Download presentation
Presentation is loading. Please wait.

1
Syphilis: Diagnosis and Treatment Veronica T. Soler MD Infectious Diseases Medical Director& Principal Investigator South Dakota AIDS Education and Training Center

2
Clinical Challenges: Syphilis Most providers have little experience in diagnosing syphilis Even in cities with syphilis outbreaks, most providers see few cases and under-diagnose Syphilis manifestations are protean, and easily misdiagnosed, particularly rashes, spots, lesions, CNS problems, eye disorders A high degree of clinical suspicion is necessary; routinely perform RPR serology's in high risk persons even if they are asymptomatic

3
Clinical Presentation: Clinical Stages of Syphilis Primary Stage- chancre- ulcerative lesion Secondary Stage- rash Tertiary- cardiovascular or gummatous Congenital Syphilis- oral defects, teeth and bone deformities; saber shins, Hutchinson's incisors Neuro-syphilis-eye symptoms and central nervous system problems Latent Syphilis – Early latent < 1 year – Late latent > 1 year

5
Latent Syphilis A period of time in which there may be no outward signs of infection Between primary and secondary stage, between secondary relapses, or after secondary stage Categories: – Early latent: < one year duration – Late latent: > one year duration

6
Diagnosis of Syphilis Treponema pallidum; has never been cultured. The organism can be viewed; indirectly via Dark Field Microscopy or directly via Fluorescent Microscopy. Serological testing is necessary for diagnosis. Multiple tests are often necessary in sequence. Services of reference laboratories and clinical experts are often needed. Both non-treponemal and treponemal serologies are involved and will be discussed.

7
MICROSCOPY Obtain a specimen by scraping the base of the ulcer/lesion and smearing the material on a microscope slide Place the slide and view directly under the dark field microscope- not readily available Apply antibody tagged fluorescent dye to the slide and observe under a fluorescent microscope- also not readily available

8
80% sensitive; varies with experience/skill of examiner ; decreased sensitivity as the lesion ages

9
Fluorescent Microscope: Demonstration of T. pallidum by using fluorescein-conjugated monoclonal antibodies It is the most specific test for the diagnosis of syphilis when lesions are present. Special microscope, and some specialized laboratory handling is required.

10
Syphilis Serology Non-treponemal tests: – RPR – VDRL Treponemal tests: – FTA-ABS – TP-PA – ELISA/Western Blot – Syphilis PCR- able to detect as low as one to 10 organisms per specimen with high specificity ; limited availability and not FDA approved

