or CVA tenderness; acute hematuria; pelvic discomfort. In those whose catheters have been removed, dysuria, urgent or frequent urination, or suprapubic pain. In patients with spinal cord injury, increased spasticity, autonomic dysreflexia, or sense of unease are also compatible with CA-UTI Culture: >/=103 cfu/mL of a single bacterial species in a single catheter urine specimen or urine specimen from a patient whose catheter has been removed within the previous 48 hrs A healthcare associated, or hospital acquired infection (nosocomial infection), is defined as an infetion that is not present when a patient is admitted to a hospital or healthcare facility. If the infection develops in patient 48 hours or more after admission to hospital or within 30 day after discharge. Duration of catherization is the most important risk factor; as 97% of UTIs in the ICU setting is associated with an indwelling urinary catheter; bacteruria develops at an average rate of 3-10% per day of catheterization w/ 26% of patients getting bacteriuria uin patient’s with a catheter in place for 2-10 days More than 3 risk factors associated with increased risk of having Candida, Klebsiella, or pseudomonas as the causative risk factor Most HAUTI associated with structural or functional abnormalities
, SIRS, altered mental status, malaise, or lethargy with no other identified cause; flank pain or CVA tenderness; acute hematuria; pelvic discomfort. In those whose catheters have been removed, dysuria, urgent or frequent urination, or suprapubic pain. In patients with spinal cord injury, increased spasticity, autonomic dysreflexia, or sense of unease are also compatible with CA-UTI. Culture: >/=103 cfu/mL of a single bacterial species in a single catheter urine specimen or urine specimen from a patient whose catheter has been removed within the previous 48 hrs. A healthcare associated, or hospital acquired infection (nosocomial infection), is defined as an infetion that is not present when a patient is admitted to a hospital or healthcare facility. If the infection develops in patient 48 hours or more after admission to hospital or within 30 day after discharge. Duration of catherization is the most important risk factor; as 97% of UTIs in the ICU setting is associated with an indwelling urinary catheter; bacteruria develops at an average rate of 3-10% per day of catheterization w/ 26% of patients getting bacteriuria uin patient’s with a catheter in place for 2-10 days. More than 3 risk factors associated with increased risk of having Candida, Klebsiella, or pseudomonas as the causative risk factor. Most HAUTI associated with structural or functional abnormalities.")
26
UTI: Catheter Associated
In the catheterized patient, pyuria is not diagnostic of CA-bacteriuria or CA-UTI, however it’s absence suggests an alternative diagnosis. Also the presence or absence of odorous or cloudy urine alone should not be used to differentiate CA-ASB from CA-UTI or as an indication for urine culture or antibiotics. “Purple urine bag syndrome”: color is due to blue and red metabolic products of biochemical reactions formed by bacterial enzymes in the urine, specifically Klebsiella, Proteus, and Proviencia spp If an indwelling catheter has been in place for >2 weeks at the onset of CA-UTI and is still indicated, the catheter should be replaced. The urine culture should be obtained from the freshly placed catheter and not the old catheter or the urine bag to avoid culturing bacteria present in the biofilm of the catheter but not in the bladder. A healthcare associated, or hospital acquired infection (nosocomial infection), is defined as an infetion that is not present when a patient is admitted to a hospital or healthcare facility. If the infection develops in patient 48 hours or more after admission to hospital or within 30 day after discharge. Duration of catherization is the most important risk factor; as 97% of UTIs in the ICU setting is associated with an indwelling urinary catheter; bacteruria develops at an average rate of 3-10% per day of catheterization w/ 26% of patients getting bacteriuria uin patient’s with a catheter in place for 2-10 days More than 3 risk factors associated with increased risk of having Candida, Klebsiella, or pseudomonas as the causative risk factor Most HAUTI associated with structural or functional abnormalities
, is defined as an infetion that is not present when a patient is admitted to a hospital or healthcare facility. If the infection develops in patient 48 hours or more after admission to hospital or within 30 day after discharge. Duration of catherization is the most important risk factor; as 97% of UTIs in the ICU setting is associated with an indwelling urinary catheter; bacteruria develops at an average rate of 3-10% per day of catheterization w/ 26% of patients getting bacteriuria uin patient’s with a catheter in place for 2-10 days. More than 3 risk factors associated with increased risk of having Candida, Klebsiella, or pseudomonas as the causative risk factor. Most HAUTI associated with structural or functional abnormalities.")
27
Asymptomatic bacteriuria: Definition
Women: bacteriuria is defined as 2 consecutive voided urine specimens with isolation of the same bacterial strain with >/=105 cfu/mL Men: A single voided urine specimen with 1 bacterial species isolated with >/=105 cfu/mL Both: A single catheterized urine specimen with 1 bacterial species isolated with >/= 102 cfu/mL

28
Asymptomatic bacteriuria: Treatment
Asymptomatic bacteriuria + pyuria = no treatment Asymptomatic bacteriruia in diabetics, nonpregnant women, elderly, neurogenic bladder, foley patients = no treatment Asymptomatic bacteriuria in pregnancy = treat (Macrobid x5d)
")
29
UTI: The Pregnant Patient
30-40% of untreated bacteriuria early in gestation develop symptomatic acute UTI including pyelonephritis Bacteriuria in pregnancy is associated with premature birth, low birth weight, preeclampsia, perinatal mortality Treatment for asymptomatic bacteriuria is usually started in women with ≥105 cfu/mL from a good clean-catch specimen Treat asymptomatic bacteriuria: Macrobid x5d, Keflex or Augmentin x 5-7 days, Fosfomycin 3g single dose Acute pyelonephritis: always admit; Ceftriaxone, Augmentin, Cefpodoxime x days Low threshold for renal ultrasound UTI can ascend quickly to pyelonephritis

30
Please feel free to email for complete references Thank you!

Similar presentations








: ITC3-1. * For Best Viewing: Open in Slide Show Mode Click on icon or From the View.>")