11
RPR/VDRL All non-treponemal tests measure both immunoglobulin IgG and IgM anti-phospholipid antibodies formed by the host in response to lipoidal material released by damaged host cells early in infection and lipids from the cell surface of the treponeme itself. Tests are reported as a qualitative result (RPR) and then as a quantitative titer (VDRL) which falls back to normal with successful cure. The RPR is reported as a positive or negative result. The VDRL is quantified and is followed serially from high titer to low or undetectable titer as the infection responds to treatment and resolves (cure).
 and then as a quantitative titer (VDRL) which falls back to normal with successful cure. The RPR is reported as a positive or negative result. The VDRL is quantified and is followed serially from high titer to low or undetectable titer as the infection responds to treatment and resolves (cure)..")
12
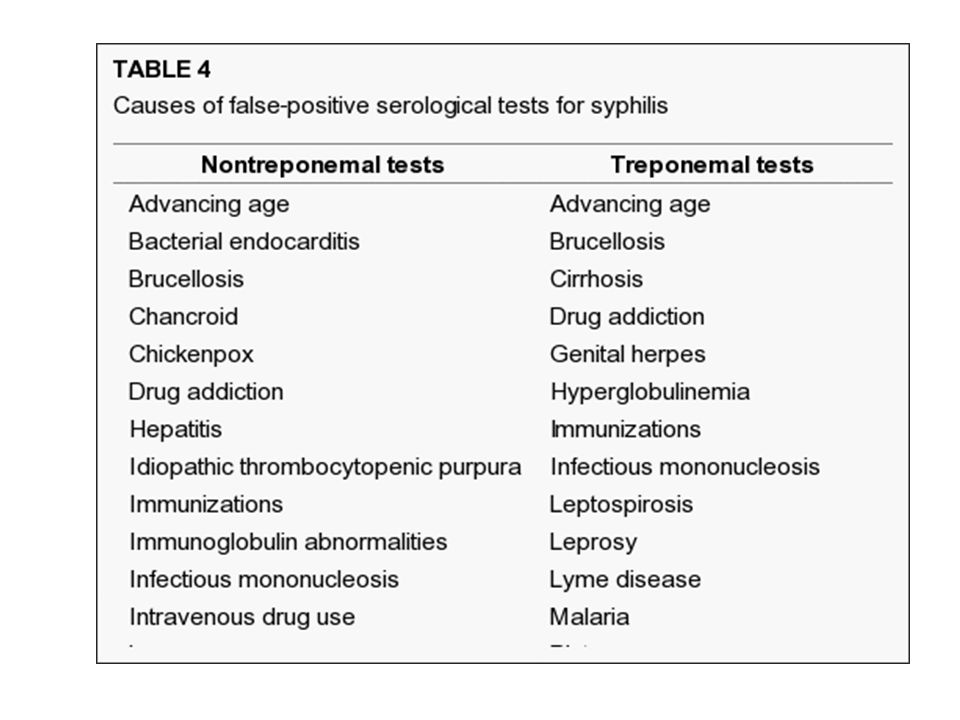
RPR/VDRL Non-treponemal serology A negative RPR does not exclude the diagnosis of syphilis; only ~75-85% sensitive in primary syphilis but 100% sensitive in secondary disease. The VDRL is quantified (example 1:32) and used to assess treatment response with four fold drop in titer indicative of treatment success These tests lack specificity (biologic false positives occur) all reactive tests need to be confirmed by a treponemal test for a definitive syphilis diagnosis
 and used to assess treatment response with four fold drop in titer indicative of treatment success These tests lack specificity (biologic false positives occur) all reactive tests need to be confirmed by a treponemal test for a definitive syphilis diagnosis.")
13
Potential Pitfalls of Non-treponemal tests False positives- the test is measuring something else that reacts with the reagin but is not syphilis.. False negatives- the test is not always positive in the very earliest phase of infection and sometimes reverts to negative in tertiary disease.

14
Benefits of Non-treponemal Tests Easy, inexpensive, fast (RPR). Can be quantified (titer) and degree of antibody levels can be measured (VDRL) The antibody titer drops with successful treatment and reverts to undetectable with successful treatment. The titer becomes positive again with re- infection or relapse of the infection.
 and degree of antibody levels can be measured (VDRL) The antibody titer drops with successful treatment and reverts to undetectable with successful treatment. The titer becomes positive again with re- infection or relapse of the infection..")
15
Treponemal Tests Measure specific antibodies to T. pallidum TP-PA test; The Treponema pallidum particle agglutination (TP-PA)- sensitive in primary syphilis, easy to perform FTA-ABS: sensitive in primary syphilis, complicated and expensive Treponemal EIA tests- detect serum antibodies to T. pallidum
- sensitive in primary syphilis, easy to perform FTA-ABS: sensitive in primary syphilis, complicated and expensive Treponemal EIA tests- detect serum antibodies to T. pallidum.")
16
Treponemal Serology FTA-ABS and others… Treponemal tests are used mainly as confirmatory tests to verify the reactivity in non-treponemal tests. However, in populations of low disease prevalence, treponemal tests can be used for screening. All positive patients would either be treated presumptively because the serious consequences of untreated infection far outweigh the effect of overtreatment, or have a follow-up RPR or VDRL to determine if they have active infection before treatment. Usually remain positive for life and are not useful to determine re-infection.

17
Diagnostic Flow Chart

22
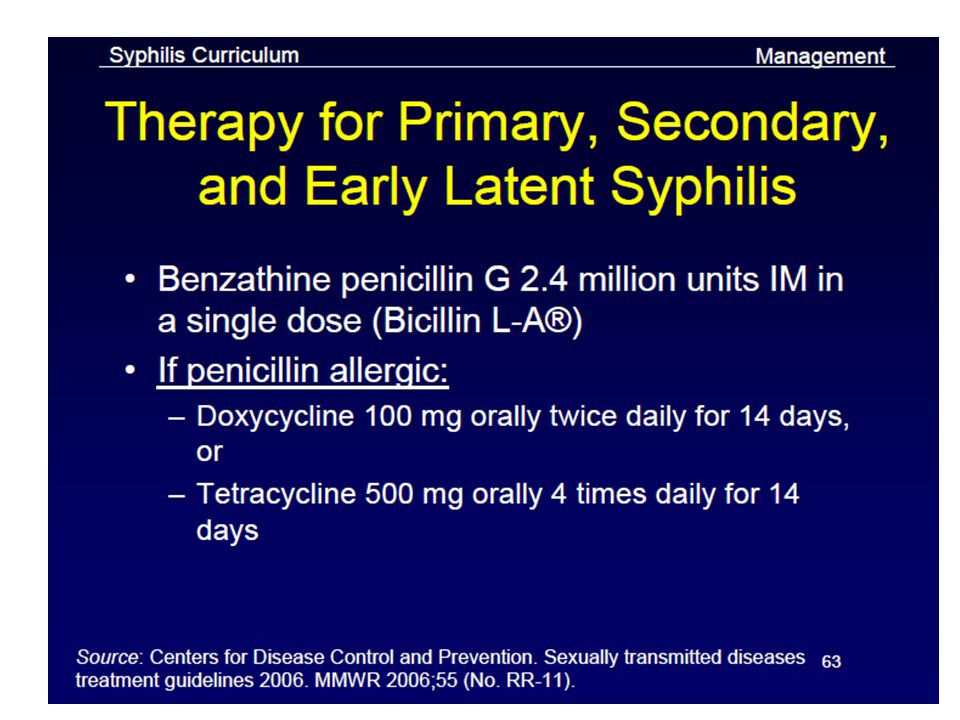
DO NOT CONFUSE Three IM PNC Preparations Penicillin G procaine: 600,000 units/mL (1 mL, 2 mL) Bicillin® C-R; Bicillin® C-R 900/300: Penicillin G benzathine and penicillin G procaine; 1.2 million units/mL (1mL, 2mL) Bicillin L-A: PNC G Benzathine: 600,000 units/mL (1 mL); 1,200,000 units/2 mL (2 mL); 2,400,000 units/4 mL (4 mL)
 Bicillin® C-R; Bicillin® C-R 900/300: Penicillin G benzathine and penicillin G procaine; 1.2 million units/mL (1mL, 2mL) Bicillin L-A: PNC G Benzathine: 600,000 units/mL (1 mL); 1,200,000 units/2 mL (2 mL); 2,400,000 units/4 mL (4 mL)")
26
Prevention “ an once is worth a pound” Detection of cases; consider it when you have skin sores, oral lesions, rash or any unusual situation: – Syphilis is the greatest mimic of all infectious diseases- “when you do not have a snowballs chance in hell send an RPR/VDRL”. Low threshold of testing; RPR/VDRL should be part of your STD/HIV bundle especially for pregnant, or at risk individuals. – HIV patients best practice is yearly RPR! – Treat presumptively for primary syphilis when in doubt. Risk reduction- condoms- remember this important prevention message to all sexually active persons. Partner notification and empiric treatment of all sexual contacts within 90 days. Syphilis is a reportable disease in all states. Syphilis is curable- treatment as prevention!

27
Contact Information: www.aidsetc.org Veronica Soler, MD PI and SD Medical Director DAETC vtsolermd@gmail.com Char Lowman Program Coordinator clowman@usd.edu Rita Shewmake SD Special Projects Coordinator ritashewmake@gmail.com

Similar presentations












 First epidemic in Europe in 15 century Incubation – 10-90 days (average.>")





 and two non->")




